Examining the relationship between sport and health among USA women: An analysis of the Behavioral Risk Factor Surveillance System
2016-02-05JenniferPharrNancyLough
Jennifer R.Pharr*,Nancy L.Lough
aDepartment of Environmental and Occupational Health,University of Nevada Las Vegas,Las Vegas,NV 89154,USA
bCollege of Education,University of Nevada Las Vegas,Las Vegas,NV 89154,USA
Examining the relationship between sport and health among USA women: An analysis of the Behavioral Risk Factor Surveillance System
Jennifer R.Pharra,*,Nancy L.Loughb
aDepartment of Environmental and Occupational Health,University of Nevada Las Vegas,Las Vegas,NV 89154,USA
bCollege of Education,University of Nevada Las Vegas,Las Vegas,NV 89154,USA
Background:Research has been conducted linking sports participation and health in childhood and adolescence;however,little is known about the contribution of sport to women’s health.The purpose of this study was to examine the relationship between sport and women’s health in the USA by analyzing data from the Behavioral Risk Factor Surveillance System(BRFSS).
Chronic diseases;Conditioning exercise;Leisure-time physical activity;Recreation;Sport participation;Women’s health
1.Introduction
Regular physical activity(PA)reduces the risk for chronic disease and improves overall health.1–5Aerobic exercise helps reduce the incidence of cardiovascular disease(heart disease and stroke)and reduces risk factors for cardiovascular disease such as obesity,diabetes,high blood pressure,and high cholesterol in adults.1–3,6,7It has also been shown to improve pulmonary function,bone density,body image,and self-esteem.1,2,7–10Specifi to women,examples of positive outcomes from engaging in regular PA include improved survival after diagnosis of breast cancer and possible reduced risk of breast cancer and colon cancer,reduced risk of osteoporosis and cardiovasculardisease,improved perceived health status and feelings of vitality,and reduced risk of metabolic syndrome.4,11–17For example, Manson and colleagues17found that women who walked briskly for 3 or more hours per week were significanty less likely to have a nonfatal or fatal myocardial infarction when compared with women who exercised infrequently.
Leisure-time PA can be divided into 4 categories,including sport,conditioning exercise,household tasks,and other (recreation).18Sport can be further define as“a human activity of achieving a result requiring physical exertion and/or physical skill which,by its nature and organization,is competitive and is generally accepted as being a sport”.19Research examining the health benefit of sport for children and adolescents is quite extensive.20–24However,in adults,most research compares people who are physically active with people who are not physically active.Additionally,some research has examined the health benefit of leisure-time PA based on its intensity,whichcan be measured as metabolic equivalents(METs).25–29PA that has a higher intensity produces a greater MET value,and a MET value of 6 or greater is associated with vigorous PA.30,31People who engage in vigorous PA(e.g.,sport)are more likely to reap the health benefit associated with being physically active than those who engage in PA associated with a lower MET value.25–29The majority of previous research has not attempted to parse out the health benefit of sport from other forms of leisure-time PA,nor has it focused on women.19
Research has been conducted to understand the difference in motivational factors for participation in sport compared with conditioning exercise in adults.People who participate in sport are more likely to be intrinsically motivated,whereas people who participate in exercise are more likely to be extrinsically motivated.32–36Intrinsic motivators of improved health,enjoyment,challenge,and competence are highly associated with sport participation,whereas the extrinsic motivators of physical appearance and weight loss are highly associated with exercise.Because the primary motivators for sport participation are intrinsic,researchers have concluded that sport participation might be a more sustainable form of PA,with a greater likelihood that those involved will meet the PA recommendations for improved health from Centers for Disease Control and Prevention(CDC).32
Increasingly,many countries including the UK and Australia are focused on growing women’s sport as a strategy to improve health among women.37,38Despite an emerging understanding of the importance of PA for women’s health,little is known about the contribution thatsportmakes to women’s health in the USA.Lamb and colleagues39examined the health outcomes of sport participation in Britain and found that women who participated in sport had lower blood pressure,lower resting heart rate,lower body mass index,and better perceived health. Liechty and colleagues40found that participating in tackle football improved body image among the women who participated. Interestingly,no large-scale studies on the impact of sport on women’s health have been conducted in the USA.
The Behavioral Risk Factor Surveillance System(BRFSS) survey conducted in 2013 provided a large,national dataset for the analysis of this relationship.By analyzing BRFSS data,this study examined the relationship between sport and women’s health in the USA.We wanted to see whether women who participate in sport reported fewer chronic conditions and better health than women who participated in other forms of PA.Our hypotheses were the following:
(1)Women who report participating in sport will be signifi cantly less likely to report chronic diseases than women who report participating in conditioning exercise,household tasks,or recreation,and differences will remain after adjusting for demographic characteristics including age, income,education,and race/ethnicity.
(2)Women who report sports participation will be signifi cantly more likely to meet the recommended amount of exercise per week and achieve a higher MET value compared with women who participate in conditioning exercise,household tasks,or recreation.
