Comparing the effectiveness of karate and fitnes training on cognitive functioning in older adults—A randomized controlled trial
2016-02-05KerstinWitteSiegfriedKropfSineDriusPeterEmmermherIrinkelmnn
Kerstin Witte*,Siegfried Kropf,Sine Drius,Peter EmmermherIrin Bökelmnn
aDepartment of Sport Science,Otto-von-Guericke-University,Magdeburg 39104,Germany
bDepartment for Biometrics and Medical Informatics,Otto-von-Guericke-University,Magdeburg 39120,Germany
cDepartment Occupational Medicine,Otto-von-Guericke-University,Magdeburg 39120,Germany
Comparing the effectiveness of karate and fitnes training on cognitive functioning in older adults—A randomized controlled trial
Kerstin Wittea,*,Siegfried Kropfb,Sabine Dariusc,Peter Emmermachera,Irina Böckelmannc
aDepartment of Sport Science,Otto-von-Guericke-University,Magdeburg 39104,Germany
bDepartment for Biometrics and Medical Informatics,Otto-von-Guericke-University,Magdeburg 39120,Germany
cDepartment Occupational Medicine,Otto-von-Guericke-University,Magdeburg 39120,Germany
Background:Recent studies demonstrate a slowdown in deterioration of cognitive functioning in old age through aerobic training.There is evidence that the combination of aerobic,balance,and coordination exercises leads to an improvement or maintenance of cognitive functions.Such age-related exercises can especially be found in East Asian martial arts.The purpose of the current study is to verify whether karate training for older adults improves cognitive functioning and,if an improvement can be found,which cognitive field are influenced
Methods:Eighty-nine older women and men(mean age:70 years)participated in this study.The participants were randomized into 2 intervention groups(karate group and fitnes group,duration of intervention:5 months)and a control group.All participants had to accomplish a cognitive test battery before and after the intervention.In a secondary study the karate group had an additional intervention for another 5 months.
Results:The results show that there is a significan improvement in motor reactivity,stress tolerance,and divided attention only after the 5-month karate training period.Additionally,the results of the secondary study indicate further improvements after 10 months.
Conclusion:The 5-month karate training can help to enhance attention,resilience,and motor reaction time,but a training period of 10 months is even more efficient
©2016 Production and hosting by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Cognition;Divided attention;Karate;Motor reactivity;Older adults;Physical exercise
1.Introduction
It is a fact that some cognitive functions decrease while others remain unaffected during aging.1–3According to Glisky3cognitive functioning containsbasic cognitive functions (attention,working memory included speed of information processing,long-term memory,perception)on one hand and higher-level cognitive functions(speech and language,decision making,executive control)on the other hand.
While“crystallized”intelligence(e.g.,factual knowledge and experience)retains,the“fluid intelligence(e.g.,working memory and processing speed)deteriorates,which also has an effect on other cognitive areas(e.g.,word fluen y and problem-solving ability).4The deterioration in cognition,based on biological degradation processes,especially affects thevelocity and fl xibility of information processing and memory retention.3Schapkin4suggests that neuroplasticity can activate additional areas of the brain which reduce the error rate and increase the reaction time.
Another important aspect is the relation between the decrease of cognitive abilities and the risk of falling.5Liu-Ambrose et al.6propose that improved cognitive function,especially executive functions and associated functional plasticity, may be an important mechanism to reduce falls in older adults. But this proposal has not been accepted yet.
A growing number of studies have analyzed the influenc of special sports interventions on cognitive abilities in older age. Meta-analyses were carried out by Colcombe and Kramer,7Smith et al.,8Price et al.,9and Zhao et al.,10who summarize that physical activity of older persons can improve cognitive performance11and decrease the risk of dementia in older people.12Findings from cross-sectional,longitudinal,and intervention studies with healthy older adults,frail patients,and persons suffering from mild cognitive impairment and dementialead to the conclusion that physical exercise is a promising non-pharmaceutical intervention to prevent age-related cognitive declination and neurodegenerative diseases.13
In particular,aerobic endurance training has a significan effect on processing speed,attention,and executive function, but only a minor one on working memory.1,8,14–16A possible reason is given by Colcombe et al.,17who,in an intervention study with persons aged 60–79 years,found out that the brain volume(white and gray matter)increases significant y after an aerobic training in comparison to a stretching training.Based on results of interventional studies Gregory et al.12show that endurance exercises increase the volume of special brain areas (particularly hippocampi).
