Physical activity and cognitive function among older adults in China:A systematic review
2016-10-24JiaojiaoWeijieFuYuLiu
Jiaojiao Lü,Weijie Fu,Yu Liu*
Key Laboratory of Exercise and Health Sciences of Ministry of Education,Shanghai University of Sport,Shanghai 200438,China
Physical activity and cognitive function among older adults in China:A systematic review
Jiaojiao Lü,Weijie Fu,Yu Liu*
Key Laboratory of Exercise and Health Sciences of Ministry of Education,Shanghai University of Sport,Shanghai 200438,China
Background:Physical activity(PA)has been shown to benefit cognitive function in older adults.However,the cognitive benefits of exercising for older Chinese adults have not been systematically documented.This study was to conduct a systematic review on evidence that PA is beneficial for cognitive functioning in older Chinese adults. Methods:Major databases,including PubMed,EMBASE,Cochrane Library,WanFang,CNKI,and VIP,were searched for studies published in English or Chinese between January 2000 and December 2015.Randomized and non-randomized controlled trials(RCTs and non-RCTs),cohort,case-control and cross-sectional studies that evaluated PA and cognitive function among older Chinese adults were included in this review. Results:Of 53 studies included and reviewed,33 were observational(22 cross-sectional,7 case-control,and 4 cohort)and 20 were experimental(15 RCTs,5 non-RCTs).Observational studies showed an association of reduced risk of cognitive-related diseases(i.e.,mild cognitive impairment,Alzheimer’s disease,and dementia)through PA,whereas experimental studies reported exercise-induced improvement in multiple domains of cognitive function(i.e.,global cognitive function,memory,executive function,attention,language,and processing recourse).
Chinese elderly;Cognition;Dementia;Exercise;Public health;Systematic review
1.Introduction
With the unprecedented economic reform taking place over the past 30 years,China has experienced a significant demographic transition.As a result of an increase in life expectancy and decades of implementing the one-child policy,the Chinese population is aging rapidly.1In 2014,it was estimated that in China there were about 212 million adults aged 60 and older,accounting for 15%of its total population.2Advancing age is associated with a high risk of decline in cognitive functioning and with an increase in both prevalence and incidence of neurodegenerative disorders,including Alzheimer’s disease(AD),vascular dementia,and dementia with Lewy bodies.3In an analysis of epidemiologic studies,the authors estimated that in 2010 the number of dementia cases in China was about 9.19 million(20%of the worldwide total),4with 30 million dementia cases predicted by 2050.5In the coming decades,various brainrelated diseases will begin to exert substantial health and economic burdens on Chinese society and the country’s health care system.6
China will undoubtedly continue to face the tremendous public health and socioeconomic challenges that accompany a rapidly aging population who suffers from late-life declines in cognitive function.However,research has shown that one-third ofAD cases worldwide(9.6 million)were attributable to modifiable risk factors,including physical inactivity.7In fact,studies have shown that physical activity(PA)may be neuroprotective in preventing age-related cognitive decline,reducing the incidence of mild cognitive impairment(MCI)and delaying the onset of dementia.8,9An increasing number of studies alsosuggest that PA may be effective in managing cognitive impairment and dementia.10
Peer review under responsibility of Shanghai University of Sport.
http://dx.doi.org/10.1016/j.jshs.2016.07.003
2095-2546/©2016 Production and hosting by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Although studies conducted in Western countries have shown that there are cognitive benefits to be gained from PA,there is a scarcity of scientific knowledge regarding the health benefits of PA on cognitive function in older Chinese populations.This may be due in part to the absence of systematic reviews of studies conducted in China that provide evidence on the influence of PA on cognition.Access to this information is of high public health importance given the increasing number of older Chinese adults and the continued upward trend in both prevalence and incidence of cognitive impairments in this population.The purpose of this article was to fill this knowledge gap by conducting a systematic review of empirical studies that have evaluated the health benefits of PA on cognitive function among older Chinese adults.
2.Methods
2.1.Data sources and search strategy
We conducted an extensive search using several major electronic databases.These included PubMed,EMBASE,Cochrane Library,WanFang,CNKI,and VIP.The search covered studies published in English or Chinese between January 2000 and December 2015.No other sources or search strategies were sought.A search of article titles and abstracts was conducted by the primary author.The keyword terms used in the search included“physical activity”,“exercise”,“running”,“walking”,“aerobic training”,“cycling”,“Tai Chi”or“Tai Ji”,“Qigong”,“cognition”,“brain”,“neuralplasticity”,“hippocampus”,“BDNF”,“dementia”,“Alzheimer”,“neurodegenerative”,“older adults”,“elderly”,“China”,“Chinese”,“Hong Kong”,and“Taiwan”.Review articles were also used as a source in a search for additional studies.
2.2.Inclusion and exclusion criteria
Eligible studies included 2 types:(1)experimental studies,comprising randomized controlled trials(RCTs)and nonrandomized studies(non-RCTs)and(2)observational studies(cross-sectional,case-control,and cohort).To be eligible,studies must have measured at least 1 cognitive domain and required at least 1 type of PA practiced by older adults(50 years and older)with or without cognitive impairment.Finally,eligible studies had to have been conducted in the Mainland of China,Hong Kong or Taiwan,China.
Studies were excluded if they(1)were published without an English title or abstract,(2)did not include a minimal-attention control condition(in the case of experimental studies),(3)were duplicates of other studies,(4)simply described research protocols,or(5)were review articles.
2.3.Data extraction
Two reviewers extracted data into a form that identified the study methodology and characteristics of each study.Categories included(1)sample,(2)design,(3)details of the outcome(i.e.,PA,cognitive function),(4)study duration,(5)intervention including intensity,frequency,and intervention duration,and(6)results.Data were extracted and synthesized separately for experimental studies and observational studies.No metaanalysis was conducted owing to significant variability in study design and methodologies.Instead,a narrative synthesis of all studies was produced.
