上海市重症急性呼吸道感染儿童中可检出多种型别的人腺病毒
2016-08-09李亚敏刘高山周为民赵彦杰李玉川沈军谭文杰
李亚敏 刘高山 周为民 赵彦杰 李玉川 沈军 谭文杰
102206 北京,中国疾病预防控制中心 病毒病预防控制所应急技术中心(李亚敏、刘高山、周为民、赵彦杰、谭文杰); 201102上海,复旦大学附属儿童医院(李玉川、沈军)
上海市重症急性呼吸道感染儿童中可检出多种型别的人腺病毒
李亚敏刘高山周为民赵彦杰李玉川沈军谭文杰
102206 北京,中国疾病预防控制中心 病毒病预防控制所应急技术中心(李亚敏、刘高山、周为民、赵彦杰、谭文杰); 201102上海,复旦大学附属儿童医院(李玉川、沈军)
李亚敏、刘高山为共同第一作者
【摘要】目的了解上海市重症急性呼吸道感染(SARI)儿童中人腺病毒(HAdV)的感染情况及其分型特征。方法2013年6月至2014年3月从上海复旦大学附属儿科医院收集441份重症急性呼吸道感染患儿鼻咽抽吸物(NPAs)。采用巢式PCR的方法进行人腺病毒的检测,对阳性样本进行分型分析及基本流行病学特征分析。结果人腺病毒共检出51例(11.6%,95%CI 8.6%~14.6%)阳性,以0.5~1岁之间的患儿感染率较高,分型分析发现感染者中B组所占比例最高,共33例(64.7%),其中HAdV-3共17例(33.3%),HAdV-7共检出16例(31.4%);其次为C组共14例(27.5%);HAdV-D (HAdV-8)与HAdV-E(HAdV-4)各1例;HAdV-F(HAdV-41)检出2例。结论人腺病毒在上海市重症急性呼吸道感染患儿中有较高的感染率,存在多种基因型且以HAdV-B中的HAdV-3、7型感染最为常见。
【主题词】重症急性呼吸道感染;儿童;人腺病毒;分型检测
Fund programs: State Megaproject for Infectious Disease Research of China(2013ZX10004601,2013ZX10004-101)
人腺病毒(HAdV)是美国学者Rowe及其同事于1953年从人体的腺样组织中分离出来[1],该病毒属于腺病毒科(Adenoviridae),哺乳动物腺病毒属(Mastadenovirus),是无包膜的单股双链线性DNA病毒,包含HAdV-A到HAdV-G共7个亚属 69个基因型[2]。其中HAdV-1~ HAdV-52是根据血清中和试验确定的血清型[3,4],HAdV-53~HAdV-69是根据全基因序列生物信息学分析确定的基因型[2,5]。
HAdV感染可引起多种疾病包括肺炎、支气管炎、膀胱炎、眼结膜炎、胃肠道疾病及脑炎等[2,6],与呼吸道感染相关的主要是HAdV-B、HAdV-C及HAdV-D亚属,在婴幼儿中HAdV感染可引起严重的甚至致命的肺炎或支气管炎[7]。近年来国内外有诸多关于不同型别HAdV感染与爆发的报道,但上海市重症急性呼吸道感染患儿中HAdV感染的病原学资料尚缺乏,为明确该地区该特殊人群中HAdV的感染特点,我们展开此项研究,并报道如下。
1材料与方法
1.1检测样品2013年6月至2014年3月从上海复旦大学附属儿科医院收集441份重症急性呼吸道感染患儿(使用WHO儿童疾病管理规划的肺炎和重症肺炎的定义[8],主要临床表现为发热、咳嗽、呼吸短促或困难、咽喉痛及其他呼吸道感染症状)的鼻咽抽吸物。每例患儿收集约1 ml呼吸道样品,4℃存放不超过48 h,尽快运送至实验室,每份样品每200 μl分装一管,存于-70℃。