Some studies give indications regarding the effect of other training programs than aerobic ones on cognitive performance. Hötting et al.14studied middle-aged adults(40–56 years)and found different effects between an aerobic endurance training (cycling)and a training with stretching and coordination on cognitive functioning,which both lead to advances in memory. The cardiovascular fitnes correlated more with episodic memory while stretching/coordination training particularly improved selective attention.
However,it should be considered that the heterogeneity of the subject groups(educational level,socioeconomic status) makes comparisons difficult1This can be seen by the results of the meta-analysis by Price et al.,9based on publications between 2006 and 2008,which show a great heterogeneity between the subject groups with regard to training intensity, educational level,and socioeconomic status.
Further research is needed to understand the impact of other forms of exercises as well as the intensity–response relationship that controls the positive impact of exercise on brain functions.13
Up to now,the influenc of duration,frequency,or intensity of exercises on cognitive performance could not be explained.It is an open issue whether physical exercises with a higher level of motor complexity,in comparison to relatively simple exercises,influenc more cognitive functions,brain physiology, respectively.Studies of complex and simple motor tasks are therefore required.
Boyke et al.18studied the implication of motor learning(in this case 3-ball cascade juggling)of older people(mean age:60years) on brain structure.On the basis of magnetic resonance imaging, they found that there was an increase of gray-matter changes in the middle temporal area of the visual cortex on the left side of the hippocampus and in the nucleus accumbens bilaterally.
Our study focuses on East Asian sports including wholebody exercises on a high coordinative level and investigates a possible effect on the cognitive performance of older adults. Chang et al.19postulate that Tai Chi improves cognitive abilities in older adults.The study by Dechamps et al.20of frail older adults confi ms that a Tai Chi training program(twice a week, 30 min)enhances the physical and mental state through the interaction of cognition and action.
Wagner21studied the effect of a modifie karate training of adults aged older than 50 years on physical and cognitive abilities and well-being.His finding show advances in short-term and procedural memory.He therefore concludes that appropriate karate training for older adults reduces fall risk and improves the subjective quality of life.
The study by Jansen and Dahmen-Zimmer22analyzed explicitly the impact of karate training,including exercises with more stringent requirements in coordination,on the well-being and cognitive abilities of older adults.The results show only trends of improvements in memory performance but significan improvements in well-being.It should to be noted that the training group contained only 12 subjects and the interventions had a duration of only 3 months.
Marie-Ludivine et al.23examined fiftee 50-year-old men in regard to the impact of karate training on healthy well-being, balance,aerobic capacity,and cognitive abilities.However,a control group without intervention is missing.The results show that a karate training over 12 months has a positive influenc on mood and perception of physical health.This was confi med by a better postural control,improved performance on objective physical testing,and shorter reaction time of the non-dominant hand.
From all these research finding we can conclude that a combination of aerobic,balance,and coordination exercises leads to an improvement or maintenance of cognitive functions. These age-related exercises are used in East Asian martial arts, e.g.,Tai Chi,taekwondo,Kung Fu,and karate.From these we selected karate,because techniques can exercise relatively slow, weapons may not be used and therefore the risk of injuries for older adults is low.The benefit of karate sport for older adults compared to other martial arts sports are discussed.23In summary,karate sport is characterized by aerobic fitness24coordination between arms and legs as well as between the right and left sides of the body at a relatively high level,continuous learning of new movements and orientation.
