Associations between individual and environmental factors and habitual physical activity among older Chinese adults:A social-ecological perspective
2016-10-24XingrenYiZhryPopeZnGoShumeiWngFngPnJingpengYnMengLiuPeipeiWuJingjingXuRuiWng
Xingren Yi*,Zhry Pope,Zn Go,Shumei Wng,Fng Pn,Jingpeng YnMeng Liu,Peipei Wu,Jingjing Xu,Rui Wng
aSchool of Physical Education,Shandong University,Jinan 250061,China
bSchool of Kinesiology,University of Minnesota Twin Cities,Minneapolis,MN 55455,USA
cSchool of Public School,Shandong University,Jinan 250061,China
dSchool of Medicine,Shandong University,Jinan 250061,China
Associations between individual and environmental factors and habitual physical activity among older Chinese adults:A social-ecological perspective
Xiangren Yia,*,Zachary Popeb,Zan Gaob,Shumei Wangc,Fang Pand,Jingpeng Yana,Meng Liuc,Peipei Wuc,Jingjing Xud,Rui Wangd
aSchool of Physical Education,Shandong University,Jinan 250061,China
bSchool of Kinesiology,University of Minnesota Twin Cities,Minneapolis,MN 55455,USA
cSchool of Public School,Shandong University,Jinan 250061,China
dSchool of Medicine,Shandong University,Jinan 250061,China
Purpose:To examine,within a social-ecological framework,associations between multifaceted individual and environmental factors and habitual physical activity(HPA)among older Chinese adults.
Methods:Through a mix of qualitative and quantitative methods,a survey instrument assessing various factors underlying 3 social-ecological dimensions of intrapersonal,interpersonal,and community and environmental resources was developed.Using a cross-sectional design,older adults(n=1580,aged 67±7 years)recruited from 10 communities in Shandong province completed the social-ecological survey of HPA.Data were analyzed using Partial Least Squares Path Modeling.
Results:Factors related to intrapersonal(medical knowledge,motivation,physical function,sport skills,socioeconomic status,and education),interpersonal(social support,social activity,and social norms),and community and physical environmental resources(safety,capacity,availability of and access to physical activity facilities)were found to be significantly associated with older adults’participation in HPA.
Conclusion:The findings provide an initial validation of a social-ecological approach to the study of HPA in China,suggesting that strategies aimed at promoting physical activity in older adults should address multiple levels of factors that may contribute to the likelihood of older Chinese adults being physically active.
©2016 Production and hosting by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Exercise;Interpersonal resources;Intrapersonal resources;Older adults;Physical activity;Social-ecological
1.Introduction
Increases in the length of life and reductions in fertility and mortality in China have contributed to a growing population of older Chinese adults,1with the number of individuals≥60 years old increasing from 194 million in 2012(14.3%of the total population)to 202 million in 2013(14.8%of the total population).2Thisincreaseintheolderadultpopulationhasbeen accompanied by a higher prevalence of non-communicable(chronic)diseases.3Itisestimatedthatabout64%ofindividuals aged 65 years and older have at least 1 chronic disease,creating public health and social/economic challenges to China.4In response,theMinistryofHealthofChinahasenactedbothshortandlong-termnationalplans(2012-2015)5inanefforttocontrol and prevent the increased incidence and prevalence of chronic diseases in this population,including diabetes,hypertension,heart disease,cancer,and arthritis.
Lifestyle factors such as physical inactivity are known to contribute to the development of many chronic diseases.6-8Therefore,there has been an increased research effort in the past decade in China aimed at identifying various individual,social,physical,and built environmental factors that promote an active and healthy aging process and,ultimately,reduce the incidence of chronic disease.9,10Mounting evidence suggeststhat habitual physical activity(HPA)is associated with numerous health benefits,including reductions in the risk of heart disease,diabetes,cancer,and osteoporosis.11-13Despite this evidence,most Chinese adults do not engage in regular physical activity(PA),and approximately 59%do not participate in any HPA.For the older adults,less than 30%participate in 30 min of PA 3 or more days/week.14Common correlates of or barriers to participation in HPA among Chinese adults include individual-level factors such as a lack of time and exercise equipment,15-17the lack of a social support system,18lack of motivation,19poor health/functional status,16busy with housework,20and low socioeconomic status.21In addition,various social and environmental correlates and determinants have also been identified as being related to PA adherence in older adults.22,23
Peer review under responsibility of Shanghai University of Sport.