2.Methods
2.1.Ethics approval
This study was deemed as excluded by the University of Nevada,Las Vegas,Institutional Review Board because it was a secondary data analysis of de-identifie data.
2.2.BRFSS
This study was a secondary data analysis of the 2013 BRFSS, which is the largest survey of adults in the USA.The survey is a collaborative effort between the CDC and each state and territory of the USA(Guam,Puerto Rico,and the Virgin Islands).41It began in 1984 and was conducted every year.The BRFSS is a random digit dial telephone survey that includes noninstitutionalized adults who are 18 years or older.Disproportionate stratifie sampling is employed to provide an adequate sample size for smaller demographic areas.41Data are weighted for population attributes and nonresponse.41Beginning in 2011,cellular telephones were added to landlines in the survey to maintain generalizability, coverage,and validity in data collection.The BRFSS has been found to have high reliability(test–retest comparisons)and validity(compared with other surveys,participant logs,accelerometers,or other PA measures)for the PA questions,especially for those who report high levels of PA.42
The core component of the BRFSS questionnaire includes questions that are asked of all respondents about their demographics,preventative health practices,chronic diseases,and health risk behaviors.Unlike the BRFSS core component from previous years,in 2013 participants were questioned extensively about their exercise behaviors.43The initial exercise question was,“During the past month,other than your regular job,did you participate in any physical activities such as running,calisthenics,golf,gardening,or walking for exercise?”43Participants who answered“yes”to this question were then asked more specifi questions about their exercise.The next question was,“What type of physical activity or exercise did you spend the most time doing the past month?”43This was an open-ended question,and participants could only identify 1 activity or exercise for this question. Seventy-six different activities were identifie by the participants. Next the participants were asked,“How many times per week or permonth did you take part in this activity during the past month?”followed by“and when you took part in this activity,for how many minutes or hours did you usually keep at it?”43
Based on the answers to the exercise questions(activity,duration,and frequency),the CDC calculated variables for each participant regarding their PA category(highly active,active, insufficienty active,or inactive)and whether they met the recommendations for the amount of aerobic exercise.PA levels set by the CDC for the BRFSS were determined as follows:highly active—respondents who reported doing enough PA to meet the recommended 300 min of aerobic activity or 150 min of vigorous aerobic exercise;active—respondents who reported doing 150–300 min of aerobic activity(or the vigorous equivalent);insuffi ciently active—respondents who reported doing insufficien PA (11–149 min of aerobic activity);and inactive—respondents who reported doing no PA.43The recommended amount of aerobic exercise was define by the CDC for the BRFSS as“meetingaerobic recommendations”(respondents who reported doing 150+min(or vigorous equivalent)of aerobic exercise)or“not meeting aerobic recommendations”(respondents who reported doing insufficien PA(0–149 min of aerobic exercise)).43Additionally,based on the answer to the exercise question,the CDC assigned a METs value to the activity.
Participants provided demographic data including age, employment,education,race/ethnicity,income,and marital status.They were also asked about chronic conditions,including previous heart attack,cardiovascular disease,stroke,high blood pressure,high cholesterol,asthma,skin cancer,other cancers,chronic obstructive pulmonary disease,arthritis, depression,kidney disease,and diabetes.Answers to chronic disease questions were“yes”,“no”,“I don’t know”,or“refused to answer”.
For this study,women who answered“no”to the initial exercise question(“During the past month,other than your regular job,did you participate in any physical activities such as running,calisthenics,golf,gardening,or walking for exercise?”),who refused to answer the second exercise question (“What type of physical activity or exercise did you spend the most time doing the past month?”),and men were excluded from our analysis.Two researchers,one with a background in sport and one with a background in PA,reviewed the 76 different activities and independently placed them into 4 predetermined leisure-time PA categories of sport,conditioning exercise,household tasks,and recreation(Table 1).The 4 categories were a modificatio of the 4 categories provided and described by Caspersen et al.,18which included sport, conditioning exercise,household tasks,and other.We used Caspersen et al.’s descriptions as well as the definitio of sport provided earlier to categorize the different activities and to differentiate sport from the other forms of activity.We agreed on the categories 96%of the time.The 3 activities that we did not agree upon were discussed,and we were ultimately able to agree on their categorization.Participants could indicate only 1 activity or exercise in answer to the question and could not be counted in multiple categories.