2.4.Quality assessment
Because of the lack of a consistent instrument to assess methodological quality across studies having various designs,RCTs were the only studies in this review that were assessed using the core criteria from the Cochrane risk of bias assessment tool for RCTs.11Specifically,each RCT was rated initially using a binary coding scheme of 1(meeting the criteria)and 0(not meeting the criteria).The rating assessed 5 methodological components:sequence,allocation,blinding,intent-to-treat,and completeness in reporting prespecified study outcomes.RCTs that provided no information on any of these criteria were coded as“not meeting the criteria”.A numerical rating for meeting any of these criteria was tabulated and summarized into 3 quality ratings:low(those that met 1 or 2 criteria),moderate(those that met 3 criteria),and high(those that met 4 or 5 criteria).
3.Results
3.1.Search results and study characteristics
Overall,540 articles were identified using our search strategy;of these,487 were excluded from the review.A total of 53 studies met the inclusion and exclusion criteria(Fig.1)and were subsequently reviewed in full.Of the 53 studies reviewed,33 were observational(22 cross-sectional,7 case-control,and 4 cohort)and 20 were experimental(15 RCTs and 5 non-RCTs).
The characteristics of the studies included in the review are summarized,organized by study design,in Table 1(observational)and Table 2(experimental).Of the 53 studies,37 were conducted in the Mainland of China(23 observational(1 also took place in Hong Kong57),14 experimental),12 took place in Hong Kong,China(7 observational,5 experimental),and 5 were conducted in Taiwan,China(4 observational,1 experimental).Study sample sizes varied significantly,ranging from 135 to 27,651 participants(median=988)for observational studies and from 29 to 555 participants(median=84)for experimental studies.Although observational studies enrolled a mix of healthy older adults and those with cognitive impairment,most experimental studies(60%)targeted older adults with cognitive impairment(i.e.,MCI and dementia).
3.2.Quality assessment
A detailed quality assessment of 15 RCTs is summarized in Table 3.Per the quality assessment scheme used in this review,7 RCTs12-18(47%)were judged to be of high quality,1(6%)wasrated as moderate,19and 7(47%)were rated as being of low quality.20-26
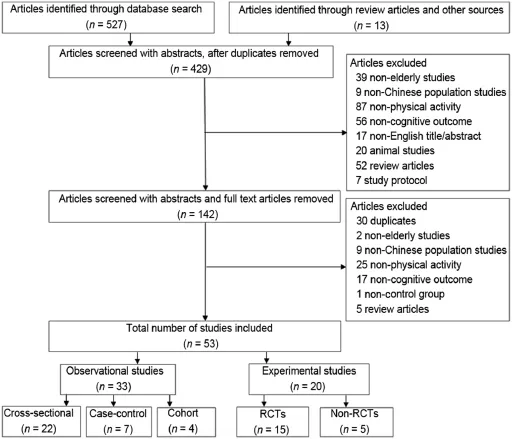
Fig.1.Flow diagram of study selection.Non-RCTS=non-randomized controlled trials;RCTs=randomized controlled trials
3.3.Results from observational studies
3.3.1.PA and risk of cognitive impairment
3.3.1.1.Mild cognitive impairment or cognitive impairment.A total of 13 studies reported an association between PA and MCI or cognitive impairment.27-39A cohort study with a 3-year follow-up showed that a lack of exercise in older women was associated with increased risk of cognitive impairment(odds ratio(OR)=2.2;95%confidence interval(CI):1.2-3.8).27In contrast,a number of studies showed that an increased level of PA was associated with low risk for MCI or cognitive impairment among older adults living in the Mainland of China,28-31,33-39Hong Kong,27and Taiwan,China.32Results from case-control studies also reported a reduced risk of MCI with a high level of PA(OR:0.382-0.570).30,38,39In addition,several cross-sectional studies reported a negative association between PA and the prevalence of MCI or cognitive impairment in older adults.28,29,31-37
3.3.1.2.AD.A total of 6 studies examined the association betweenPAandriskofAD.40-45Resultsfrom4case-controlstudies showed that older adults who engaged in PA were associated with a lower incidence ofAD.40-42,45For example,Yang et al.45reported thatahigherlevelofleisurePAwasassociatedwithalowerriskof AD(adjusted OR(AOR)=0.45;95%CI:0.30-0.68)and vascular dementia(AOR=0.38;95%CI:0.23-0.63).Incontrast,astudyby Hong et al.40showed that compared with healthy controls,older adults diagnosed with cognitive impairment who reported no time spent on daily PA were associated with an increased risk of AD(OR=1.68;95%CI:1.304-2.172).Cross-sectional studies showed that the complete absence of PA was related to an increasedAD prevalence(p<0.01)43and that a lack of PA in early life was associated with an increased likelihood of AD incidence(OR=2.537,p<0.001).44
3.3.1.3.Dementia.Three studies examined the relationship between PA and risk of dementia.46-48One cohort study with a 6-year follow-up showed that community-dwelling older adults who participated in 2 habitual PAs were associated with a low risk of developing dementia for aerobic exercise(OR=0.81;95%CI:0.68-0.95)and for mind-body exercises(OR=0.76;95%CI:0.63-0.92).46Two cross-sectional studies also reported that among highly educated older adults,a lack of PA was associated with dementia(OR=2.56;95%CI:1.18-5.84),47whereas regular exercise was associated with a decreased risk for dementia among community-dwelling older adults(OR=0.12;95%CI:0.09-0.16).48
3.3.2.PA and cognitive function
3.3.2.1.Global cognitive function.A total of 10 studies assessed the relationship between PA and global cognitive function.28,49-57One cohort study49with an 11-year follow-up showed an association between initial levels of PA and a slower decline in late-life global cognitive performance(β=0.22,p<0.05)and a positive relationship between changes in PA and changes in cognitive function during the long-term follow-up(β=0.36,p<0.05).Six cross-sectional studies28,50-54reported significant positive associations between older adults’PA and global cognitive function.For example,Lam et al.50showed that older adults with long-term exercise habits of performing aerobic and mind-body exercises had better cognitive test scores,including scores on the Mini-Mental State Examination(MMSE)andAlzheimer’s DiseaseAssessment Scale-cognitive subscale(ADAS-Cog),with a significantly better performance among young-old participants(65-75 years old).However,these findings were not consistent.For example,1 cohort with a 2-year follow-up55and 2 cross-sectional studies56,57showed no significant differences in global cognitive function measures between exercisers and nonexercisers.
