Competitive trampolining influence trabecular bone structure, bone size,and bone strength
2016-02-05LaurenBurtJohnSchipilowStevenBoyd
Lauren A.Burt,John D.Schipilow,Steven K.Boyd*
Department of Radiology,Faculty of Medicine,McCaig Institute for Bone and Joint Health,University of Calgary,Calgary T2N 4Z6,Canada
Competitive trampolining influence trabecular bone structure, bone size,and bone strength
Lauren A.Burt,John D.Schipilow,Steven K.Boyd*
Department of Radiology,Faculty of Medicine,McCaig Institute for Bone and Joint Health,University of Calgary,Calgary T2N 4Z6,Canada
Background:Trampolining is a form of gymnastics that has increased in popularity over the last decade and due to its concurrence with the formative years of bone development,it may have an important impact on bone health.However,bone density,microarchitecture,and bone strength of competitive trampolinists have not been explored.Therefore,the purpose of this cross-sectional study was to investigate the relationship between trampolining participation and(1)bone density,area,and microarchitecture;and(2)estimated bone strength and the role of muscle and impact loading in young female adults.
Methods:We recruited 29 female participants aged 16–29 years for this study(n=14 trampolinists;n=15 controls).Skeletal parameters were assessed using dual X-ray absorptiometry,high-resolution peripheral quantitative computed tomography(HR-pQCT),and finit element analysis (FEA).Muscle strength was measured using dynamometers.
Results:Trampolinists had higher bone density at the hip and spine,greater trabecular density and thicker trabeculae at the tibia,as well as larger bones at both the tibia and radius than controls(p<0.05).Trampolinists also had higher muscle strength than controls at the lower body with no difference between groups in the upper body.Estimates of bone strength using FEA were greater for trampolinists than controls at both the radius and tibia.
Conclusion:This is the firs study to investigate bone density,area,and microarchitecture in female trampolinists using HR-pQCT.Trampolinists had greater bone density,area,microarchitecture,and estimated bone strength than controls.
©2016 Production and hosting by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Dual X-ray absorptiometry;Finite element analysis;Gymnastics;High-resolution peripheral quantitative computed tomography;Muscle strength;Trampolining
1.Introduction
Trampolining is 1 of 7 gymnastics disciplines consisting of men’s and women’s artistic gymnastics,rhythmic gymnastics, aerobics,acrobatics,and gymnastics for all(general gymnastics combining all disciplines in a fun non-competitive environment).Specifical y,trampolining consists of individual trampoline,synchronized trampoline,double mini-trampoline,and tumbling.In the year 2000 trampolining became an Olympic sport;however,Olympic competition only involves individual trampoline1and does not include 3 additional forms of trampolining.Nevertheless,as a result of its inclusion in the Olympics,trampolining has increased in popularity over thepast decade.1Popularity has increased at both an unstructured“free-play”(backyard)level as well as in structured form at local gymnastics centers.2
Most of the scientifi literature on trampolining highlights the injuries associated with both unstructured and structured involvement in the sport.2–5However,health benefit including enhanced strength,endurance,balance,and proprioceptive development following involvement in trampolining are also important aspects of the sport.2,6At a clinical level,trampolines have been used to increase maximal oxygen uptake in children with cystic fibrosis7to improve motor and balance ability in children with intellectual disability,8and to enhance hip moment and balance during forward falls in an elderly cohort.9At a competitive level,the physiological responses and fatigue patterns of elite male trampoline athletes have been explored.10However,bone density, microarchitecture,and bone strength of competitive trampolinists are not known.Therefore,the aim of this study was toinvestigate the relationship between trampolining gymnastics participation and(1)bone density,area,and microarchitecture; and(2)estimated bone strength and the role of muscle and impact loading in young adult females.