We expect that age-appropriate karate training helps to prevent cognitive decline in older age.Therefore,the aim of the present intervention study is to analyze the influenc of ageappropriate karate training on several field of cognition (common cognitive performance,motor reactivity,reactive stress tolerance,and divided attention)of older adults.We hypothesize that age-related karate training has a positive impact on common cognitive functioning,motor reactivity, reactive stress tolerance,and divided attention in older adults compared to common fitnes training or even without special sports programs.
In the primary study we therefore included a second sports intervention group(common fitnes training)and a control group without any specifi intervention program.The interventions were carried out over 5 months.Another aim was to analyze if there are further changes in cognitive functioning in the karate group.Therefore an additional 5-month karate training was accomplished for the karate group after the common intervention program in a secondary study.
2.Methods
2.1.Study design and participants
The randomized controlled study was carried out at the Department of Sport Science and at the Department ofOccupational Medicine of the Otto-von-Guericke-University Magdeburg and was approved by the Otto-von-Guericke-University Ethics Committee.A written informed consent was obtained from each participant.
The sample size was calculated to detect large effects(in the sense of Cohen’sd≥0.8)with a power of 80%for 2-sided tests at levelα=0.05 when comparing the 2 treatment groups.
Two hundred adults with a mean age of 70 years(age range:63–83 years)were recruited through advertisements in the local newspapers.Eighty-nine persons provided a medical certificat and had a professional training or a higher education degree(inclusion criteria).Three levels of physical activity were assessed through a questionnaire:no sports activity (Level 0),individual sports activity without any instructions (Level 1),and sports club activity(Level 2).The participants were sorted randomly into 2 intervention groups(Group 1: karate group and Group 2:fitnes group)and a control group (Group 3):without any planned sports interventions in relation to gender(about 40%men and 60%women),age(mean age: 69 years),and level of physical activity(Levels 0–2 were evenly distributed).
For the primary study the following timeline was defined pre-test(pre),intervention over 5 months,and post-test 1(po1). In the secondary study the intervention only for Group 1 was extended for another 5 months of karate training with another post-test 2(po2)afterwards.The test leaders were authorized to carry out and analyze cognitive tests and executed these blind in regard to groups.
Fig.1 shows the study timeline and consort participant fl w diagram.Only participants who undertook 80%of all training units of the interventions groups(Groups 1 and 2)were involved in the analysis.
2.2.Interventions
In addition to the group classification Fig.1 shows at which points in time the interventions were accomplished.
The sports interventions(karate and fitness of a duration of 60 min were performed twice per week by a karate expert for Group 1 and a fitnes trainer for Group 2.A training unit contained a warm-up phase(10–15 min),the specifi training (40–45 min),and a cool-down phase(5 min).
The warm-up phase of the karate training for Group 1 contained several balance exercises,exercises for improvement of reactions, as well as games for orientation.The cool-down phase included strengthening exercises for the body and short games.The5-month specifi karate training was divided into modules in conformity with Emmermacher and Witte.24They included stances such as forward stances(Jap.zenkutsu-dachi),back stances(Jap.kokutsudachi),and straddle-leg stances(Jap.kiba-dachi)to train leg and trunk musculature as well as balance skills.Also included were several arm techniques in standing positions and during forward and backward walking(downward-block(Jap.gedan-barai),lunge punches(Jap.oi-zuki),reverse punches(Jap.gyaku-zuki),and upper blocks(Jap.age-uke)to improve arm–leg coordination.In order to facilitate cognitive processes(reactivity,learning processes,memory,and attention)the participants executed simple attack and respond exercises(Jap.kumite)as well as the special karate form(Jap.kata)taikyoku-shodan.
The objectives of the fitnes training for Group 2 were: improvement of balance ability,coordination reaction,rhythm, body awareness,and strengthening of muscles.Accordingly,the main part of a training unit contained elements of gymnastics, running exercises,practices with balls and other hand devices, age-related games and strengthening exercises.