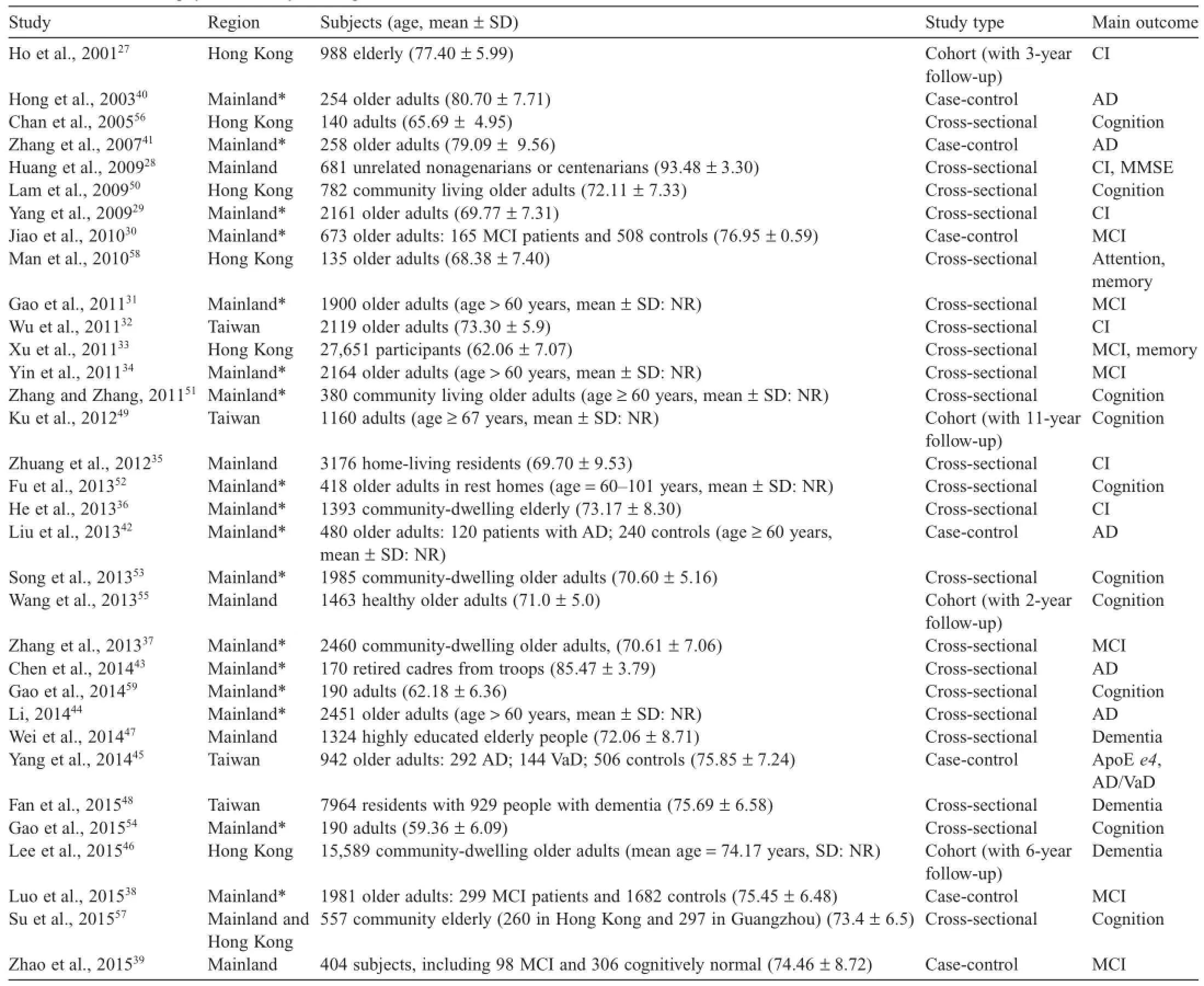
Table 1 Observational studies:physical activity and cognitive function.
3.3.2.2.Memory.The relationship between PA and memory was assessed in 7 studies.33,50,55-59One cohort study with a 2-year follow-up showed that a high level of PA was mildly associated with less decline in episodic memory among older adults(β=-0.08,p<0.05).55Six cross-sectional studies33,50,56-59reported better memory performance outcomes(e.g.,verbal memory,episodic memory)observed in the delayed recall test and digit and visual span test among older adults with higher levels of PA.
3.3.2.3.Executivefunction.Onecross-sectionalstudy57reported that the total amount of PA positively but mildly correlated with executive function in the Category Verbal Fluency Test(CVFT)(r=0.15,p<0.01)but not with the Trail Making Test(r=0.02,p>0.05).One cohort study55also showed no significant association between PA and executive function as measured by the Indiana University Tokens Test(β=0.04,p>0.05).

Table 2Experimental studies: physical activity and cognitive function.