1.2核酸提取与病毒检测使用QIAamp MinElute Virus Spin Kit(QIAGEN,Germany)进行病毒全基因提取,按照说明书进行操作,最终溶于80 μl洗脱缓冲液。选取部分六邻体(hexon)基因作为基因分型区,使用巣式PCR的方法对HAdV进行分型检测与基因多态性分析[9-11]。反应体系25 μl,1.25U FastStart Taq DNA Polymerase,10×PCR Buffer,2mmol/L MgCl2(Roche Diagnostic Systems Inc., Mannheim, Germany),200 μmol/L dNTPs(日本,TaKaRa公司),0.5 μmol/L引物(大连宝生物工程有限公司合成),5 μl基因组提取液(第一轮)或2 μl的第一轮PCR产物(第二轮)。反应条件同参考文献[9,10]。第一轮PCR产物大小为1 004 bp,第二轮为956 bp。
1.3分型分析对检测阳性的内侧PCR产物使用QIAquick® Gel Extraction Kit(QIAGEN,Germany)进行切胶回收,按照操作说明书进行回收纯化,回收产物由上海生物工程有限公司进行序列测定。应用Sequin向基因库提交序列(序列号为:KR025751~ KR025768,KR025770~ KR025782,KR025784~ KR025788,KR025790~ KR025804),使用Clustal X软件将结果与GenBank上公布的与呼吸道感染相关的HAdV序列进行比对,经Bioedit软件裁齐序列后,使用MEGA 5.0软件进行进化分型分析。
1.4统计学方法使用统计学分析系统SAS9.2进行统计学分析,基本的流行病学特征使用χ2检验进行分析,P<0.05为差别有统计学意义。
2结果
2.1患儿基本特征441例SARI患儿中男性281例(63.7%),女性160例(36.3%),男女比为1.8∶1。中位年龄为1Y(0.3M~14Y),按年龄大小将患儿分为(≤6M、7M~≤1Y、2~≤5Y、>5Y)四组,各组分别有139人、125人、120人及57人。
2.2流行病学特征共检出51例HAdV感染者,阳性检出率为11.6%(51/441,95%CI8.6%~14.6%),男性患儿检出率为12.5%(35/281),女性患儿检出率为10.0%(16/160),不同性别患儿HAdV的检出情况差异均无统计学意义(P>0.05)。年龄≤6M组感染者8例,阳性率为5.8%(8/139);7M~≤1Y组阳性率为15.2%(19/125);2~≤5Y组阳性率为16.7% (20/120);>5Y组阳性率为7.0%(4/57),以6M~5Y患儿阳性率较高(P<0.05)。除夏季外其余三个季节HadV均有较高检出率,尤以冬春季检出率较高,除12月份外各个月份均有检出,且各个月份阳性检出率差异无统计学意义(P>0.05)(结果未示)。
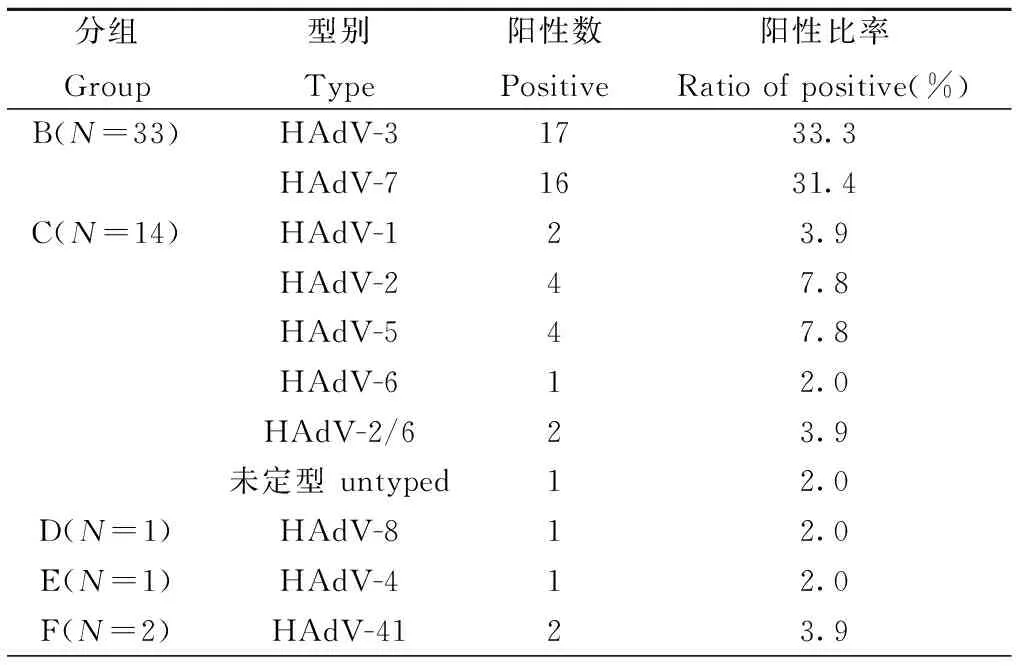
2.3分型分布特征根据感染HAdV阳性样本靶序列与各型别参考株核苷酸序列在进化树中的距离(图1),确定所感染HAdV所属型别(表1)。
2.4临床表现51例HAdV感染者中有48例诊断为肺炎,2例诊断为上呼吸道感染,1例为支气管炎。患儿主要表现为发热、咳嗽、喘息偶有腹泻症状,且这些症状在感染者与非感染者中差异无统计学意义(P>0.05)。
3讨论