http://dx.doi.org/10.1016/j.jshs.2016.06.010
2095-2546/©2016 Production and hosting by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
It is now recognized that there are multiple factors contributing to or correlating with participation in HPA.Thus,addressing this issue requires a multifaceted approach.In this regard,social-ecological models24,25provide a suitable framework for studying the complex interplay among individual,social,and community and environmental factors and the influences that interact and affect the ability of individuals to participate in PA or the likelihood of them doing so.26-31Evidence suggests that a social-ecological approach is effective in identifying and understanding various intrapersonal,interpersonal,community/ organizational,and environmental issues/resources that either enable or impede PA,thus influencing the health status of young and adult populations.32-43
In China,there is an obvious absence of research based on social-ecological models that focus on understanding the relationships among individual,social,and organizational/ environmental factors and PA in older Chinese adults,a population that faces increasing health and environmental challenges due to the unprecedented economic reform witnessed over the past 30 years.9Thus,the purpose of this study was to adopt a social-ecological framework in order to examine the associations between multifaceted individual and environmental factors and HPA in Chinese older populations.On the basis of past research,we hypothesized that social-ecological-based factors involving intrapersonal,interpersonal,and community and environmental resources would be related to participation in HPA among older Chinese adults.
2.Methods
2.1.Overview of the study design
The study was conducted between 2012 and 2014.The overall design involved a mix of qualitative and quantitative approaches carried out in 3 phases.In Phase 1,using a qualitative approach,we sought to develop a survey instrument specifically designed to test our study hypotheses.In Phase 2,using the information from Phase 1,we evaluated the initial factorial structure of the theoretical constructs entailed in our survey scale.In Phase 3,using the validated survey instrument,we empirically tested the hypotheses in a cross-sectional study.In all phases of the study,community-dwelling older adults were the target population.The study protocol was approved by the Institutional Review Board of Shandong University,and an informed consent was obtained from each participant.
2.2.Phase 1
The process of constructing the survey instrument included(1)a review of the existing research literature and(2)focus group meetings and interviews with local community stakeholders(i.e.,community leaders,administrators,resident representatives)and targeted community-dwelling older adults. The literature review included a synthesis of constructs derived from social-ecological-based studies and measures that involved assessments of intrapersonal/interpersonal and community/ environmental resources in PA.Focus group meetings,conducted by the researchers,involved discussions on topics and issues related to policies,social norms,safety,social activity,and community capacity and accessibility pertaining to older adults’PA.These preliminary efforts resulted in the generation of an initial pool of 115 survey items designed to assess various PA resources described below.
2.2.1.Intrapersonal
These items focused primarily on assessing individual characteristics such as health and medical knowledge,motivation,physical function,and sport skills.Items on health and medical knowledge were developed from the 2008 Chinese Citizens’Health Literacy Survey,44which includes questions about health habits,diabetes,and hypertension.Motivation(both intrinsic and extrinsic)was assessed via a Chinese version of the Motivation for Physical Activities Measure45(Cronbach’s internal consistency α=0.85).Physical function was assessed via the Chinese version of SF-3646(Cronbach’s α=0.66-0.94),with a high value indicating worse physical functioning.47Items related to sport skills were developed by a panel of experts in the areas of both traditional and conventional Chinese sport activities such as Tai Ji Quan,martial arts,table tennis,folk dance,badminton,gate ball,and walking.
2.2.2.Interpersonal
Interpersonal resources focused on dimensions of social support,social norms,and social connection.The social support measure developed by Eyler et al.48was adopted to assess both emotional and informational factors.Measures related to social safety and social connection were derived from the work by Sampson et al.49Finally,the Social Norms for PhysicalActivity Scale50was used to assess perceived norms at both the organizational/community level and individual level(e.g.,neighbor,family,or friends).
2.2.3.Community and environment
These resources focused on community capacity and physical environment.Specifically,community capacity was measured using items developed by Bush et al.51and assessed 4 areas:network partnerships,knowledge transfer,problem solving,and infrastructure.Items related to physical environment were developed via a mix of methods using input from focus groups,audits at local facilities on PA access,information on safety issues,information on programs offered,and interviews with stakeholders and older adults.
2.2.4.Initial scale construction
With the assistance of local community leaders,50 local community-dwelling older adults were interviewed individually to elicit their reactions to the clarity of the writing and content ambiguity in the survey items.Using a Delphi technique,the content of these items was further reviewed and scrutinized by a panel of 15 experts in the areas of public health,exercise instruction,PA research,sports psychology,and epidemiology. The responses from these panel members were examined,and a decision was then made on whether to modify,delete,or add items.During the process,items agreed upon by at least 80%of the panel members were included in a final version of the survey.As a result of these systematic content evaluations,a 100-item initial survey was developed for assessing the 3 general resources:intrapersonal,interpersonal,and community and environmental resources.
The 100 items were incorporated into 12 subscales that represented the different resources identified previously.A Likert-type response format was adopted for the survey.Specifically,scale items that measured intrapersonal and interpersonal resources were anchored on a 5-point scale ranging from 1(strongly disagree)to 5(strongly agree),whereas items measuring community and physical environment were anchored on a 4-point scale:1(not at all/very limited),2(somewhat),3(substantial),and 4(almost entirely/entirely).