2.3.Statistical analyses
SAS Version 9.2(SAS Institute Inc.,Cary,NC,USA)was used for statistical analyses of demographic characteristics and chronic conditions by exercise category.Weighted descriptive statistics were obtained to describe the demographic characteristics of the 4 exercise categories by gender,age,race,education,income,employment,and marital status.To determine statistically significan differences in demographic characteristics,PA level,and aerobic recommendation achieved by exercise category,χ2tests were performed using PROC SURVEYFREQ in SAS to test Hypothesis 2.Additionally, PROC SURVEYMEANS in SAS was used to calculate the mean number of minutes and the mean METs associated with the activity for each of the PA categories along with a 95% confidenc interval(CI)to compare groups.If the 95%CI did not overlap,then the groups were significanty different. Chronic conditions were dichotomized as“yes”or“no”,with“I don’t know”and“refused”coded as missing.Logistic regression was used to calculate crude and adjusted odds ratios for chronic conditions by exercise category,with sport as the reference category.Because there were significan differences between exercise groups for all the demographic variables,we controlled for all demographic variables when calculating adjusted odds ratios.PROC SURVEYLOGISTIC was used for this analysis to test Hypothesis 1.
3.Results
In 2013,290,498 women participated in the BRFSS survey. In total,180,523 women reported participating in some form of leisure-time PA,with 14,985(8.3%)participating in sport, 143,389(79.4%)in conditioning exercise,5282(2.9%)in recreation,and 16,867(9.4%)in household tasks.Demographic characteristics of the participants can be found in Table 2.There were significan differences between groups,with the group who reported participating in sport having a higher percentage of women who indicated that they were college graduates,in the 18–24 or 25–34 age range,earning more than USD75,000 per year,and employed.Although women who participated in sport were more likely to be married and White,when compared to the other PA groups,sport had a higher percentage of single and Hispanic participants.
When comparing general health and PA levels by categories (Table 3),there were significan differences,with a higher percentage of women who reported participating in sport reporting good to excellent health.However,women who reported participating in recreation or household tasks were more likely to be categorized as highly active and meeting aerobic exerciserecommendations(i.e.,exercising more)than women in the sport or conditioning exercise groups.These unexpected find ings will be elaborated on in the discussion.When comparing the means and 95%CI for minutes and METs,women who participated in recreation or household tasks spent significanty more time in their activities;however,women who participated in sport had significanty higher METs or worked at a higher intensity during their activities(Table 4).
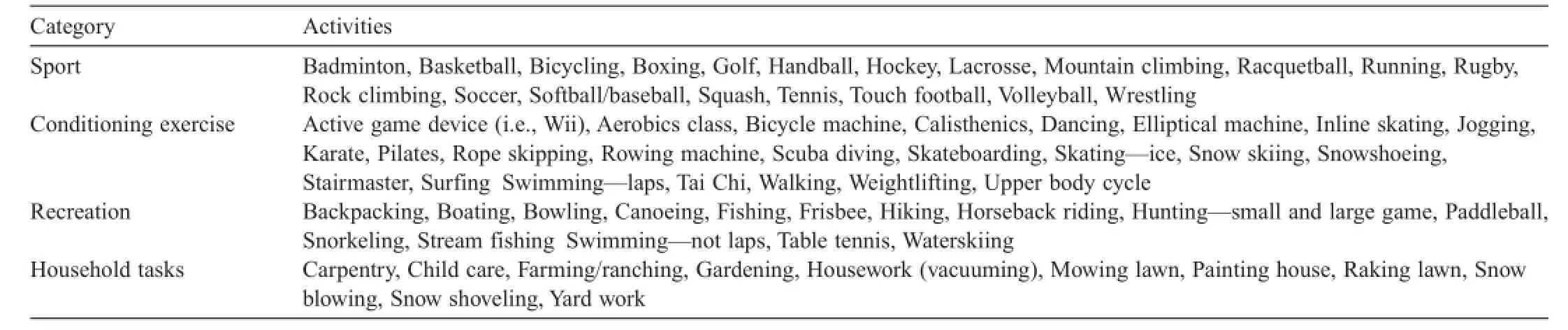
Table 1 Exercise categories for reported activities.