HAdV-A~ HAdV-G七个亚属中,与急性呼吸道感染相关主要是HAdV-B(HAdV-3、-7、-11、-14及-21)与HAdV-E(HAdV-4)[12-15],对HAdV的快速分型检测有助于指导应急反应,并有助于指导治疗。不同地区急性呼吸道感染患儿中HAdV的检出率不尽相同[16-20],本研究SARI患儿中HAdV感染率为11.6%,与相关研究的结果一致,且HAdV的感染在季节分布上差异无统计学意义,与相关报道一致[21]。

图1 根据HAdV部分六邻体基因构建系统进化树(前缀“S”代表来自上海的样品.□,HAdV-A参考株; ●, HAdV-B参考株;■,HAdV-C参考株;▲, HAdV-D参考株;△,HAdV-E参考株; ◆,HAdV-F参考株)Fig.1 Phylogenetic analysis of HAdV based on the partial hexon gene.(Prefix-S:samples from Shanghai; □,sequences of reference strains of HAdV-A;●,sequences of reference strains of HAdV-B;■,sequences of reference strains of HAdV-C;▲,sequences of reference strains of HAdV-D;△,sequences of reference strains of HAdV-E;◆,sequences of reference strains of HAdV-F)
分组Group型别Type阳性数Positive阳性比率Ratioofpositive(%)B(N=33)HAdV-31733.3HAdV-71631.4C(N=14)HAdV-123.9HAdV-247.8HAdV-547.8HAdV-612.0HAdV-2/623.9未定型untyped12.0D(N=1)HAdV-812.0E(N=1)HAdV-412.0F(N=2)HAdV-4123.9
本研究发现上海市SARI患儿中HAdV感染以HAdV-B组为主,主要是HAdV-3与HAdV-7(占64.7%),其次为HAdV-C组(14/51,占27.45%),与北京、广州等地的研究结果较一致[22-23],但与同属华东地区的浙江温岭的流行株分布(以HAdVC组1,2,5型为主)不同[11,22],可能是研究时间、地区、样品形式或患儿疾病状态不同所致。另外,本研究发现在HAdV-C中,有一例未定型,进化分析发现其不属于HAdV-C中的任何一个型别而独立存在,很可能是HAdV-C中的新型别,不过,由于本研究中我们只针对部分六邻体基因进行分型检测,根据部分片段来确定新型别说服力尚显不足,有待于对该病毒全基因进行扩增,从全基因水平进行进一步的生物信息学分析来确定其准确的型别。
总之,本研究发现上海市重症急性呼吸道感染患儿中HAdV存在较高的检出率(11.6%),存在多种基因型。要明确该地区的流行株特征及进化规律还有待于长期动态地针对更大范围人群进行长期监测。
4参考文献
[1]Rowe WP, Huebner RJ, Gilmore LK, et al. Isolation of a cytopathogenic agent from a human adenoids undergoing spontaneous degeneration in tissue culture. Proc Soc Exp Biol Med, 1953, 84:570-573. doi: 10.3181/00379727-84-20714.