2.Materials and methods
2.1.Participants
We recruited 29 female participants aged 16–29 years for this cross-sectional study over a 9-month period.Sample size was based on large effect sizes previously reported in gymnastics studies.11To achieve over 80%statistical power a minimum of 14 participants per group was required.12,13Trampolinists (n=14)were training and competing at a provincial or national level.Controls(n=15)were female sedentary volunteers recruited using information fl ers from the student population at the University of Calgary.Controls have no previous or current training history in any competitive or organized sporting programs.Participants were healthy individuals with no medical conditions known to effect bone metabolism.Approval for all procedures was obtained from the University of Calgary Conjoint Health Research Ethics Board.All participants over the age of 18 years provided written informed consent prior to involvement in the study.For those participants under 18 years, a parent provided written informed consent on behalf of the child.
2.2.Anthropometrics
Height(Seca model 222;Seca,Hamburg,Germany)and weight(Seca model 876;Seca)were measured using standard protocols to the nearest 0.1 cm and 0.1 kg,respectively.Dual X-ray absorptiometry(DXA,Discovery A,Hologic Inc., Bedford,MA,USA)was used to obtain a measurement of lean mass(kg)and percent body fat(%)from a whole-body scan.
2.3.Health,physical activity,and calcium
All participants completed a series of questionnaires to assess their overall health and well-being.The short version of the International Physical Activity Questionnaire,a reliable and valid questionnaire14,15was used to determine general physical activity.Trampolinists completed a training history questionnaire to capture their weekly training commitments(training volume)and training age.To capture calcium intake,all participants completed a food frequency questionnaire(FFQ).The FFQ has been used by the Canadian Multi-Centre Osteoporosis Study,16which is a modifie version of the Block et al.17(short form)and Willett et al.18questionnaires;however,has not been validated in an independent study.
2.4.Skeletal parameters
Both the dominant and non-dominant limbs were scanned as part of this study.Differences between limbs were not detected and as a result the dominant limb has been reported in this manuscript.
2.4.1.DXA
Areal bone mineral density(aBMD,g/cm2)of the dominant hip(femoral neck(FN)and total hip(TH)),and lumbar spine (LS,L1–L4)was obtained by DXA.Controls were scanned on their dominant hip identifie as the leg used to kick a ball, whereas trampolinists were scanned on their sport-specifi dominant hip determined as the takeoff leg(push leg or last leg to leave the ground)in a hurdle.Machine calibration,daily and weekly quality assurance assessments were performed and monitored as per the manufacturer guidelines.All scans were performed and analyzed by 1 trained technologist(ISCD certified)
2.4.2.High-resolution peripheral quantitative computed tomography(HR-pQCT)
To assess measurements of volumetric bone mineral density (BMD,mg HA/cm3),and bone macro-and micro-architecture of the peripheral skeleton,participants received an HR-pQCT scan(XtremeCT,Scanco Medical,Brüttisellen,Switzerland)of their radius and tibia.Controls were scanned on their dominant radius and tibia,whereas trampolinists were scanned on their sport-specifi dominant radius and tibia determined by the“push”or second hand in a cartwheel and the takeoff leg in a hurdle.The opposite limb was scanned if a previous fracture was reported(n=1 trampolinist;n=1 control).