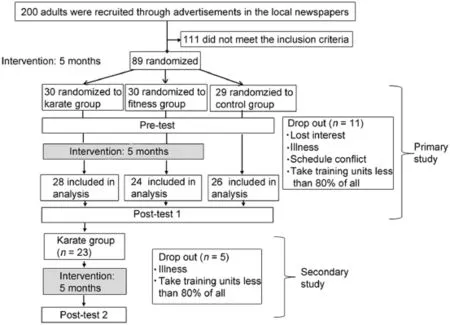
Fig.1.Study timeline and consort participant fl w diagram.
The participants in the control group,Group 3,were only instructed to continue their usual sports activities.
2.3.Outcome parameters
The following tests were conducted to measure common cognitive functioning,motor reactivity,reactive stress tolerance,and divided attention.
2.3.1.Common cognitive functioning
The DemTect test is a screening test for mild cognitive impairment and mild dementia and includes 5 short tasks: memory formation by word list,number transcoding,semantic word fluen y task,attention by digit span reverse,and delayed recall of word list.25Higher scores Ptotal(maximal total score is 18)indicate better cognitive functioning.
2.3.2.Motor reactivity
The rod test is a simple motor test to determine the ability to react to a failed rod:the test leader drops a rod in a define distance into a person’s hand,which catches it.The falling length is a parameter for measuring the reaction time.26A shorter falling length(L)indicates a better reaction time.
2.3.3.Reactive stress tolerance
DT Determination Test Version S11(Vienna Test System 024674-01;SCHUHFRIED GmbH,Mödling,Austria)is a computer controlled test assessing reactive stress tolerance.DT measures stress tolerance,attention,and reaction speed to rapidly changing visual and acoustic stimuli.The subject is presented with color stimuli and acoustic signals during the test procedure and the task is to react by pressing the appropriate buttons on the response panel.The reliability is given withr=0.98.The validity was examined among others in the fiel of traffi psychology.27A lower score(TtotalMed)indicates a better reactive stress tolerance.
2.3.4.Divided attention
Test of Divided Attention(TAP 2.2,Psytest—Psychological Test Systems; PSYTEST Psychologische Testsysteme, Herzogenrath,Germany)is a computer controlled test which examines the divided attention(dual-task performance)to parallel processed visual and acoustic signals.The subject has to respond as fast as possible when a special visual pattern appears or the same tone occurs twice.Lower reaction times to acoustic (Ac_med)and visual signals(Vis_med)indicate a better performance in divided attention.The reliability was examined by Zoccolotti et al.28(r=0.33...0.73,p<0.01).Objectivity is given through a complete automatic analysis.
The test leaders were authorized to carry out and analyze cognitive tests and executed these blind to the groups.
2.4.Statistical analysis
The normal distribution of all outcome parameters was confi med by means of the Kolmogorov–Smirnov test.In the primary study the pairedttest was used to evaluate differences between the results of the pre and po1 within the groups.In case of a significan result the effect size(Cohens’sd) was calculated.Furthermore,a two-way repeated measures (Time×Group)ANOVA,with time as the within-subject factor and group as the between-subject factor,was used to assess all outcome parameters in the primary study.In the secondary study the one-way ANOVA(factor time:pre,po1,and po2)and pairwise Bonferroni correctedpost hoccomparisons were carried out.
The analyses were performed with a significanc level of 0.05.In addition,results with apvalue smaller than 0.1 were presented to show possible trends.
The data were collected and organized using EXCEL (Microsoft Excel 2010;Microsoft Corp.,Redmond,WA,USA). Statistical analyses were performed by the statistical software package IBM SPSS Statistics(Version 22.0,64-Bit-Version; IBM Corp.,Armonk,NY,USA).