2.3.Phase 2
2.3.1.Participants
A pilot study designed to evaluate the factorial structure of individualandenvironmentalresourceswasconducted among 400 older adults(65.36±5.68 years).The participants,recruited by resident representatives via telephone,were sampled randomly from a local telephone directory.The response rate of using the telephone recruitment method was 100%.The survey was administered to each participant by a group of local leaders and resident representatives.
2.3.2.Data analysis
Exploratoryfactoranalysis(EFA) wasperformed(SPSS18.0;SPSS Inc.,Chicago,IL,USA)to determine the underlying factorial structure of various resources identified in Phase 1.Since the scale was developed according to an a priori determined number of factors,the number of factors was fixed to 12 as identified by the α extraction and promax rotation.The criteria for retaining the factors were based on the eigenvalue being≥1.0 and a value of≥0.50 on factor loading.Under these criteria,7 items were removed.
The 12 factors underlying the 3 categories of resources included 5 factors that represented intrapersonal resources:individual characteristics(5 items,α=0.58),medical knowledge(4 items,α=0.71),motivation(18 items,α=0.77),physical functioning(14 items,α=0.68),and sport skill(PA type)(5 items,α=0.80).The next set of 3 factors represented interpersonal resources:social support(5 items,α=0.86),social norms(6 items,α=0.83),and social activity(4 items,α=0.88).The final set of 4 factors represented community and physical resources:safety(6 items,α=0.77),community capacity(18 items,α=0.81),facility(4 items,α=0.76),and PA programs(4 items,α=0.71).
2.4.Phase 3
2.4.1.Participants
The study sampling area covered the city of Jinan in Shandong province.Participants were recruited via a multistage sampling strategy.In the first stage,5 districts were randomly selected,and 2 neighborhoods from each district were then randomly chosen.With the assistance of local resident representatives,a total of 1613 older adults were contacted and invited to participate.Of these,33 decided not to participate,resulting in a response rate of 98%.The final sample consisted of 1580 participants(36.7%males,63.3%females)with ages ranging from 60 to 85 years old(67.11±7.77 years).
2.4.2.Procedure
The study survey was conducted in a local community setting and was administered by a group of graduate and undergraduate student assistants who were trained in the research and survey protocols.
2.4.3.Measures
Participants completed the survey instrument that was developed and evaluated in the first 2 phases of the study.In addition,participants’demographic information(i.e.,age,education,income)was obtained.As part of the survey,items on levels of PA were also included.Specifically,3 items were used to assess self-reported PA in older adults.Using a Yes/No response format,the first item asked whether the respondents participated in at least 150 min/week of PA.The second item assessed HPA frequency,which was anchored on a 4-point scale:1(no activity),2(1-2 times/week),3(3-4 times/week),and 4(5-6 times/week).Using the same scale,the last item assessed duration:1(less than 15 min),2(15-30 min),3(30-60 min),and 4(60-90 min).The items on frequency and duration were used in our structural model analysis.
2.4.4.Data analysis
To test the study hypotheses,Partial Least Squares Path Modeling(SmartPLSVersion2.0;SmartPLSGmbH,Boenningstedt,Germany)was used to examine,simultaneously,relationships among various individual and environmental factors and their associations with HPA among older Chinese adults.The model tested entails a measurement model(with observed variables that were related to their corresponding latent variables)and a structural model that links various individual and environment factors to HPA.The HPA latent factor was defined by the 2 items that measured HPA frequency and duration.The strength of the relationships is presented and evaluated by standardized path(or β)coefficients and their associated test statistics.A p value less than 0.05 was interpreted as reaching statistical significance.In addition,psychometric properties of each subscale were evaluated using variance explained(VE)and composite reliabilities(CR),employing the procedures described by Fornell and Larcker.52
3.Results
3.1.Study population characteristics
Demographic information about the study population is presented in Table 1.Overall,the sample was primarily female(63.3%),had a low level of education(90.2%had a high school degree or lower),and had a low level of income(68.9%had a monthlyincome≤RMB2000(aboutUSD300)).IntermsofHPA,approximatelyone-thirdoftheparticipantsreportedparticipatingat least 150 min/week of HPA.Though no gender difference(59.0% for men,61.9%for women)was found,HPA declined gradually with increasing age and was more prevalent among those who had an income level between RMB 1000 and RMB 3000.
3.2.VE and CR
Values of VE and CR for the survey scale are presented in Table 2.Reasonable variances were extracted by each construct,ranging from 0.55(physical function)to 0.65(social support). These variances represent the“amount of variance captured by the construct in relation to the amount of variance due to measurement error”(p.45).52Similarly,CR values ranged from 0.75 to 0.90,which was higher than recommended(i.e.,>0.70).52These estimates,collectively,indicate that the scale has an adequate convergent validity.