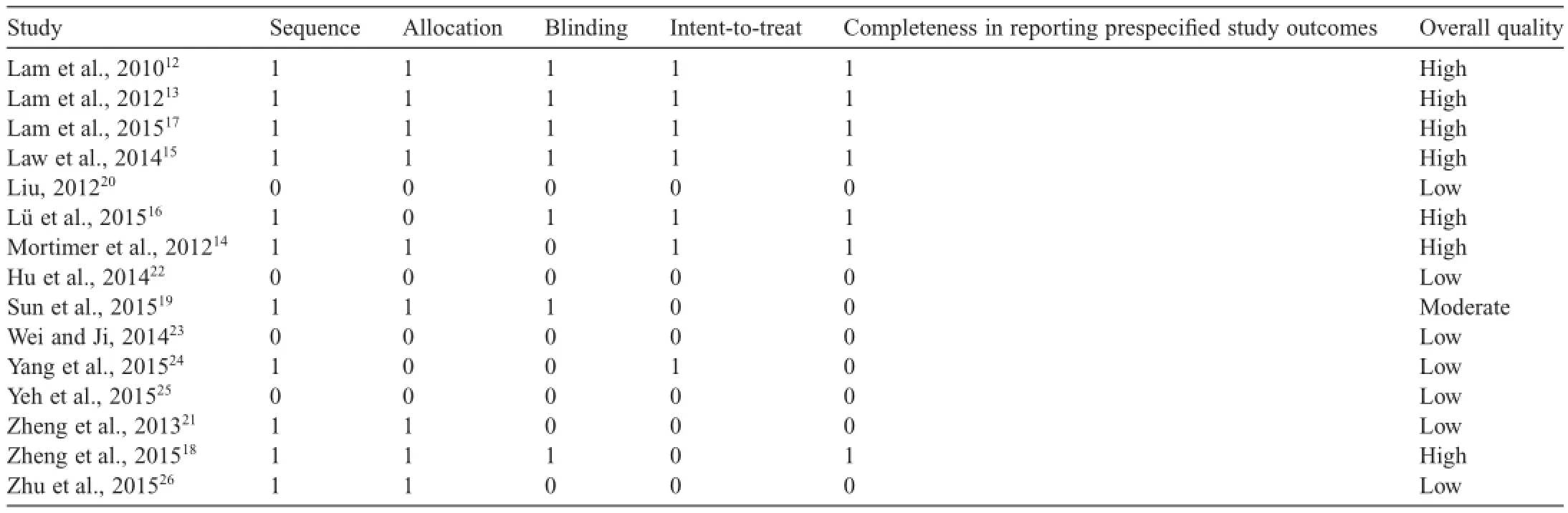
Table 3 Quality rating of randomized controlled trials.
3.3.2.4.Attention.Two cross-sectional studies50,58showed that healthy community-dwelling older adults participating in regular aerobic and mind-body exercises(e.g.,Tai Chi,yoga)showed better sustained and selective attention.However,these benefits were not supported in a cohort study in which PA was found not to be associated with attention among older adults living in Hong Kong,China and the Mainland of China.57
3.3.2.5.Language.Bothcohort55andcross-sectional50,57studies demonstrated a significant positive association between PA and verbal fluency as measured by the CVFT or the animal fluency test.However,in a cross-sectional study,56researchers from Hong Kong,China found that language function in older adults was weakly associated with PA.
3.3.2.6.Processing resource.Only 1 study examined PA and its relationship to processing resource in older adults.In a crosssectional study,Gao et al.59reported that older adults who regularly exercised tended to perform better in a number of cognitive processing outcome measures,including sensory function,processing speed,and reasoning and processing capacity.
3.4.Results from experimental studies
3.4.1.Aerobic exercise
Atotalof4studies(3non-RCTsand1RCT)conductedinthe MainlandofChinashowedthataerobicexercise,whencompared with a non-exercise control condition,resulted in a significant improvement in cognitive function(e.g.,global cognitive function,executive function,language)24,60-62and reductions in disease symptoms associated with AD.24For example,an RCT study reported by Yang et al.24showed that a 3-month cycling training regimen significantly reduced symptoms of dementia(as indexedbychange inADAS-Cog)and improved global cognitive functionandplasmaapoproteinA1levels.Inanon-RCTstudyof 150 healthy older adults,Zhang et al.62evaluated the health benefits of 4 different exercises(i.e.,swimming,running,square dancing,andTai Ji Quan)on cognitive function after a 12-month intervention.Compared with the control participants,participants in the exercise groups improved their event-related potential in the P300 test—a time-locked measure of electrical activity of the cerebral surface(as indexed by reduced P2,N2,and P3 latencies and response time).In addition,a stronger effect was observed among those who participated in the Tai Ji Quan exercise when compared with those assigned to other 3 exercise groups.Not all aerobic-based exercises were found to be effective in improving cognition.For example,1 RCT14involving a 40-week walking intervention showed no improvement in cognition among community-dwelling older adults.
3.4.2.Traditional Chinese exercises
3.4.2.1.Tai Ji Quan.Three RCTs13,14,19and 3 non-RCTs62-64evaluated the cognitive health benefits of Tai Ji Quan(or Taiji ball).14,19,62-65In an RCT,Mortimer et al.14showed that a 40-week Tai Ji Quan intervention in a sample of healthy communitydwelling older adults resulted in a significant increase in brain volume and improvements in cognitive function as indexed in several neuropsychological measures,including the Mattis Dementia Rating Scale,Trail Making Test,Auditory Verbal Learning Test,and CVFT.
Two other RCTs involving older adults with MCI also showed consistent results of cognitive benefits from Tai Ji Quan.13,22For example,in a 1-year study of 389 older adults with MCI,Lam et al.13showed that compared with those in a control group,participants in the Tai Ji Quan exercise group significantly lowered their risk of developing dementia(OR=0.21;p=0.04)and improved their delay recall.Similarly,Hu et al.22showed that a 6-month Tai Ji Quan intervention for older adults with MCI resulted in a significant improvement in immediate memory(p<0.001)and delayed recall(p=0.004)function.
3.4.2.2.Qigong.Three RCTs conducted in the Mainland of China showed the cognitive benefits of Qigong exercises(e.g.,Wu Qin Xi,Ba Duan Jin,and Six Healing Sounds).20,21,26,65One of these studies,a 6-month RCT,21showed that the Six Healing Sounds exercise significantly improved the global cognitive function(i.e.,in MMSE and Montreal Cognitive Assessment(MoCA))and electroencephalographic results among older adults with MCI.Two other RCTs involving patients with metabolic disease evaluated the effects of Wu Qin Xi and Ba Duan Jin exercises and showed improved cognitive outcomes(i.e.,inMMSE,MoCA,executive function,naming,attention,delay recall,and orientation).20,26
3.4.3.Specialized exercises
There were 4 specialized exercise interventions conducted with older adults who had MCI or dementia.These involved handballexercise,23functionaltasksexercise,12,15and momentum-based dumbbell training.16All 4 studies showed a significant improvement in cognitive function.For example,an RCT reported by Lü et al.16showed that a 12-week momentumbased dumbbell intervention significantly improved cognitive performance(i.e.,global cognitive function,executive function,immediate memory,and attention)in older adults with MCI.