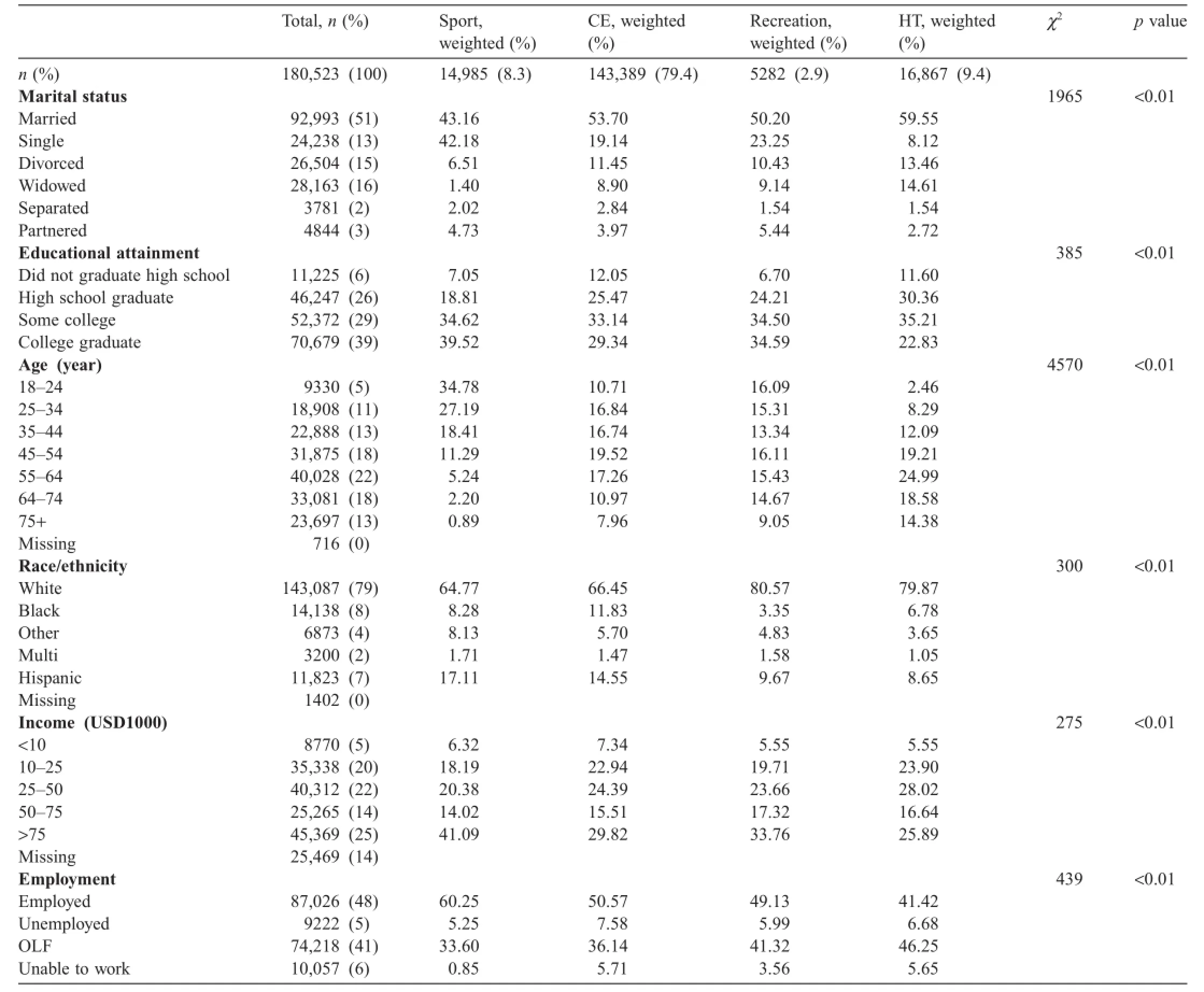
Table 2 Demographic characteristics by exercise type-weighted percentages.
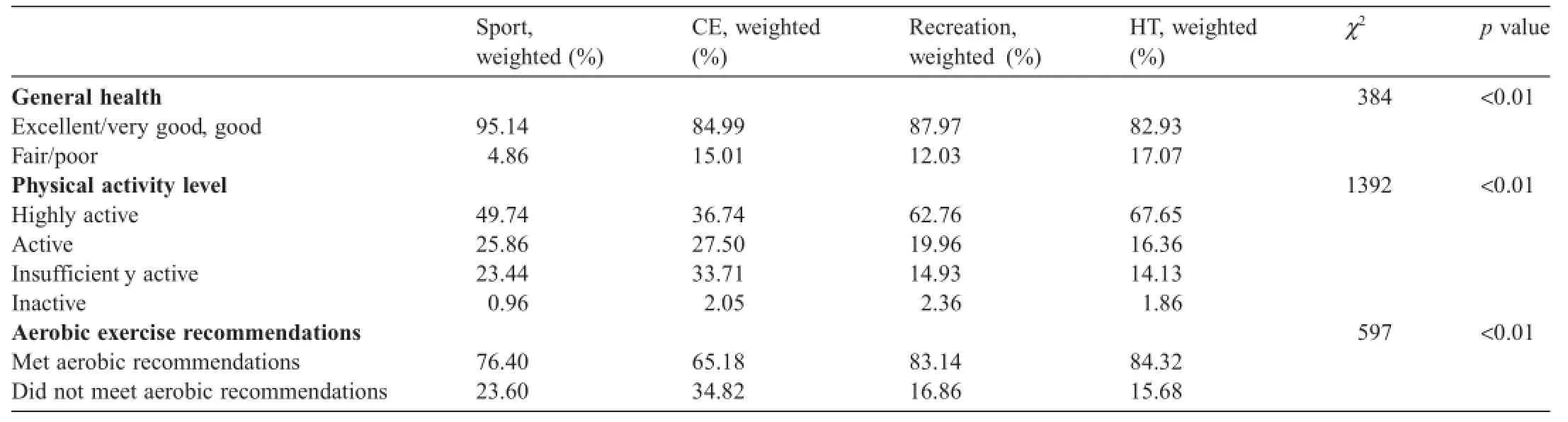
Table 3 General health and exercise amounts by exercise type.