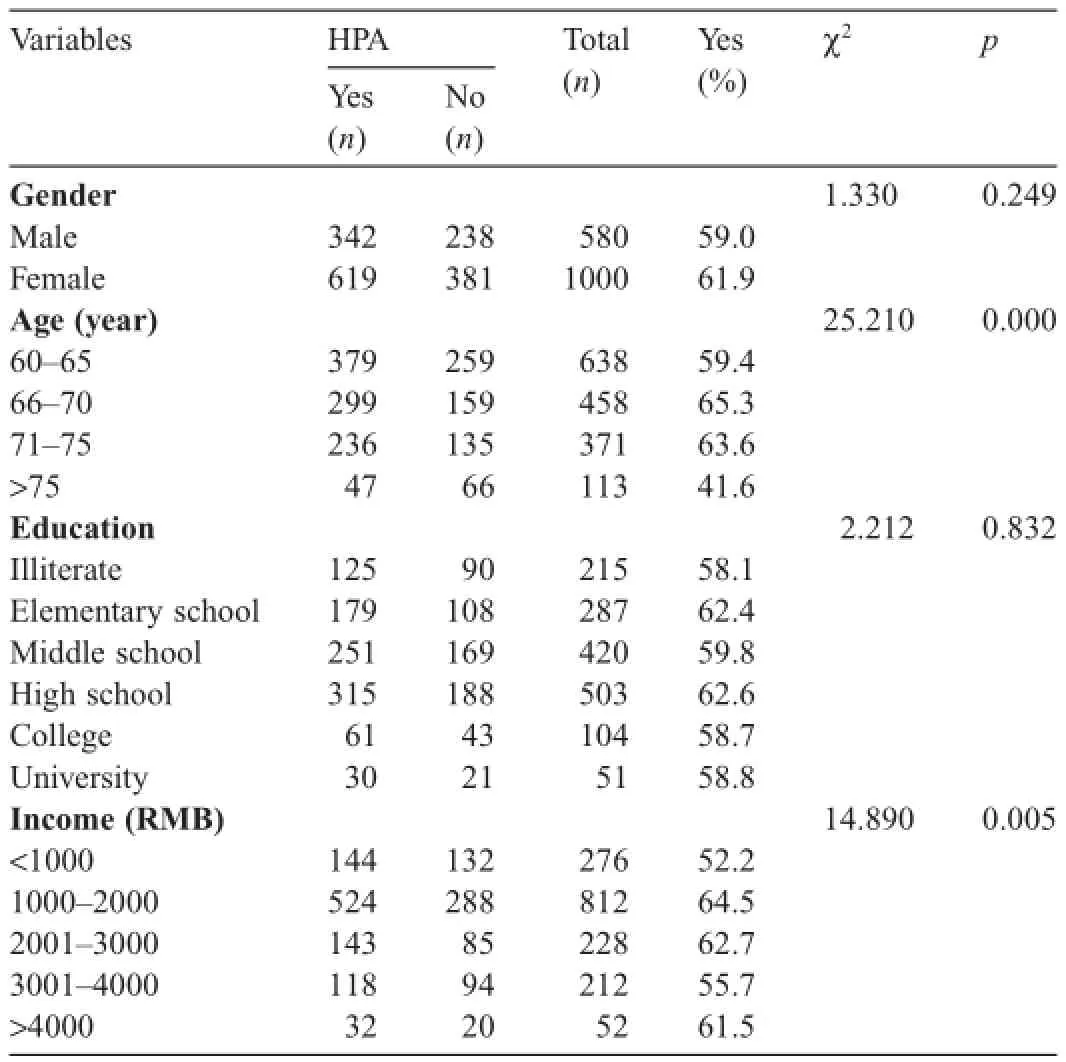
Table 1 Characteristics of the study population(n=1580).
3.3.Structural model
Modelestimatesforthehypothesizedstructuralrelationshipsare presented in Table 3.As can be seen,all latent variables were significantly associated with HPA.Specifically,perceptions of intrapersonal resources were,in general,positively related to participation in HPA among older Chinese adults.However,impaired physical function,which was negatively associated with HPA,reducedthelikelihoodofparticipatinginHPA.Forfactorsrelatedto interpersonal resources,the results show that older adults who had high levels of perceived social support and who followed social norms and participated in social activities were associated with a higherlevelofparticipationinHPA.Finally,forthecommunityand physical environmental factors,the results show that older adults whoperceivedhighlevelsofcommunitysafety,capacity,andaccess tolocalPAfacilitiesandprogramsweremorelikelytoreporthigher levels of HPA.

Table 2 Convergent validity of the survey scale.

Table 3 Path coefficients of the structural model.
4.Discussion
In this study,within the social-ecological framework,relationships between a set of individual and environmental factorsand participation in HPA among older Chinese adults were examined.Prior to the examination of the theoretical relationships under scrutiny,we used both qualitative and quantitative methods to develop a psychometrically sound survey instrument that allowed us to subsequently test the study’s hypothesized relationships.Results from structural equation modeling provide support for our working hypothesis that various theoretical factors underlying intrapersonal,interpersonal,and community and physical environmental resources are associated with older adults’participation in HPA.