[2]Harrach B, Benk M, Both GW, et al. Family Adenoviridae. In: King AMQ, Adams MJ, Carstens EB, Lefkowitz EJ, editors. Virus Taxonomy. 9th Report of the International Committee on Taxonomy of Viruses. New York: Elsevier; 2011. pp. 125-141.
[3]Davison AJ, Benko M, Harrach B. Genetic content and evolution of adenoviruses. J Gen Virol, 2003, 84:2895-2908. doi: 10.1099/vir.0.19497-0.
[4]Jones MS, Harrach B, Ganac RD, et al. New adenovirus species found in a patient presenting with gastroenteritis. J Virol, 2007, 81:5978-5984. doi: 10.1128/JVI.02650-06.
[5]Seto D, Chodosh J, Brister JR, et al. Using the whole-genome sequence to characterize and name human adenoviruses. J Virol, 2011, 85:5701-5702. doi: 10.1128/JVI.00354-11.
[6]Elizabet GR, Dan HB. Adenoviruses. In: Mandell GL, Bennet JE, Dolin R, editors. Principles and Practice of Infectious Diseases. Philadephia: Churchill Livingstome; 2010. pp. 2077-2133.
[7]Mistchenko AS, Robaldo JF, Rosman FC, et al. Fatal adenovirus infection associated with new genome type. J Med Virol, 1998, 54:233-236. doi: 10.1002/(SICI)1096-9071(199803)54:3<233::AID-JMV15>3.0.CO;2-I.
[8]Ortiz JR, Sotomayor V, Uez OC, et al.Strategy to enhance influenza surveillance worldwide. Emerg Infect Dis, 2009, 15: 1271-1278. doi: 10.3201/eid1508.081422.
[9]Saitoh-Inagawa W, Oshima A, Aoki K, et al. Rapid diagnosis of adenoviral conjunctivitis by PCR and restriction fragment length polymorphism analysis. J Clin Microbiol, 1996, 34:2113-2116. pmid:8862567.
[10]Shimada Y, Ariga T, Tagawa Y, et al. Molecular diagnosis of human adenoviruses D and E by a phylogeny-based classification method using a partial hexon sequence. J Clin Microbiol, 2004, 42:1577-1584. doi: 10.1128/JCM.42.4.1577-1584.2004.
[11]李亚敏,周为民,赵彦杰,等. 浙南地区重症肺炎住院儿童中常见呼吸道病毒感染的检测分析. 中国病毒病杂志,2015,5,189-193.
[12]Pavia AT. Viral infections of the lower respiratory tract: old viruses, new viruses, and the role of diagnosis. Clin Infect Dis, 2011, Suppl 4: S284-S289. doi: 10.1093/cid/cir043.
[13]Tang L, Wang L, Tan X, et al. Adenovirus serotype 7 associated with a severe lower respiratory tract disease outbreak in infants in Shaanxi Province, China. Virol J, 2011, 8:23. doi:10.1186/1743-422X-8-23.
[14]Abd-Jamil J, Teoh BT, Hassan EH, et al. Molecular identification of adenovirus causing respiratory tract infection in pediatric patients at the University of Malaya Medical Center. BMC Pediatr, 2010, 10:46. doi: 10.1186/1471-2431-10-46.
[15]Selvaraju SB, Kovac M, Dickson LM, et al. Molecular epidemiology and clinical presentation of human adenovirus infections in Kansas City children. J Clin Virol, 2011, 51: 126-131. doi:10.1016/j.jcv.2011.02.014.
[16]Lee J, Choi EH, Lee HJ. Comprehensive serotyping and epidemiology of human adenovirus isolated from the respiratory tract of Korean children over 17 consecutive years (1991-2007). J Med Virol, 2010, 82:624-631. doi: 10.1002/jmv.21701.
[17]Abbas KZ, Lombos E, Duvvuri VR, et al. Temporal changes in respiratory adenovirus serotypes circulating in the greater Toronto area, Ontario, during December 2008 to April 2010. Virol J, 2013, 10:15. doi:10.1186/1743-422X-10-15.