3.Results
Eleven participants of the primary study and 5 participants of the secondary study dropped out because of missing more than 20%of all training units based on several reasons(Fig.1). No significan differences between the groups concerning age (Group 1:68.8±4.1;Group 2:69.0±5.3;Group 3:68.0±5.1; one-way ANOVA:F=1.468,total degree of freedom(df)=2,p=0.229),gender composition(Group 1:male=12,female= 16;Group 2:male=8,female=16;Group 3:male=10, female=16;2-dimensionalχ2test:χ2(Pearson)=0.495,df=2,p=0.781;χ2(Likelihood quotient)=0.497,df=2,p=0.780), or physical activity level(2-dimensionalχ2test:χ2(Pearson)= 0.399,df=6,p=0.092)were found.
The results of the two-way repeated measures ANOVA (Table 1)show no significan differences between the groups for each parameter related to factor Group.Based on this,we conclude an equal baseline for all 3 groups.No adverse effectsof karate training and fitnes training during intervention in both studies could be found.

Table 1 Results of the general common model(two-way repeated measures ANOVA)—primary study.

Table 2 Group data of the test parameters(analyzed at pre-test(pre)and post-test 1(po1))—primary study(mean±SD).
3.1.Results of the primary study
3.1.1.Common cognitive functioning
The results of the two-way repeated measures ANOVA show no significan differences in total score Ptotal(DemTect test) related to the factors Time,Group,and their interaction (Table 1).Results of mean comparisons within the groups confi m these finding(Table 2).Only Group 1 is characterized by a slight but not significan improvement of Ptotal.
3.1.2.Motor reactivity
Considering the simple Rod Test we found a significan effect considering Time×Group(Table 1).Remarkably,there is a significan improvement of the Rod test performance L with a small effect for Group 1(Table 2).
3.1.3.Reactive stress tolerance
For the total performance in the DT Determination Test (TtotalMed)two-way repeated measures ANOVA could identify a significan effect only for factor Time(Table 1).Concerning differences between pre and po1,the 3 groups offer a significan improvement of this parameter(Table 2).
3.1.4.Divided attention
Significan results could only be found for(median value of reaction time to acoustic signals)(Ac_Med)through a two-way repeated measures ANOVA for the factor Time×Group (Table 1).The comparison within the groups shows only for Group 1 a trend based improvement(Table 2).It should be noted that a decrease in reaction time related to acoustic signal only occurs for Group 1(positive sign).
3.2.Results of secondary study
The secondary study should analyze whether further improvements of detected parameters can be confi med when the karate training was extended for another 5 months.
3.2.1.Common cognitive functioning
Generally,the DemTect test detects changes in mild cognitive impairment.Kalbe et al.25proved its applicability for early detection of dementia,while Wagner21used DemTect test for healthy adults at middle age.In our finding one-way repeated measures ANOVA shows only a trend when all 3 test dates are compared(Table 3).This improvement could only be confi med between po2 and pre.Considering the single subtests we could only fin an improvement for item A5(number of the right mentioned words of the recalled word list to measure recalled memory)comparing pre with po2(pre:5.32±2.09, po1:5.71±2.09,po2:6.39±2.29;one-way repeated measures ANOVA:sum of squares=20.957,mean squares=10.478,F(2,22)=4.202,p=0.021,η2=0.160;pairedttest prevs.po2:t=-2.69,p=0.013)after 10 months of karate training.

Table 3 Results of the general common model(one-way repeated measures ANOVA)—secondary study(mean±SD).
3.2.2.Motor reactivity
For the practice-oriented Rod Test(L)high significan improvements of Group 1 were found comparing pre,po1,and po2,especially considering po2vs.po1(Table 3).
3.2.3.Reactive stress tolerance
We investigated whether the parameters which show signifi cant or potential changes in Gr1(primary study)vary more after the second 5-month karate training period.For TtotalMed significan differences between pre,po1,and po2 were confi med.Post hoctests show that parameters of po2 improve highly significant y in relation to pre and po1(Table 3).
3.2.4.Divided attention
On the basis of one-way repeated measures ANOVA the results of Ac_Med in pre,po1,and po2 vary significant y.Post hoctests show significan differences between po2 and pre and between po1 and pre.The impairment of Ac_Med in po2 in relation to po1 is not significan(Table 3).