Table 4 Exercise time and METs by exercise type(mean(range)).
Odds ratios and adjusted odds ratios are reported in Table 5. Women who participated in sport were used as the reference category.Compared with women who participated in sport, women who participated in conditioning exercise,recreation,or household tasks were significant y more likely to report all chronic conditions except asthma.When controlling for demographic variables(i.e.,age,income,and education),the signifi cant differences remained,with women who participated in conditioning exercise,recreation,or household tasks reporting higher rates for many of the chronic conditions.
In sum,the firs hypothesis was confi med,demonstrating that (1)women who report participating in sport were significant y less likely to report chronic diseases than women who report participating in conditioning exercise,household tasks,or recreation, and(2)differences in chronic diseases remained after adjusting for demographic characteristics including age,income,education, and race/ethnicity.Surprisingly,the second hypothesis,that women who report sports participation are significanty more likely to meet the recommended amount of exercise per week compared with women who participated in conditioning exercise, recreation,or household tasks,was not supported.
4.Discussion
Studies looking at motivations for participating in sport point to health as a primary motive.34–36With health acknowledged as an impetus for sport participation,we wanted to see whether women who participated in sport had fewer chronic conditions and better health than women who participated in other forms of PA.This was the firs large-scale study to consider the impact of sport on the health of women in the USA.
Key finding suggest a relationship between sport and the health of women in the USA.A higher percentage of women who said that they participated in sport reported good to excellent health.Relatedly,compared with women who participated in sport,women who participated in conditioning exercise, recreation,or household tasks were significant y more likely to report all chronic conditions except asthma.When demographic variables were controlled for,many of the differences remained.Our finding are similar to those from studies on the benefit of sport participation in mixed-gender samples.For example,Hoffman and Krishnan44examined the health implications of ultramarathon running among a group of runners including both genders.They found that ultramarathon runners had a low prevalence of cancers,coronary artery disease, seizure disorders,diabetes,and human immunodeficien y virus infection.
Ironically,women who reported participating in recreation or household tasks were more likely to be categorized as highly active and meeting aerobic exercise recommendations for time compared with women in the sport group;however,womenwho participated in sport reported better general health.This may be due to the way in which the variables were calculated. Both variables were based on the amount of time that women reported engaging in activities.When compared with sport, recreation activities and household tasks lend themselves to being sustained over a longer period of time.For example,a person is more likely to be able to fish hunt,hike,or backpack for a longer period of time than they can run,cycle,or play soccer.To be categorized as highly active,a person needed to either participate in aerobic activity for≥300 min or participate in vigorous aerobic activity for>150 min.On average,women in the household tasks group reported doing 443 min of activity, and this amount of activity automatically places someone in the highly active category regardless of intensity.However,women who participated in sport did so at a significant y higher intensity(METs),and this higher intensity may have resulted in the improved health outcomes observed.
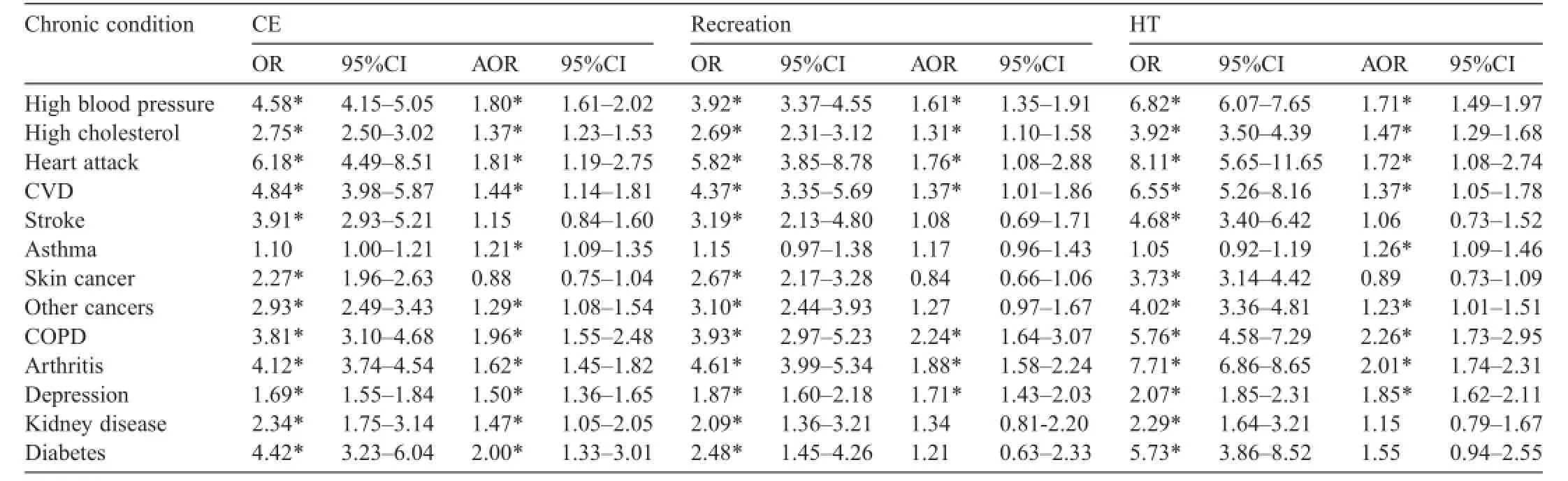
Table 5 OR and AOR for chronic conditions with sport as reference.