[18]Barrero PR, Valinotto LE, Tittarelli E, et al. Molecular typing of adenoviruses in pediatric respiratory infections in Buenos Aires, Argentina(1999-2010). J Clin Virol, 2012, 53: 145-150. doi:10.1016/j.jcv.2011.11.001.
[19]Deng J, Qian Y, Zhao LQ, et al. Identification and typing of adenovirus from pediatric patients with acute respiratory infections in Beijing from 2003 to 2008. Chin J Pediatr, 2010, 48: 739-743.doi: 10.3760/cma.j.issn.0578-1310.2010.10.005.
[20]Wang T, Zhu R, Qian Y, et al. Investigation of common respiratory viruses in children with acute respiratory infection during 2009 pandemic influenza A(H1N1) in Bejing. Chin J Evid Based Pediatr, 2012, 7: 25-30. doi: 10.3969/j.issn.1673-5501.2012.01.005.
[21]Wong S, Pabbaraju K, Pang XL, et al. Detection of a broad range of human adenoviruses in respiratory tract samples using a sensitive multiplex real-time PCR assay. J Med Virol, 2008, 80:856-865. doi:10.1002/jmv.21136.
[22]Li Y, Zhou W, Zhao Y, et al. Molecular typing and epidemiology profiles of human adenovirus infection among paediatric patients with severe acute respiratory infection in China. PLoS One,2015,10:e0123234.doi:10.1371/journal.pone.0123234.
[23]Han G, Niu H, Zhao S, et al. Identification and typing of respiratory adenoviruses in Guangzhou, Southern China using a rapid and simple method. Virol Sin, 2013, 28:103-108. doi: 10.1007/s12250-013-3308-7.
通信作者:谭文杰,Email:tanwj28@163.com;沈军, Email:echoshen11@163.com
DOI:10.3760/cma.j.issn.1003-9279.2016.01.003
基金项目:传染病防治重大专项(2013ZX10004601,2013ZX10004-101)
(收稿日期:2015-12-31)
Prevalence of multiple types of human adenovirus infection among children with severe acute respiratory infection in Shanghai
LiYamin,LiuGaoshan,ZhouWeimin,ZhaoYanjie,LiYuchuan,ShenJun,TanWenjie
KeyLaboratoryofMedicalVirology,MinistryofHealth;NationalInstituteforViralDiseaseControlandPrevention,ChinaCDC,Beijing102206,China(LiYM,LiuGS,ZhouWM,ZhaoYJ,TanWJ);ShanghaiPediatricsHospitalAffiliatedFudanUniversity,Shanghai201102,China(LiYC,ShenJ)LiYaminandLiuGaoshanarethefirstauthorswhocontributedeaquallytothearticleCorrespondingauthor:TanWenjie,Email:Tanwj28@163.com;ShenJun,Email:echoshen11@163.com
【Abstract】ObjectiveTo investigate the typing profiles of human adenovirus infection among children with severe acute respiratory infection(SARI) in Shanghai. MethodsA total of 441 nasopharyngeal aspirates (NPAs) were collected from hospitalized children with SARI in Shanghai Pediatrics Hospital Affiliated Fudan University from June 2013 to March 2014. Human adenovirus was detected by nested PCR followed molecular typing by sequencing. Then the phylogenetic and epidemiological analysis was conducted. ResultsFrom 441 hospitalized children with SARI, 51 of samples (11.6%, 95%CI: 8.6%~14.6%) were detected as HAdV infection. Most of the SARI children with HAdV infection were distributed between 0.5 to 5 years old. Typing data shown that HAdV-B (17 of HAdV-3, 16 of HAdV-7) was most dominant as 64.7% (33/51),followed by HAdV-C as 27.5% (14/51); either HAdV-D (HAdV-8) or HAdV-E (HAdV-4) contained only one case, and HAdV-F (HAdV-41) found in two cases. ConclusionMultiple species(B-F)of HAdVs were circulated among children with SARI in Shanghai, and HAdV-B (HAdV-3, HAdV-7) was the most predominant species of circulation.
【Key words】Severe acute respiratory infection; Children;Human adenovirus;Typing detection