With respect to factors related to intrapersonal resources,the results indicate that adequate medical knowledge regarding common diseases/conditions(e.g.,hypertension,diabetes),high levels of motivation,sport skills,socioeconomic status,and education were more likely to be associated with participation in HPA among older Chinese adults.Physical function,however,was negatively related to HPA,suggesting that older adults reporting limitations in physical function were likely to be physically inactive or underactive compared to those who reported no limitations.These findings are consistent with other reports that personal knowledge,attitudes,beliefs,and motivation are important in initiating and maintaining HPA.35,48On the influence of socioeconomic characteristics,our findings suggest that both socioeconomic status and level of education were associated with participation in HPA.These findings are consistent with a study from Jiaxing,China,indicating that adults having middle or high socioeconomic status tended to exercise more compared to those having lower socioeconomic status.21In regard to education,other studies have shown reduced PA among adults with low levels of education53and increased PA among those with high levels of education.33
Our findings also suggest the importance of interpersonal resources such as social support,social norms,and social activities in levels of HPA among older Chinese adults.These findings are congruent with the view that social support for HPA from neighbors,friends,family,and program staff is likely to facilitate HPA participation.54Although not specifically measured in the current study,it is likely that social support and social norms may affect PA indirectly through one’s perception of self-efficacy,55which has been shown to consistently predict PA.33,42,56Therefore,future studies should expand our current model to take into account the potential role of self-efficacy among older adults in mediating the relationships between social factors and HPA.Finally,engagement in social activities was also shown to correlate with HPA.This finding is consistent with a study conducted in Shanghai that demonstrated that older adults who participated in neighborhood-based social activities were likely to report higher levels of leisure time PA.34
Community-level factors were also shown to be important in regard to HPA participation among older Chinese adults.Our findings suggest that factors such as community safety,social activities,capacity,and availability and access to PA-related facilities were likely to be associated with increased levels of HPA among older adults.Past studies conducted both in China and other countries have consistently shown that positive social and built environmental features such as neighborhood safety,33,36,37,57high social cohesion33,34,37and engagement,34high walkability,37,58,59and availability of and accessibility to PA facilities33,36,57,58,60were associated with increased HPA or utilitarian PA(e.g.,walking for transportation).
4.1.Future research
Future efforts should focus on mechanisms through which some of the multilevel factors may either mediate or moderate HPA outcomes.For example,a study by McNeill et al.39suggests that individual perceptions of self-efficacy play an important role in mediating the relationships between social and physical environment and PA and that social support influences PA indirectly through one’s intrinsic and extrinsic motivation. Also,social and physical environments may interact with individual-level factors.For example,community resources may be important in facilitating HPA in older adults;however,individual factors such as self-efficacy,motivation,and physical function may influence people in using these available resources to engage in HPA.Finally,given that most PA takes place in social and built environments,29a multilevel approach is needed to delineate level-specific and cross-level influences of social and physical determinants of HPA.9,29This approach will allow us to identify potentially modifiable factors that can inform policies and facilitate the design of interventions to change PA behavior at the societal level.
4.2.Public health implications
There is an increasing need for PA programs in China in order to promote population health.9This study contributes to the sparse literature in the field of aging and PA in China by providing preliminary evidence regarding the important individual and social/physical environmental factors that may contribute to participation in HPA among older Chinese adults. Some of the important public health implications derived from this study include following:
(1)Olderadults’perceptionsaboutchronicdiseases/ conditions and physical function are important when designing community-based exercise and HPA programs.
(2)HPA may vary by socioeconomic characteristics,such as an individual’s income or education.Therefore,it is important to provide affordable and accessible PA facilities in promoting HPA in communities or neighborhoods with varying levels of socioeconomic status.
(3)Promotional strategies encouraging HPA need to maximize positive social support and enhanced cultural norms about the importance of HPA.This will create opportunities for engaging in meaningful community-based social activities for older adults.
(4)Salient social,physical,and built environmental factors are of high importance when promoting communitybased HPA among older adults.Community-living environments that are safe in regard to traffic and/or crime,that have good connectivity and are in close proximity to HPA facilities,that have capacity in mobilizing local HPA resources,and that have accessible facilities with rich PA programs are likely to encourage older adults to participate more frequently in HPA.
(5)Rather than focusing on individual-level factors,HPA programs and interventions are more likely to be successful and effective when they address multiple levels of factors or resources in a large social and community environment.