4.Discussion
Because only a small number of empirical studies analyzing the impact of karate training to cognitive functioning exist,a comparison of our results with finding in literature is limited.
It can be concluded that the effect of the slight improvement of memory performance(item A5 of DemTect)is small compared with the results of the study’s findin of significan improvements in memory performance by aerobic endurance training.11The slight improvement of recalled memory caused by karate training agrees with results of Boyke et al.,18who showed that motor learning enhances the plasticity of the brain in older adults.Our results are in contrast to those of Wagner,21who discovered that 50–65-year-old adults(n=59)generally improve their performance in DemTect through age-appropriate karate training.Wagner21found significan improvements in all sub-items(A1–A5)and total score.The contrast in our results to those of Wagner21can be explained by the age of our participants,who were nearly 20 years older than the participants of Wagner’s study.Our finding agree with results by Jansen and Dahmen-Zimmer,22who applied the digit-span test,figur test and block-tapping test with only 12 participants over 20 training units within 3–6 months without findin any cognitive improvements.
The motion-oriented Rod Test only showed an improvement in performance for the karate group after both 5 months and 10 months of training.Similar results were reported by Marie-Ludivine et al.,23who found an improvement in reaction time of the non-dominant hand after(adapted)karate training with duration of both 6 months and 12 months for 50-year-old men. So it can be assumed that karate training over an extended period of time has a positive impact on motor reactivity.We therefore conclude that partner exercises in karate training in particular lead to reduced reaction times in physical exercises.
While karate techniques inherit demanding coordinative movements,especially for people of older age,karate training could be valuable for training of reactive stress tolerance and attention,which was analyzed by Determination Test.Based on our finding it can be concluded that the slight improvements of reactivity in the Determination Test do not result exclusively from karate training.But a trend improvement of the test’s parameter TtotalMed after 5 and 10 months’intervention for Group 1 could be found.
Regarding divided attention,the reaction time to acoustic signals(Ac_Med)was especially reduced through karate training.We explain this findin based on the fact that participants performing karate training have to react immediately to acoustic instructions of the trainer,for instance rhythmic counting in kata exercises.Compared to the other intervention group (Group 2)and control group(Group 3)we can conclude that karate training in older adults counteracts the deterioration of reactivity under stress and in dual tasks.
We explain the general small effects considering the factors Time and Group with the recruitment through advertisements in the local newspapers.It can be assumed that only older adults with active lifestyles express their willingness to be included in a study with physical intervention.
5.Conclusion
The presented study shows a limitation in regard to the study design.While we compared 3 groups in pre and po1 in the primary study,we analyzed only the karate group in the secondary study(single group design).These results can therefore only be shown as a trend.
In general,we have to note that the recruited participants had a good level of fitness In contrast,there are studies with frail persons that,from a logical point of view,improved their cognitive functions by physical training significant y(mixture from stretching,endurance,strength,and coordination training).14From these finding we suppose that age-appropriate karate training positively influence particular cognitive functions of healthy older and frail people.We consider the main reason for positive effects is based on cognitive functioning,the learning of new movement techniques and kata,which includes physical as well as cognitive components,in karate training.Furthermore,we assume that karate training in older adults could have an additional effect:the reduction of falling risk.This is due to the relation between cognitive abilities and falling risk29and the training of balance and leg muscles by karate exercises.
Acknowledgment
A positive vote by the Ethics Committee(Otto-von-Guericke-University Magdeburg, Germany, registration number:109/11)was given.The study was supported by the Otto-von-Gueicke-University Magdeburg,Germany.
Authors’contributions
KW conceived of scientifi idea,carried statistical analysis, drafted the manuscript,and carried motor tests;SK carried statistical analysis;SD carried cognitive tests;PE carried karate intervention;and IB analyzed cognitive tests and designed the study.All authors have read and approved the fina version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
None of the authors declare competing financia interests.