We found that women who participated in sport had an average MET of 6.18,the highest of the 4 groups.They also had decreased odds and adjusted odds of high cholesterol,history of a heart attack or cardiovascular disease,chronic obstructive pulmonary disease,arthritis,or depression when compared with the other groups.This findin is consistent with previous studies,which show greater health benefit associated with vigorous(i.e.,higher METs and higher intensity)PA.25,26,28,29Warburton et al.4found a linear relationship between fitnes levels and health status,with people who exercised at a higher intensity having the lowest rates of disease.In this study,we found that sport was associated with higher intensity PA,suggesting that sport may be an approach to encourage women to exercise at a greater intensity.
Women who participated in sport reported better health,which means one goal would be to encourage more women to engage in sport as a means of preventing chronic disease and attaining better health outcomes.Other countries are increasingly focused on growing women’s sport as a strategy to improve health among women.For example,the health and sport ministries in the UK and Australia have initiated new programs focused on encouraging sport participation among women.Sport England is investing half a billion pounds to increase sport participation among women over 4 years(2013–2017).37In Australia,VicHealth’s“Changing the Game:Increasing Female Participation in Sport”program was launched in August,2015,with the goal of getting 25,000 more women and girls to participate in sport.38
Lastly,the impact of education was notable in the findings Women who reported participating in sport were more likely to be single,college graduates,18–34 years old,making more than USD75,000 per year,and employed when compared with the other exercise types.Arguably,the relationship between level of education attained(college graduate),employment status,and income contributes to the socioeconomic status warranted for sport participation.If we embrace a model to increase sport participation among women to promote health, a key strategy needed is to insure that sport is affordable and accessible to all women.
There were limitations with this study.Causation cannot be determined because the BRFSS is cross-sectional.45There was a possibility of bias resulting from self-reported information, and the participants may also have under-or over-reported information if they perceived the response to be socially desirable.46However,with 180,523 participants,the finding from this initial study merit consideration and point to the need for additional research.
5.Conclusion
Sport participation was associated with more vigorous PA and positive health outcomes among women in the USA.Other countries have nationally organized initiatives to increase sport participation among women.These initiatives may serve as examples to guide efforts in the USA to increase women’s sport participation, which was shown in this study to be associated with positive health outcomes.If we consider a similar initiative in the USA,we need to identify how we can create a model for sport participation among women that satisfie the motives identifie but also is affordable and accessible to all women across the lifespan.
Authors’contributions
JRP and NLL designed the study and coded the PA.JRP conducted the statistical analysis.JRP and NLL drafted the manuscript and approved the fina submission.Both authors have read and approved the fina version of the manuscript and agree with the order of presentation of the authors.
Competing interests
Neither of the authors declare competing financia interests.
1.O’Donovan G,Blazevich AJ,Boreham C,Cooper AR,Crank H,Ekelund U,et al.The ABC of physical activity for health:a consensus statement from the British Association of Sport and Exercise Sciences.J Sports Sci2010;28:573–91.
2.Vuori I.Physical activity and cardiovascular disease prevention in Europe: an update.Kinesiology2010;42:5–15.
3.Bauman AE.Updating the evidence that physical activity is good for health:an epidemiological review 2000–2003.JSci MedSport2004;7:6–19.
4.Warburton DE,Nicol CW,Bredin SS.Health benefit of physical activity: the evidence.CMAJ2006;174:801–9.
5.Hardman AE,Stensel DJ.Physical activity and health:the evidence explained.New York,NY:Routledge;2009.
6.Andersen LB,Harro M,Sardinha LB,Froberg K,Ekelund U,Brage S, et al.Physical activity and clustered cardiovascular risk in children:a cross-sectional study (The European Youth Heart 6Study).Lancet2006;368:299–304.
7.Ferreira I,Boreham CA,Twisk JW,Gallagher AM,Young IS,Murray LJ, et al.Clustering of metabolic syndrome risk factors and arterial stiffness in young adults:the Northern Ireland Young Hearts Project.J Hypertens2007;25:1009–20.
8.Biddle SJ,Gorely T,Stensel DJ.Health-enhancing physical activity and sedentary behaviour in children and adolescents.J Sports Sci2004;22: 679–701.