4.3.Strengths and limitations
This study has several strengths.First,it is one of the first studies that specifically evaluated the influences of individual and social/physical environmental factors on HPA among older Chinese adults.From this perspective,the study is significant because it addresses an important but relatively unexplored public health issue in the Chinese aging population.9Second,the study was hypothesis-driven and was built on a wellestablished social-ecological framework,thus providing scientific validation of this theoretical approach in the context of PA participation in China.Third,it uses both qualitative and quantitative approaches to understanding the influences of socialecological factors associated with participation in HPA among older adults.The qualitative component allowed us to provide a clear description of individual and contextual factors in naturalistic settings in order to gain a better understanding of conditions that influence HPA in older Chinese adults.
This study also has some significant limitations that may affect the generalizability of its findings.First,although the study’s cross-sectional design was useful in the preliminary stages of the project,it limits our ability to make causal inferences.Future longitudinal studies are needed to better understand how various factors influence PA participation over time. Second,like many other studies conducted in China,10notable limitations exist in our HPA measures in that(1)we used a generic assessment of PA domains and(2)the measures relied on self-reports,which are known to be subject to bias.Future studies should consider a combination of self-reports and objective assessment that entails various domains of PA(e.g.,leisure time PA,traditional Chinese sport activities,utilitarian walking/cycling).Finally,because of the multistage sampling,it is likely that clusters of participants recruited from the same district/neighborhood shared similarities in demographic and/or lifestyle characteristics that may have led to reduced variability in responses.Given that we analyzed the data at the individual level and did not take this clustering into account,this cluster sampling will not only impact standard errors of estimates but also reduce the power of the study.Therefore,future studies should consider proper adjustments for this clustering effect by using a multilevel modeling approach to the hierarchical data structure that is often encountered in community-based epidemiological studies.
5.Conclusion
This study provides an initial validation of a socialecological approach to the study of HPA among older Chinese adults.The findings suggest that public health intervention strategies aimed at promoting HPA in older adults should recognize multiple levels of influences that may either enhance or impede the likelihood of PA among older Chinese adults.
Acknowledgment
The work presented in this article was supported by grant from the Ministry of Science and Technology of China(2015FY111600).
XY participated in the design,data collection and analysis,and writing of the manuscript.ZP,ZG,SW,and FP participated in study design,data analysis and drafted the manuscript.JY,ML,PW,JX,and RW participated in design,collecting data,and coordination.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
None of the authors declare competing financial interests.
1.World Health Organization.China country assessment report on ageing and health.Available at:http://apps.who.int/iris/bitstream/10665/194271/ 1/9789241509312_eng.pdf;2015[accessed 09.06.2016].
2.National Council on Aging of China.China report on development of the cause of aging.Beijing:Social Science Documentation Publishing House;2013.[in Chinese].
3.The World Bank.Toward a healthy and harmonious life in China:stemming the rising tide of non-communicable diseases.Washington DC:World Bank;2011.Available at:http://www.worldbank.org/content/dam/ Worldbank/document/NCD_report_en.pdf;2011[accessed 09.06.2016].
4.China statistical yearbook 2010.Available at:http://www.stats.gov.cn/ tjsj/ndsj/2010/indexeh.htm;2010[accessed 09.01.2016].[in Chinese].
5.Ministry of Health of China.China national plan for NCD prevention and treatment(2012-2015).Availableat:http://www.chinacdc.cn/en/ne/ 201207/t20120725_64430.html;[accessed 10.06.2016].[in Chinese].
6.Blair SN,Brodney S.Effects of physical inactivity and obesity on morbidity and mortality:current evidence and research issues.Med Sci Sports Exerc 1999;31(Suppl.11):S646-62.
7.Durstine JL,Gordon B,Wang Z,Luo X.Chronic disease and the link to physical activity.J Sport Health Sci 2013;2:3-11.
8.Booth FW,Roberts CK,Laye MJ.Lack of exercise is a major cause of chronic diseases.Compr Physiol 2012;2:1143-211.
9.Li F.Physical activity and health in the presence of China’s economic growth:meeting the public health challenges of the aging population. J Sport Health Sci 2016;5:258-69.
10.Zhu W,Chi A,Sun Y.Physical activity among older Chinese adults living in urban and rural areas:a review.J Sport Health Sci 2016;5:281-6.
11.Bauman A,Merom D,Bull FC,Buchner DM,Fiatarone Singh MA. Updating the evidence for physical activity:summative reviews of the epidemiological evidence,prevalence,and interventions to promote“active aging”.Gerontologist 2016;56(Suppl.2):S268-80.
12.Bouchard C,Blair SN,Haskell WL.Physical activity and health. Champaign,IL:Human Kinetics;2007.
13.Dishman RK,Heath GW,Lee IM.Physical activity epidemiology. Champaign,IL:Human Kinetics;2013.
14.General Administration of Sport of China.Report for physical activity participation in Chinese citizen 2014.Available at:http://www.sport. gov.cn/n16/n1077/n1422/7300210.html; [accessed12.06.2016].[in Chinese].