3.4.4.Multimodal exercise-based interventions
There were 5 RCTs that used multimodal exercise-based or lifestyle interventions.17,18,22,25,61These modalities involved a combination of various types of exercises(e.g.,aerobic,strength,body-mind exercises)or activities related to cognitive health(e.g.,cognitive training,social interaction).One 48-week RCT17conducted in Hong Kong,China showed a significant improvement in ADAS-Cog,delayed recall test,and verbal fluency test. Another RCT conducted in Taiwan,China25also showed that a 12-week resistance exercise program combined with cognitive training significantly improved MoCA and its subscales(i.e.,naming,attention,delayed recall,and orientation).
The remaining 3 RCTs focused on a multicomponent exercise interventioninpatientswithMCI22andacognitivepsychological-physical intervention in healthy older adults.18,61Li and colleagues18,66,67showed that a 6-week cognitivepsychological-physical intervention was effective in maintaining a healthy brain and improving executive function.Using functional magnetic resonance imaging,the study also showed exercise-induced brain functional plasticity,including reorganizedregionalhomogeneityofspontaneousfluctuations,improved resting-state functional connectivity,and enhanced intrinsic brain activity in brain regions correlated with cognition.
4.Discussion
4.1.Summary of evidence
Over the past 15 years,a growing number of studies in China have examined the potential of PA for positively affecting cognitive health in older adult populations.This review has synthesized for the first time both observational and experimental studies that have contributed to our initial understanding of the relationship between PA and cognitive function among older Chinese adults.
Preliminary evidence presented in this systematic review suggests an important protective role of PA in preventing agerelated cognitive decline and improving cognitive function for healthy older Chinese adults and those with cognitive impairment.Findings from observational studies indicate that in general,physically active older Chinese adults,especially those with long-term engagement or participation in PA early in life, are likely to have a lower risk of cognitive impairment and have better cognitive health and cognitive performance later in life.40,45,46Similarly,some findings consistently indicate that exercise-based interventions can have a positive effect on lowering the risk of developing dementia and improving multiple domains of cognitive function,with the greatest benefits achieved through aerobic exercises24and traditional Chinese physical activities such as Tai Ji Quan.13,14
Although most studies have documented some positive associations or effects between PA and cognitive function,a few discrepancies in the findings were noted across both observational55-57and experimental studies.14These discrepancies can likely be attributed to differences in the selection of study populations,the type of PA or intervention,and/or methodological limitations.In addition,this review provides no evidence suggesting that the type,intensity,or frequency of various physical activities leads to a reduction in the incidence of MCI or AD or to improved cognitive function.
The limited number of studies examined,the wide range of sample sizes,the use of limited-exposure assessments and selfreport measures,and the lack of rigorously designed studies temper the findings described in this review.All these factors may have contributed to results that are not always consistent across different types of study design,settings,and interventions.In this respect,the interpretation and generalizability of the findings presented here may be limited to only a few of the studies that displayed a high degree of scientific rigor in their designs and methodologies.In addition,of the 33 observational studies reviewed here,a vast majority(n=22,67%)were crosssectional in design,making it impossible to infer causality. Similarly,only a few longitudinal studies on the relationship between PA and the incidence of cognitive impairment have been conducted in China.
Of the 15 RCTs reviewed,only a limited number were rigorously designed and were rated as being of high quality or showing low risk of bias.Many of the RCTs had notable limitations,including poorly defined clinical characteristics of study participants,poorly executed randomization procedures without proper concealment of allocation,an absence of interventions that specifically integrated a cognitive component with exercise training,and the small and often inadequately powered study sample sizes.These limitations make conducting metaanalyses and planning for the future quite difficult.
4.2.Future research
The evidence for the cognitive health benefits that older Chinese adults might gain from participating in PAs remains fragmented and inconclusive owing to the limited epidemiologic studies in this area and their lack of quality and scientific rigor.Given the increased life expectancy in China,1long-term cohort studies are needed to better understand the relationship between PA and development of MCI,AD,and other types of dementia.Differences in the types and levels of PA and their relative benefits for cognitive function should be examined across various ethnic groups,urban-rural settings,and gender. For example,data from a representative cross-section of theChinese population have shown clear differences in cognitive function between older men and older women,with larger declines observed for older women.68
Given the limited number of RCTs exploring the relationship between exercise and cognitive function,especially from the Mainland of China,additional trials are clearly needed to corroborate the findings reported in this review.Interestingly,aerobic and low-intensity exercises such as Tai Ji Quan or Qigong appear to offer great potential in preventing cognitive decline and delaying the onset of dementia or slowing down its progression.Intervention studies that target older adults who are at higher risk of developing AD and dementia are urgently needed.In addition,new interventions that combine exercise movements and cognition components that might stimulate brain health should be developed and tested.
4.3.Implications for public health
The findings described in this review provide initial evidence regarding the potential cognitive health benefits of PA for older Chinese adults.These findings,however,must be corroborated by future studies,especially RCTs.It is also important to conduct research on the type,intensity,and frequency of PA that is needed to produce the greatest cognitive health benefits. Given this lack of research and evidence,it is not possible to develop up-to-date public health guidelines that make dependable recommendations for specific PAs that will prevent cognitive decline.Nevertheless,the mounting evidence in the PA literature indicating that PA offers older adults multiple health benefits,69,70including improved cognitive function,71-73supports the idea that PA should be considered a primary prevention tool in maintaining normal cognitive function,preventing cognitive decline,and reducing the incidence of AD and dementia.
4.4.Limitations
This review has several limitations:(1)it is restricted to studies that were published within the past 15 years;(2)it may have omitted studies from the“gray”literature;and(3)it lacks an assessment of effect sizes.In addition,the quality assessment of the RCTs reviewed was limited in scope and depth. Future reviews should include a more detailed assessment of quality and include elements of design,analysis,and reporting of key information(i.e.,dropout rates and consistency and clarity in reporting trial outcomes).Given these methodological limitations,caution should be exercised when interpreting the synthesized results presented here.
5.Conclusion
This systematic review provides some initial evidence showing that PA is beneficial for the cognitive health of older Chineseadults.Additionalresearchisneeded,includingprospective studies examining relationships between PA and cognitive function over time and RCTs evaluating the efficacy of aerobicbased exercises specifically designed to preserve cognitive health in older Chinese adults and to slow down progression of cognitive decline in individuals with cognitive impairments.