9.Hind K,Burrows M.Weight-bearing exercise and bone mineral accrual in children and adolescents:a review of controlled trials.Bone2007;40: 14–27.
10.Tremblay MS,LeBlanc AG,Kho ME,Saunders TJ,Larouche R,Colley RC,et al.Systematic review of sedentary behaviour and health indicators in school-aged children and youth.Int J Behav Nutr Phys Act2011;8:98. doi:10.1186/1479-5868-8-98
11.Eifert EK,Wideman L,Oberlin DJ,Labban J.The relationship between physical activity and perceived health status in older women:finding from the woman’s college alumni study.J Women Aging2014;26:305–18.
12.Freese EC,Acitelli RM,Gist NH,Cureton KJ,Evans EM,O’Connor PJ. Effect of six weeks of sprint interval training on mood and perceived health in women at risk for metabolic syndrome.J Sport Exerc Psychol2014;36:610–8.
13.Irwin ML,Mc Tiernan A,Manson JE,Thomson CA,Sternfeld B,Stefanick ML,et al.Physical activity and survival in postmenopausal women with breast cancer:results from the women’s health initiative.Cancer Prev Res (Phila)2011;4:522–9.
14.Lin CH,Chiang SL,Yates P,Lee MS,Hung YJ,Tzeng WC,et al.Moderate physical activity level as a protective factor against metabolic syndrome in middle-aged and older women.J Clin Nurs2015;24:1234–45.
15.Phipps AI,Chlebowski RT,Prentice R,McTiernan A,Stefanick ML, Wactawski-Wende J,et al.Body size,physical activity,and risk of triple-negative and estrogen receptor-positive breast cancer.Cancer Epidemiol Biomarkers Prev2011;20:454–63.
16.Kendall KL,Fairman CM.Women and exercise in aging.J Sport Health Sci2014;3:170–8.
17.Manson JE,Hu FB,Rich-Edwards JW,Colditz GA,Stampfer MJ,Willett WC,et al.A prospective study of walking as compared with vigorous exercise in the prevention of coronary heart disease in women.N Engl J Med1999;341:650–8.
18.Caspersen CJ,Powell KE,Christenson GM.Physical activity,exercise,and physical fitness definition and distinctions for health-related research.Public Health Rep1985;100:126–31.
19.Eime RM,Young JA,Harvey JT,Charity MJ,Payne WR.A systematic review of the psychological and social benefit of participation in sport for children and adolescents:informing development of a conceptual model of health through sport.Int J Behav Nutr Phys Act2013;10:98. doi:10.1186/1479-5868-10-98
20.Baumert PW,Henderson JM,Thompson NJ.Health risk behaviors of adolescent participants in organized sports.JAdolescHealth1998;22:460–5.
21.Pate RR,Trost SG,Levin S,Dowda M.Sports participation and health-related behaviors among US youth.Arch Pediatr Adolesc Med2000;154:904–11.
22.Taliaferro LA,Rienzo BA,Donovan KA.Relationships between youth sport participation and selected health risk behaviors from 1999 to 2007.J Sch Health2010;80:399–410.
23.Donaldson SJ,Ronan KR.The effects of sports participation on young adolescents’emotional well-being.Adolescence2006;41:369–89.
24.Dishman RK,Hales DP,Pfeiffer KA,Felton GA,Saunders R,Ward DS, et al.Physical self-concept and self-esteem mediate cross-sectional relations of physical activity and sport participation with depression symptoms among adolescent girls.Health Psychol2006;25:396–407.
25.Lee IM,Paffenbarger Jr RS.Associations of light,moderate,and vigorous intensity physical activity with longevity.The Harvard Alumni Health Study.Am J Epidemiol2000;151:293–9.
26.Sesso HD,Paffenbarger Jr RS,Lee IM.Physical activity and coronary heart disease in men:the Harvard Alumni Health Study.Circulation2000;102:975–80.
27.O’Donovan G,Owen A,Bird SR,Kearney EM,Nevill AM,Jones DW, et al.Changes in cardiorespiratory fitnes and coronary heart disease risk factors following 24 wk of moderate-or high-intensity exercise of equal energy cost.J Appl Physiol2005;98:1619–25.
28.Samitz G,Egger M,Zwahlen M.Domains of physical activity and all-cause mortality:systematic review and dose-response meta-analysis of cohort studies.Int J Epidemiol2011;40:1382–400.
29.Yu S,Yarnell JW,Sweetnam PM,Murray L.Caerphilly study.What level of physical activity protects against premature cardiovascular death?The Caerphilly Study.Heart2003;89:502–6.
30.Jones DA,Ainsworth BE,Croft JB,Macera CA,Lloyd EE,Yusuf HR. Moderate leisure-time physical activity:who is meeting the public health recommendations?A national cross-sectional study.Arch Fam Med1998;7:285–9.