15.General Administration of Sport of China.Report for physical activity participation in Chinese citizen 2007.Available at:http://zhuanti.sports. cn/dcgb/index.html;[accessed 10.06.2016].[in Chinese].
16.Wang D,Chen G.The influential factors of the elderly exercise in Beijing Chaoyang District.J Shenyang Sport Univ 2013;1:62-4.[in Chinese].
17.Wang H,Li X.The investigation of physical activity for elderly in Datong. Bull Sport Sci Technol 2010;18:77-81.[in Chinese].
18.Wang W.The sport demand and the social support system of the old adult in China.J Beijing Sport Univ 2007;11:1478-80.[in Chinese].
19.Fang Y,Ji L.Study on the physical exercise motivation of the old in China. J Beijing Sport Univ 2003;2:183-5.[in Chinese].
20.Gong C,Gong H,Sheng L,Han H,Chen X,Du X.Factors affecting on regular physical activity for old adult in Chengdu.Chin J Gerontol 2014;34:5219-21.[in Chinese].
21.Chen M,Wu Y,Narimatsu H,Li X,Wang C,Luo J,et al.Socioeconomic status and physical activity in Chinese adults:a report from a community-based survey in Jiaxing,China.PLoS One 2015;10:e0132918. doi:10.1371/journal.pone.0132918
22.Gao L,Wang X.Analysis of the factors of the physical activity for elderly in Nanjing.J Nanjing Inst Phys Educ 2005;19:26-30.[in Chinese].
23.Wang X,Lu S.Current condition and future trend of exercise life for elderly in Guangzhou.Sport Sci 2004;4:58-61.[in Chinese].
24.Bronfenbrenner U.Ecological models of human development.In:International encyclopaedia of education,vol.3.2nd ed.Oxford:Elsevier;1994.p.1643-7.
25.Glanz K,Rimer BK,Viswanath K.Health behavior and health education-theory,research and practice.4th ed.San Francisco,CA:John Wiley and Sons;2008.
26.Haselwandter EM,Corcoran MP,Folta SC,Hyatt R,Fenton M,Nelson ME.The built environment,physical activity,and aging in the United States:a state of the science review.J Aging Phys Act 2015;23:323-9.
27.Humpel N,Owen N,Leslie E.Environmental factors associated with adults’participation in physical activity:a review.Am J Prev Med 2002;22:188-99.
28.Li F,Fisher KJ,Bauman A,Ory MG,Chodzko-Zajko W,Harmer P,et al. Neighborhood influences on in middle-aged and older adults:a multilevel perspective.J Aging Phys Act 2005;13:87-114.
29.O’Donoghue G,Perchoux C,Mensah K,Lakerveld J,van der Ploeg H,Bernaards C,et al.A systematic review of correlates of sedentary behavior in adults aged 18-65 years:a socio-ecological approach.BMC Public Health 2016;16:163.doi:10.1186/s12889-016-2841-3
30.Saelens BE,Handy SL.Built environment correlates of walking:a review. Med Sci Sports Exerc 2008;40(Suppl.7):S550-66.
31.Vrazel J,Saunders RP,Wilcox S.An overview and proposed framework of social-environmental influences on the physical-activity behavior of women.Am J Health Promot 2008;23:2-12.
32.Ainsworth BE,Wilcox S,Thompson WW,Richter DL,Henderson KA. Personal,social,and physical environmental correlates of physical activity in African American women in South Carolina.Am J Prev Med 2003;25(Suppl.1):S23-9.
33.Fisher KJ,Li F,Michael Y,Cleveland M.Neighborhood-level influences on physical activity among older adults:a multilevel analysis.JAging Phys Act 2004;12:45-63.
34.Gao J,Fu H,Li J,Jia Y.Association between social and built environment and leisure-time physical activity among Chinese older adults-a multilevel analysis.BMC Public Health 2015;15:1317.doi:10.1186/s12889 -015-2684-3
35.Henderson K,Ainsworth B.A synthesis of perceptions about physical activity among older African American and American Indian women. Am J Public Health 2003;93:313-7.
36.Jia Y,Usagawa T,Fu H.The association between walking and perceived environment in Chinese community residents:a cross-sectional study. PLoS One 2014;9:e90078.doi:10.1371/journal.pone.0090078
37.King DK.Neighborhood and individual factors in activity in older adults:results from the neighborhood and senior health study.J Aging Phys Act 2008;16:144-70.
38.Li F,Harmer P,Cardinal BJ,Bosworth M,Acock A,Johnson-Shelton D,et al.Built environment,adiposity and physical activity in adults aged 50-75.Am J Prev Med 2008;35:38-46.
39.McNeill LH,Wyrwich KW,Brownson RC,Clark EM,Kreuter MWW. Individual social environmental and physical environmental influences in physical activity among black and white adults:a structural equation analysis.Ann Behav Med 2006;31:36-44.