Acknowledgment
The work presented in this article is supported by research grant from the National Natural Science Foundation of China(No.11372194).The authors thank Dr.Fuzhong Li for his help with the data synthesis and helpful advice and constructive comments during the various stages of writing this manuscript.
JL participated in design of the study,searched articles,extracted data,performed quality assessment,drafted the manuscripts,and approved the final manuscript.WF participated in the data extraction and read and approved the final manuscript.YL conceived of the study,participated in its design and helped to draft the manuscript.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
None of the authors declare competing financial interests.
1.World Health Organization.China country assessment report on ageing and health.Available at:http://www.who.int/ageing/publications/china -country-assessment/en/;[accessed 13.05.2016].
2.National Bureau of Statistics of China.Statistical communique on China’s 2014 national economic and social development.Available at:http://www.chinadaily.com.cn/business/2015-02/26/content_19660254.htm;[accessed 13.05.2016].
3.Yuan J,Zhang Z,Wen H,Hong X,Hong Z,Qu Q,et al.Incidence of dementia and subtypes:a cohort study in four regions in China.Alzheimers Dement 2016;12:262-71.
4.Chan KY,Wang W,Wu JJ,Liu L,Theodoratou E,Car J,et al. Epidemiology of Alzheimer’s disease and other forms of dementia in China,1990-2010:a systematic review and analysis.Lancet 2013;381:2016-23.
5.Prince M,Wimo A,Guerchet M,Ali GC,Wu YT,Prina M.World Alzheimer Report 2015.The global impact of dementia:an analysis of prevalence,incidence,cost and trends.London:Alzheimer’s Disease International;2015.
6.Keogh-Brown MR,Jensen HT,Arrighi HM,Smith RD.The impact of Alzheimer’s disease on the Chinese economy.E Bio Med 2015;4:184-90.
7.Norton S,Matthews FE,Barnes DE,Yaffe K,Brayne C.Potential forprimarypreventionofAlzheimer’sdisease:ananalysisof population-based data.Lancet Neurol 2014;13:788-94.
8.Blondell SJ,Hammersley-Mather R,Veerman JL.Does physical activity prevent cognitive decline and dementia?:a systematic review and meta-analysis of longitudinal studies.BMC Public Health 2014;14:510.doi:10.1186/1471-2458-14-510
9.Sofi F,Valecchi D,Bacci D,Abbate R,Gensini G,Casini A,et al.Physical activity and risk of cognitive decline:a meta-analysis of prospective studies.J Intern Med 2011;269:107-17.
10.Paillard T,Rolland Y,de Souto Barreto P.Protective effects of physical exercise in Alzheimer’s disease and Parkinson’s disease:a narrative review.J Clin Neurol 2015;11:212-9.
11.Higgins JP,Altman DG,Gotzsche PC,Juni P,Moher D,Oxman AD,et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials.BMJ 2011;343:d5928.doi:10.1136/bmj.d5928
12.Lam LCW,Lui VW,Luk DN,Chau R,So C,Poon V,et al.Effectiveness of an individualized functional training program on affective disturbances and functional skills in mild and moderate dementia—a randomized control trial.Int J Geriatr Psychiatry 2010;25:133-41.
13.Lam LC,Chau RC,Wong BM,Fung AW,Tam CW,Leung GT,et al.A 1-year randomized controlled trial comparing mind body exercise(Tai Chi)with stretching and toning exercise on cognitive function in older Chinese adults at risk of cognitive decline.J Am Med Dir Assoc 2012;13:568,e15-20.
14.Mortimer JA,Ding D,Borenstein AR,DeCarli C,Guo Q,Wu Y,et al. Changes in brain volume and cognition in a randomized trial of exercise and social interaction in a community-based sample of non-demented Chinese elders.J Alzheimers Dis 2012;30:757-66.
15.Law LL,Barnett F,Yau MK,Gray MA.Effects of functional tasks exercise on older adults with cognitive impairment at risk ofAlzheimer’s disease:a randomised controlled trial.Age Ageing 2014;43:813-20.
16.Lü J,Sun M,Liang L,Feng Y,Pan X,Liu Y.Effects of momentum-based dumbbell training on cognitive function in older adults with mild cognitive impairment:a pilot randomized controlled trial.Clin Interv Aging 2015;11:9-16.
17.Lam LC,Chan WC,Leung T,Fung AW,Leung EM.Would older adults with mild cognitive impairment adhere to and benefit from a structured lifestyle activity intervention to enhance cognition?:a cluster randomized controlled trial.PLoS One 2015;10:e0118173.doi:10.1371/journal.pone .0118173
18.Zheng Z,Zhu X,Yin S,Wang B,Niu Y,Huang X,et al.Combined cognitive-psychological-physical intervention induces reorganization of intrinsic functional brain architecture in older adults.Neural Plast 2015;2015:713104.doi:10.1155/2015/713104
19.Sun J,Kanagawa K,Sasaki J,Ooki S,Xu H,Wang L.Tai chi improves cognitive and physical function in the elderly:a randomized controlled trial.J Phys Ther Sci 2015;27:1467-71.
20.Liu H.Correlation research on effect of wuqinxi exercise on cognitive function in older people with metabolic syndrome.JWuhan Inst Phys Educ 2012;46:56-61.[in Chinese].
21.Zheng X,Yu J,Tu R,Sun S,Sun H,Wang X.Rehabilitation of“Six Healing Sounds”on MCI of the old-aged persons.Int J Tradit Chin Med 2013;35:968-72.[in Chinese].
22.Hu JP,Guo YH,Wang F,Zhao XP,Zhang QH,Song QH.Exercise improves cognitive function in aging patients.Int J Clin Exp Med 2014;7:3144-9.
23.Wei XH,Ji LL.Effect of handball training on cognitive ability in elderly with mild cognitive impairment.Neurosci Lett 2014;566:98-101.
24.Yang SY,Shan CL,Qing H,Wang W,Zhu Y,Yin MM,et al.The effects of aerobic exercise on cognitive function of Alzheimer’s disease patients. CNS Neurol Disord Drug Targets 2015;14:1292-7.