1.Lukas I,Lindholm H,Winkler R.Influenc of endurance training on cognitive performance in older age—a review.(Der Einflus von Ausdauersport auf die kognitive Leistungsfähigkeit im Alter—Ein Überblick).ArbeitsmedSozialmedUmweltmed2011;46:624–8.[in German].
2.Schapkin SA,Freude G,Gajewski PD,Wild-Wall N,Falkenstein M. Effects of working memory load on performance and cardiovascular activity in younger and older workers.Int J Behav Med2012;19:359–71.
3.Glisky EL.Changes in cognitive function in human aging.Chapter I.In: Riddle DR,editor.Brain aging,models,methods,and mechanisms—frontiers in neuroscience.Boca Raton,FL:CRC Press;2007.
4.Schapkin SA.Age-related cognitive abilities—compensatory processes and physiological costs. (Altersbezogene Änderungen kognitiver Fähigkeiten—kompensatorische Prozesse und physiologische Kosten). Forschung Projekt F 2152(research project F 2152).Bundesanstalt für Arbeitsschutz und Arbeitsmedizin.Dortmund/Berlin/Dresden2012.p.102. [in German].
5.Chen TY,Peronto CL,Edwards JD.Cognitive function as a prospective predictor of falls.J Gerontol B Psychol Sci Soc Sci2012;67:720–8.
6.Liu-Ambrose T,Nagamatsu LS,Hsu CL,Bolandzadeh N.Emerging concept:‘central benefi model’of exercise in falls prevention.Br J Sports Med2013;47:115–7.
7.Colcombe S,Kramer AF.Fitness effect on the cognitive function of older adults:a meta-analytic study.Psychol Sci2003;14:125–30.
8.Smith PJ,Blumenthal JA,Hoffman BM,Cooper H,Straumann TA, Welsh-Bohmer K,et al.Aerobic exercise and neurocognitive performance: a meta-analytic review of randomized controlled trials.Psychosom Med2010;72:239–52.
9.Price AE,Corwin SJ,Friedman DB,Laditka SB,Colabianchi N, Montgomery KM.Physical activity and cognitive-health content in top-circulating magazines,2006–2008.J Aging Phys Act2011;19:147–68.
10.Zhao E,Tranovich MJ,Wright VJ.The role of mobility as a protective factor of cognitive functioning in aging adults:a review.Sports Health2014;6:63–9.
11.Angevaren M,Vanhees L,Wendel-Vos W,Verhaar HJ,Aufdemkampe G, Aleman A,et al.Intensity,but not duration,of physical activities is related to cognitive function.Eur J Cardiovasc Prev Rehabil2007;14:825–30.
12.Gregory SM,Parker B,Thompson PD.Physical activity,cognitive function,and brain health:what is the role of exercise training in the prevention of dementia?Brain Sci2012;2:684–708.
13.Bherer L,Erickson KI,Liu-Ambrose T.Review of the effects of physical activity and exercise on cognitive and brain functions in older adults.J Aging Res2013;2013:657508.doi:10.1155/2013/657508
14.Hötting K,Reich B,Holzschneider K,Kauschke K,Schmidt T,Reer R, etal.Differential cognitive effects of cycling versus stretching/ coordination training in middle-aged adults.Health Psychol2011;31: 145–55.
15.Langlois F,Vu TTM,Chassé K,Dupuis G,Kergoat MJ,Bherer L.Benefit of physical exercise training on cognition and quality of life in frail older adults.J Gerontol B Psychol Sci Soc Sci2012;68:400–4.
16.Nagamatsu LS,Chan A,Davis JC,Beattie BL,Graf P,Voss MW,et al. Physical activity improves verbal and spatial memory in older adults with probable mild cognitive impairment:a 6-month randomized controlled trial.J Aging Res2013;2013:861893.doi:10.1155/2013/861893
17.Colcombe SJ,Erickson KI,Scalf PE,Kim JS,Prakash R,McAuley E,et al. Aerobic exercise training increases brain volume in aging humans.J Gerontol A Biol Sci Med Sci2006;61:1166–70.