31.Fletcher GF,Froelicher VF,Hartley LH,Haskell WL,Pollock ML. Exercise standards.A statement for health professionals from the American Heart Association.Circulation1990;82:2286–322.
32.Kilpatrick M,Hebert E,Bartholomew J.College students’motivation for physical activity:differentiating men’s and women’s motives for sport participation and exercise.J Am Coll Health2005;54:87–94.
33.Ryan RM,Frederick CM,Lepes D,Rubio N,Sheldon K.Intrinsic motivation and exercise adherence.Int J Sport Psychol1997;28:335–54.
34.Funk D,Jordan J,Ridinger L,Kaplanidou K.Capacity of mass participant sport events for the development of activity commitment and future exercise intention.Leis Sci2011;33:250–68.
35.Geurin-Eagleman A.Attitudes,motivation,and commitment of runners who do and do not participate in women-only road races.Int J Sport Manag Mark2014;13:200–17.
36.Lough N,Pharr J,Geurin A.I am Bolder:a social cognitive examination of road race participant behavior.Sport Mark Q2016;5:90–102.
37.Sport England.Women.Available at:http://www.sportengland.org/our -work/equality-diversity/women/;[accessed 05.08.2015].
38.VicHealth.Changing the game:increasing female participation in sport. Available at:https://www.vichealth.vic.gov.au/changing-the-game;2015 [accessed 05.08.2015].
39.Lamb KL,Brodie DA,Minten JH,Roberts K.A comparison of selected health-related data from surveys of a general population and a sporting population.Soc Sci Med1991;33:835–9.
40.Liechty T,Sveinson K,Willfong F,Evans K.It doesn’t matter how big or small you are...there’s a position for you:body image among female tackle football players.Leis Sci2015;37:109–24.
41.Centers for Disease Control and Prevention.Behavioral risk factor surveillance system overview:BRFSS 2013.Available at:http://www.cdc .gov/brfss/annual_data/2013/pdf/overview_2013.pdf; 2014 [accessed 05.08.2016].
42.Pierannunzi C,Hu SS,Balluz L.A systematic review of publications assessing reliability and validity of the behavioral risk factor surveillance system(BRFSS),2004–2011.BMC Med Res Methodol2013;13:49.doi: 10.1186/1471-2288-13-4
43.Centers for Disease Control and Prevention.Behavioral risk factor surveillance sytstem:2013 codebook report.Available at:http://www.cdc .gov/brfss/annual_data/2013/pdf/codebook13_llcp.pdf; 2014 [accessed 05.08.2015].
44.Hoffman MD,Krishnan E.Health and exercise-related medical issues among 1,212 ultramarathon runners:baseline finding from the Ultrarunners Longitudinal TRAcking (ULTRA)study.PLoSOne2014;9:e83867.doi:10.1371/journal.pone.0083867
45.Aschengrau A,Seage GR.Essentials of epidemiology in public health. Burlington,MA:Jones&Bartlett Learning;2003.
46.Adams AS,Soumerai SB,Lomas J,Ross-Degnan D.Evidence of self-report bias in assessing adherence to guidelines.Int J Qual Health Care1999;11:187–92.
Received 1 March 2016;revised 19 May 2016;accepted 14 June 2016
Available online 18 July 2016
Peer review under responsibility of Shanghai University of Sport.
*Corresponding author.
E-mail address:Jennifer.pharr@unlv.edu(J.R.Pharr)
http://dx.doi.org/10.1016/j.jshs.2016.07.005
2095-2546/©2016 Production and hosting by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Methods:This study was a secondary data analysis of the 2013 national BRFSS survey.Unlike the BRFSS core component from previous years,in 2013,participants were questioned extensively about their physical activity behaviors.Seventy-six different activities were identifie by the participants.Two researchers categorized the 76 activities as sport,conditioning exercise,recreation,or household tasks based on previously identifie categories.Logistic regression was utilized to calculate odds ratios and adjusted odds ratios for chronic diseases based on physical activity category.Results:Women who participated in sport had better health outcomes with significanty lower odds for all chronic diseases except asthma and better general health than women who participated in conditioning exercise,household tasks,or recreation,and many of the significan differences remained after controlling for demographic characteristics.
Conclusion:Sport participation was associated with more positive health outcomes among women in the USA compared with the other categories. As a means to improve health of women,the USA could focus on efforts to increase sport participation among women.
©2016 Production and hosting by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
杂志排行

Journal of Sport and Health Science的其它文章
- Biomarker-guided classificatio scheme of neurodegenerative diseases
- Mechanism of neurodegeneration through tau and therapy for Alzheimer’s disease
- The microbiome,microbial-generated proinflammato y neurotoxins, and Alzheimer’s disease
- Longitudinal trajectories of physical activity in women using latent class growth analysis:The WIN Study
- Evidence of a conservative gait strategy in athletes with a history of concussions
- Total soy saponins improve the antioxidant capacity of the myocardium and exercise ability in exhausted rats