25.Yeh I,Chang CM,Chen KC,Hong WC,Lu YH.The influence of functional fitness and cognitive training of physical disabilities of institutions.Sci World J 2015;2015:686498.doi:10.1155/2015/686498
26.Zhu H,Zhang N,Ji C.Influence of Baduanjin on mild cognitive impairment in elderly diabetic patients.Chin J Pract Nurs 2015;31:1202-4.[in Chinese].
27.Ho SC,Woo J,Sham A,Chan SG,Yu AL.A 3-year follow-up study of social,lifestyle and health predictors of cognitive impairment in a Chinese older cohort.Int J Epidemiol 2001;30:1389-96.
28.Huang CQ,Dong BR,Zhang YL,Wu HM,Liu QX.Association ofcognitiveimpairmentwithsmoking,alcoholconsumption,tea consumption,and exercise among Chinese nonagenarians/centenarians. Cogn Behav Neurol 2009;22:190-6.
29.Yang Y,Chen CC,Li JM,Zhao JQ,Zhang FF.The relationship between daily exercise and the age-related cognitive impairment.Mod Prev Med 2009;36:2327,31.[in Chinese].
30.Jiao FB,Tan JP,Wang LN.A case-control study on psychosocial risk factors for mild cognitive impairment in elders.Chin J Contemp Neurol Neurosurg 2010;10:203-7.[in Chinese].
31.Gao LW,Jiang LL,Gao YZ,Nie HW,Xu Y.Prevalence of mild cognitive impairment and its risk factors among elderly people in Canglang district of Suzhou city.Occup Health 2011;27:2676-8.[in Chinese].
32.Wu MS,Lan TH,Chen CM,Chiu HC,Lan TY.Socio-demographic and health-related factors associated with cognitive impairment in the elderly in Taiwan.BMC Public Health 2011;11:22.doi:10.1186/1471-2458-11-22
33.Xu L,Jiang CQ,Lam TH,Zhang WS,Thomas GN,Cheng KK. Dose-response relation between physical activity and cognitive function:Guangzhou biobank cohort study.Ann Epidemiol 2011;21:857-63.
34.Yin SQ,Nie HW,Xu Y.The prevalence and risk factors of mild cognitive impairment among the aged in Huzhou.Chin J Pract 2011;14:4145-7.[in Chinese].
35.Zhuang JP,Wang G,Cheng Q,Wang LL,Fang R,Liu LH,et al.Cognitive impairment and the associated risk factors among the elderly in the Shanghai urban area:a pilot study from China.Transl Neurodegener 2012;1:22.doi:10.1186/2047-9158-1-22
36.He XY,Cao RF,Zhao GQ,Jiang QP,Luo Y,Wang YG,et al.A survey oncognitivefunctioninHangzhoucommunity-dwellingelderly:prevalence and associated factors.Zhejiang Prev Med 2013;25:8-10.[in Chinese].
37.Zhang JA,Jiang H,Wang FC,Gao LL.Investigation and analysis on mild cognitive impaiment among the elderly in the communities ofTaicang city. Pract Geriatr 2013;27:859-62.[in Chinese].
38.Luo X,Tang MN,Shen YE,Yu JC,Huang RY,Ren JJ,et al.Risk factors for mild cognitive impairment in community residents.Chin J Ceriatr Heart Brain Vessel Dis 2015;17:227-30.[in Chinese].
39.Zhao X,Yuan L,Feng L,Xi Y,Yu H,Ma W,et al.Association of dietary intake and lifestyle pattern with mild cognitive impairment in the elderly. J Nutr Health Aging 2015;19:164-8.
40.Hong Z,Zhou F,Huang MS,Zeng J,Ding D,Jin MH.Exercise and activity as protection factors of Alzheimer’s disease.Chin J Clin Rehabil 2003;7:24-5,43.[in Chinese].
41.Zhang YL,Huang HL,Zhou YS.A 1:1 matched case-control study on factors of Alzheimer’s disease.Chin J Contr Chron Non-commun Dis 2007;15:328-30.[in Chinese].
42.Liu XB,Yan JF,Zhou DS,Chen ZM.Lifestyle and risk of dementia:a case-study.Chin Pre Med 2013;14:171-4.[in Chinese].
43.Chen CT,Shi XQ,Zhang WZ,Zhang L.An investigation and analysis of Alzheimer’s factors affecting daily life of the special group.Mil Med J Southeast China 2014;16:171-3,211[in Chinese].
44.Li QP.Analyze and study the regional infection situation of Alzheimer’s disease.J ZheJiang Chin Med Univ 2014;38:654-6.[in Chinese].
45.Yang SY,Weng PH,Chen JH,Chiou JM,Lew-Ting CY,Chen TF,et al. Leisure activities,apolipoprotein E e4 status,and the risk of dementia. J Formos Med Assoc 2014;114:1216-24.
46.Lee AT,Richards M,Chan WC,Chiu HF,Lee RS,Lam LC.Intensity and types of physical exercise in relation to dementia risk reduction in community-living older adults.J Am Med Dir Assoc 2015;16:899,e1-7.
47.Wei CJ,Cheng Y,Zhang Y,Sun F,Zhang WS,Zhang MY.Risk factors for dementia in highly educated elderly people in Tianjin,China.Clin Neurol Neurosurg 2014;122:4-8.
48.Fan LY,Sun Y,Lee HJ,Yang SC,Chen TF,Lin KN,et al.Marital status,lifestyle and dementia:a nationwide survey in Taiwan.PLoS One 2015;10:e0139154.doi:10.1371/journal.pone.0139154
49.Ku PW,Stevinson C,Chen LJ.Prospective associations between leisure-time physical activity and cognitive performance among older adults across an 11-year period.J Epidemiol 2012;22:230-7.
50.Lam LC,Tam CW,Lui VW,Chan WC,Chan SS,Chiu HF,et al.Modality of physical exercise and cognitive function in Hong Kong older Chinese community.Int J Geriatr Psychiatry 2009;24:48-53.
51.Zhang J,Zhang JH.Analyses on influencing factors of cognitive function of the aged in city.J Shanxi Med Coll Contin Educ 2011;21:62-5.[in Chinese].