18.Boyke J,Driemeyer J,Gaser C,Büchel C,May A.Training-induced brain structure changes in the elderly.J Neurosci2008;28:7031–5.
19.Chang YK,Pan CY,Chen FT,Tsai CL,Huang CC.Effect of resistance-exercise training on cognitive function in healthy older adults: a review.J Aging Phys Act2012;20:497–517.
20.Dechamps A,Onifade C,DecampsA,Bourdel-Marchasson I. Health-related quality of life in frail institutionalized elderly:effects of a cognition-action intervention and Tai Chi.J Aging Phys Act2009;17:236–48.
21.Wagner HJ.Infuence of combined coordination and strength training based on karate to risk of fall,cognition and life quality of elderly people. (Einfuss eines kombinierten Koordinations-und Krafttrainings auf der Basis von Karate auf Sturzrisiko,Kognition und Lebensqualität bei älteren Menschen).Munich:Technical University of Munich;2009.[Dissertation] [in German].
22.Jansen P,Dahmen-Zimmer K.Effects of cognitive,motor,and karate training on cognitive functioning and emotional well-being of elderly people.FrontPsychol2012;3:40. doi:10.3389/fpsyg.2012.00040. eCollection 2012
23.Marie-Ludivine CD,Papouin G,Saint-Val P,Lopez A.Effect of adapted karate training on quality of life and body balance in 50-year-old men.Open Access J Sports Med2010;1:143–50.
24.Emmermacher P,Witte K.Exercise in a different way—fall prevention as well as maintaining and improving of learning and memory performance in older adults by East Asian martial arts.(Bewegung einmal anders—SturzprophylaxesowieErhalt undVerbesserungvonLern-und Gedächtnisleistungen im Alter durch ostasiatische Kampfkunst).1st ed. Aachen:Shaker-Verlag;2012[in German].
25.Kalbe E,Kessler J,Calabrese P,Smith R,Passmore AP,Brand M,et al. DemTect:a new,sensitive cognitive screening test to support the diagnosis of mild cognitive impairment and early dementia.Int J Geriatr Psychiatry2004;19:136–43.
26.Grosser M,Starischka S.Tests of condition(Konditionstests).Vol.42. Munich:Blv Sportwissen;1986.
27.Karner T,Neuwirth W.Validation of traffi psychology tests by comparing with actual driving.In:International Conference on Traffc and Transport Psychology.Bern,Switzerland.4–7 September,2000.
28.Zoccolotti P,Matano A,Deloche G,Cantagallo A,Passadori A,Leclercq M,et al.Patterns of attentional impairment following closed head injury:a collaborative European study.Cortex2000;36:93–107.
29.Bolandzadeh N,Liu-Ambrose T,Aizenstein H,Harris T,Launer L,Yaffe K,et al.Pathways linking regional hyperintensities in the brain and slower gait.Neuro Image2014;99:7–13.
Received 2 September 2014;revised 8 January 2015;accepted 25 May 2015
Available online 21 September 2015
Peer review under responsibility of Shanghai University of Sport.
*Corresponding author.
E-mail address:kerstin.witte@ovgu.de(K.Witte).
http://dx.doi.org/10.1016/j.jshs.2015.09.006
2095-2546/©2016 Production and hosting by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
杂志排行

Journal of Sport and Health Science的其它文章
- Biomarker-guided classificatio scheme of neurodegenerative diseases
- Mechanism of neurodegeneration through tau and therapy for Alzheimer’s disease
- Examining the relationship between sport and health among USA women: An analysis of the Behavioral Risk Factor Surveillance System
- The microbiome,microbial-generated proinflammato y neurotoxins, and Alzheimer’s disease
- Longitudinal trajectories of physical activity in women using latent class growth analysis:The WIN Study
- Evidence of a conservative gait strategy in athletes with a history of concussions