40.Ng SW,Howard AG,Wang HJ,Su C,Zhang B.The physical activity transition among adults in China:1991-2011.Obes Rev 2014;15:27-36.
41.Sallis J,Johnson M,Calfas K,Caparosa S,Nichols J.Assessing the perceived physical environmental variables that may influence physical activity.Res Q Exerc Sport 1997;68:345-51.
42.Warner LM,Schüz B,Knittle K,Ziegelmann JP,Wurm S.Sources of perceived self-efficacy as predictors of physical activity in older adults. Appl Psychol Health Well-Being 2011;3:172-92.
43.Zang J,Ng SW.Age,period and cohort effects on adult physical levels from 1991 to 2011 in China.Int J Behav Nutr Phys Act 2016;13:40.doi:10.1186/s12966-016-0364-z
44.National Health and Family Planning Commission of China.Basic knowledge and skills in health literacy China residents.Beijing:Ministry of Health of PRC;2008.
45.Frederick CA,Ryan RM.Differences in motivation for sport and exercise and their relationships with participation and mental health.J Sport Behav 1993;16:124-46.
46.McHorney CA,Ware JE,Lu JFR,Sherbourne CD.The MOS 36-item short-form health survey(SF-36):III.Tests of data quality,scaling assumptions,and reliability across diverse patient groups.Med Care 1994;32:40-66.
47.Li L,Wang H,Shen Y.Development and psychometric tests of a Chinese version of the SF-36 health survey scales.ZhonghuaYu FangYi Xue Za Zhi 2002;36:109-13.[in Chinese].
48.Eyler AA,Baker E,Cromer L,King AC,Brownson RC,Donatelle RJ. Physical activity and minority women:a qualitative study.Health Educ Behav 1998;25:640-52.
49.Sampson RJ,Raudenbush SW,Earls F.Neighborhoods and violent crime:a multilevel study of collective efficacy.Science 1997;277:918-24.
50.Ball K,Jeffery RW,Abbott G,McNaughton SA,Crawford D.Is healthy behaviorcontagious:associationsofsocialnormswithphysical activity and healthy eating.Int J Behav Nutr Phys Act 2010;7:86.doi:10.1186/1479-5868-7-86
51.Bush R,Dower J,Mutch A.Community capacity index manual.Brisbane:Centre for Primary Health Care of Brisbane,Australia;2002.
52.FornellC,LarckerD.Evaluatingstructuralequationmodelswithunobservable variances and measurement errors.J Mark Res 1981;18:39-50.
53.Shaw B,Spokane LS.Examining the association between education level and physical activity changes during early old age.J Aging Health 2008;20:767-87.
54.Sallis J,Owen N.Physical activity&behavioral medicine.Thousand Oaks,CA:Sage Publications;1999.
55.Bandura A.Self-efficacy mechanism in human agency.Am Psychol 1982;37:122-47.
56.McAuley E,Blissmer B.Self-efficacy determinants and consequences of physical activity.Exerc Sport Sci Rev 2000;28:85-8.
57.Jáuregui A,Pratt M,Lamadrid-Figueroa H,Bernardo Hernández B,Rivera JA,Salvo D.Perceived neighborhood environment and physical activity:the international physical activity and environment network adult study in Mexico.Am J Prev Med 2016;51:271-9.
58.Sundquist K,Eriksson U,Kawakami N,Skog L,Ohlsson H,Arvidsson D. Neighborhood walkability,physical activity,and walking behavior:the Swedish Neighborhood and Physical Activity(SNAP)study.Soc Sci Med 2011;72:1266-73.
59.Siqueira Reis R,Hino AA,Ricardo Rech C,Kerr J,Curi Hallal P. Walkability and physical activity.Am J Prev Med 2013;45:269-75.
60.Eriksson U,Arvidsson D,Sundquist K.Availability of exercise facilities and physical activity in 2,037 adults:cross-sectional results from the Swedish neighborhood and physical activity(SNAP)study.BMC Public Health 2012;12:607.doi:10.1186/1471-2458-12-607
.
E-mail address:xrenyi@sdu.edu.cn(X.Yi)
s’contributions
3 May 2016;revised 4 June 2016;accepted 14 June 2016 Available online 29 June 2016
杂志排行

Journal of Sport and Health Science的其它文章
- Physical activity and health in the presence of China’s economic growth:Meeting the public health challenges of the aging population
- Physical activity and cognitive function among older adults in China:A systematic review
- Effects of Tai Ji Quan training on gait kinematics in older Chinese women with knee osteoarthritis:A randomized controlled trial
- Recruitment of older adults into randomized controlled trials:Issues and lessons learned from two community-based exercise interventions in Shanghai
- Exercise-induced rhabdomyolysis mechanisms and prevention:A literature review
- Scientific evidence is just the starting point:A generalizable process for developing sports injury prevention interventions