52.Fu JM,Sun SD,Pang W,Tan L,Li HQ,Zhang Y,et al.The study of correlation between physical activity and cognitive function in elderly residents.Chin J Prev Contr Chron Dis 2013;21:22-5.[in Chinese].
53.Song YJ,Zhang BL,Li JY,Li XH,Shang L,Li J,et al.Survey of cognitive impairment and associated factors for the elderly in community in Beijing. Chin J Rehabil Theory Pract 2013;19:583-5.[in Chinese].
54.Gao X,Chai J,Meng Y.Positive effects of physical exercise on cognitive function of the elder:based on the checking of psychological intermediary model of attitude toward aging and general self-efficacy.J Shenyang Sport Univ 2015;34:7-12.[in Chinese].
55.Wang HX,Jin Y,Hendrie HC,Liang C,Yang L,Cheng Y,et al.Late life leisure activities and risk of cognitive decline.J Gerontol A Biol Sci Med Sci 2013;68:205-13.
56.Chan AS,Ho YC,Cheung MC,Albert MS,Chiu HF,Lam LC.Association between mind-body and cardiovascular exercises and memory in older adults.J Am Geriatr Soc 2005;53:1754-60.
57.Su EX,Lin YQ,Zhang SL,Leung GT,Lam LC,Chiu HF.Physical activity and cognitive function of community Chinese elderly in Hong Kong(HK)and Guangzhou(GZ).Int Psychogeriatr 2015;27:959-66.
58.Man DW,Tsang WW,Hui-Chan CW.Do older t’ai chi practitioners have better attention and memory function?J Altern Complement Med 2010;16:1259-64.
59.Gao SQ,Mao ZX,Zhang LC.Psychological mechanism of physical exercise delaying aging of primary mental ability:mediation model of cognitive processing resources.J Tianjin Univ Sport 2014;29:461-6.[in Chinese].
60.Cao M,Wei WS.Clinical research intervention of rule physical exercise on mild cognitive dysfunction in the elderly.Ceriatr Health Care 2012;18:173-4.[in Chinese].
61.Liu JW,Wei SM.Effect of different leisure activities on the intellectual levels of elderly.Mod Prev Med 2013;40:3801-4.[in Chinese].
62.Zhang X,Ni X,Chen P.Study about the effects of different fitness sports on cognitive function and emotion of the aged.Cell Biochem Biophys 2014;70:1591-6.
63.Cui J,Yang L.Effects of taiji ball on the estrogen,muscle strength and cognitive function of the aging women.China Sport Sci Technol 2012;48:108-12.[in Chinese].
64.Kwok TCY,Lam KC,Wong PS,Chau WW,Yuen KSL,Ting KT,et al. Effectiveness of coordination exercise in improving cognitive function inolderadults:aprospectivestudy.ClinInterv Aging2011;6:261-7.
65.Guo Y,Shi H,Yu D,Qiu P.Health benefits of traditional Chinese sports and physical activity for older adults:a systematic review of evidence.J Sport Health Sci 2016;5:270-80.
66.Li R,Zhu X,Yin S,Niu Y,Zheng Z,Huang X,et al.Multimodal intervention in older adults improves resting-state functional connectivity between the medial prefrontal cortex and medial temporal lobe.Front Aging Neurosci 2014;6:39.doi:10.3389/fnagi.2014.00039
67.Yin S,Zhu X,Li R,Niu Y,Wang B,Zheng Z,et al.Intervention-induced enhancement in intrinsic brain activity in healthy older adults.Sci Rep 2014;4:7309.doi:10.1038/srep07309
68.Smith JP,Strauss J,Zhao Y.Healthy aging in China.J Econ Ageing 2014;4:37-43.
69.Nelson ME,Rejeski WJ,Blair SN,Duncan PW,Judge JO,King AC,et al. Physical activity and public health in older adults:recommendation from the American College of Sports Medicine and the American Heart Association.Circulation 2007;116:1094-105.
70.World Health Organization.Physical activity and older adults.Available at:http://www.who.int/dietphysicalactivity/factsheet_olderadults/en/;2011[accessed 13.05.2016].
71.Bherer L,Erickson K,Liu-Ambrose T.A review of the effects of physical activity and exercise on cognitive and brain functions in older adults.J Aging Res 2013;2013:657508.doi:10.1155/2013/657508
72.Carvalho A,Maeve Rea I,Parimon T,Cusack BJ.Physical activity and cognitive function in individuals over 60 years of age:a systematic review. Clin Interv Aging 2014;9:661-82.
73.Larson EB,Wang L,Bowen JD,McCormick WC,Teri L,Crane P,et al. Exercise is associated with reduced risk for incident dementia among persons 65 years of age and older.Ann Intern Med 2006;144:73-81.
s were downloaded into an Excel spreadsheet and assessed for relevance against the prespecified inclusion and exclusion criteria(described later).Full-text articles were obtained for all studies entering the review.Any uncertainties or discrepancies about entering the review were resolved by consensus and,if necessary,by a third reviewer.
.
E-mail address:yuliu@sus.edu.cn(Y.Liu).
s’contributions
26 March 2016;revised 30 April 2016;accepted 14 May 2016 Available online 11 July 2016
Conclusion:This systematic review provides initial evidence that PA may benefit cognition in older Chinese adults.Further studies of individuals with cognitive impairments and prospective and RCT studies having high scientific rigor are needed to corroborate the findings reported in this review.
©2016 Production and hosting by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
杂志排行

Journal of Sport and Health Science的其它文章
- Physical activity and health in the presence of China’s economic growth:Meeting the public health challenges of the aging population
- Effects of Tai Ji Quan training on gait kinematics in older Chinese women with knee osteoarthritis:A randomized controlled trial
- Recruitment of older adults into randomized controlled trials:Issues and lessons learned from two community-based exercise interventions in Shanghai
- Associations between individual and environmental factors and habitual physical activity among older Chinese adults:A social-ecological perspective
- Exercise-induced rhabdomyolysis mechanisms and prevention:A literature review
- Scientific evidence is just the starting point:A generalizable process for developing sports injury prevention interventions