Participants were scanned using a standard humanin vivoscanning protocol(60 kVp,1000 μA,100 ms integration time). Following a scout scan,reference lines were placed at the midinclination tuberosity and at the plateau portion of the tibial endplate,for the radius and tibia,respectively.19Each scan was comprised of 110 slices,corresponding to a 9.02 mm scan area, with a nominal isotropic resolution of 82 μm carried out at the standard location 9.5 mm(radius)and 22.5 mm(tibia)proximal to the reference line.Trained technologist performed and analyzed all scans using the standard manufacturer’s method.20Scans were graded for motion artifacts:a scan scoring 1 had no motion,and a scan scoring 5 was subject to severe blurring and discontinuities.21None of our scan data had to be removed due to motion artifacts(motion score of 4 or higher)or inadequate scan quality.HR-pQCT CVs range from<1%for density measures to 4% for microarchitecture parameters in our laboratory.22
Total and trabecular volumetric BMD(Tt.BMD,Tb.BMD; mg HA/cm3),trabecular number(Tb.N;1/mm)and thickness (Tb.Th;mm)were obtained by the standard morphologic analysis20as described in detail elsewhere.19
Bone size and cortical parameters,including total crosssectional area (Tt.Ar;mm2),cortical volumetric BMD (Ct.BMD;mg HA/cm3),cortical thickness(Ct.Th;mm),and cortical porosity(Ct.Po;%)were determined using an automated segmentation method.23,24
2.4.3.Finite element analysis(FEA)
Estimates of bone strength were based on custom FEA software(FAIM,Version 6.0;Numerics88 Solutions,Calgary, Canada)applied to each HR-pQCT scan using a linear,homogenous model.A uniaxial compression test was simulated on each radius and tibia using a 1%axial strain,Young’s modulus of 6829 MPa and a Poisson’s ratio of 0.3.25Our primary estimate of bone strength was failure load(N)based on 2%of the elements exceeding 7000 microstrain.26
2.5.Muscle strength
2.5.1.Biodex dynamometer
A Biodex isokinetic dynamometer(System 3;Biodex,New York,NY,USA)set at 90°/s measured maximal isokinetic knee extension torque(KET,N·m)and knee fl xion torque(KFT, N·m)of the dominant leg.Our testing protocol has been described in detail elsewhere.27In brief,maximal torque was calculated from 3 sequential experimental trials where the combination of knee extension and fl xion at 90°/s consisted of 1 trial.
2.5.2.Grip strength
A grip strength dynamometer(Almedic,Quebec,Canada) measured overall isometric strength(kg).Grip strength assessment was performed on the same arm as was scanned by HR-pQCT and we implemented the Canadian Physical Activity, Fitness,and Lifestyle Approach protocol.28Participants performed 3 trials of a maximal effort squeeze(contracting for 5 s) with the maximum value being recorded.
2.6.Statistics
Statistical analyses were performed using SPSS Version 19 (IBM,Armonk,NY,USA).Results are displayed as mean±SD, and significanc was define asp<0.05.Following Shapiro–Wilk tests for normal distribution,ttest and a Fisher’s exact test were used to explore anthropometric,health,nutrition,and physical activity between groups.To assess potential bias,subanalyses were performed on trampolinists with a training history in artistic gymnastics(n=4)to ensure they were not different from the remainder of the trampolinists.Due to anthropometric differences between trampolinists and controls, age,height,and weight adjusted ANCOVAs were used to compare skeletal and muscle strength parameters between groups.To determine the role of muscle and impact loading in estimates of bone strength,a linear regression model was used. Predictors of bone strength were entered into the model in the following order:(1)age,height,and weight,(2)age,height, weight,and trampolining gymnastics participation(categorical variable),(3)age,height,weight,trampolining gymnastics participation,and grip strength(radius only)or KFT(tibia only).
3.Results
3.1.Anthropometric characteristics
Anthropometric characteristics of trampolinists and controls are illustrated in Table 1.Trampolinists were younger,smaller, and lighter than controls(p<0.05).Body mass index(BMI) was not significanty different between trampolinists and controls;however,trampolinists had a lower percent body fat than controls(p<0.001).None of the participants in this study have been,or were currently pregnant or amenorrheic.Following a Fisher’s exact test 50% of trampolinists and 21%of controls were taking oral contraceptives;however,this was not signifi cant between groups(p>0.05).The percentage of individuals who fractured was not different between groups(p>0.05),36%of trampolinists and 27%of controls recorded a previous fracture.Lower extremity fractures were more prevalent among trampolinists whereas upper extremity fractures occurred more frequently in controls.Trampolinists with previous participation in artistic gymnastics(n=4)were not different from those with no previous experience in artistic gymnastics(n=10) (p>0.05).3.2.Skeletal parameters
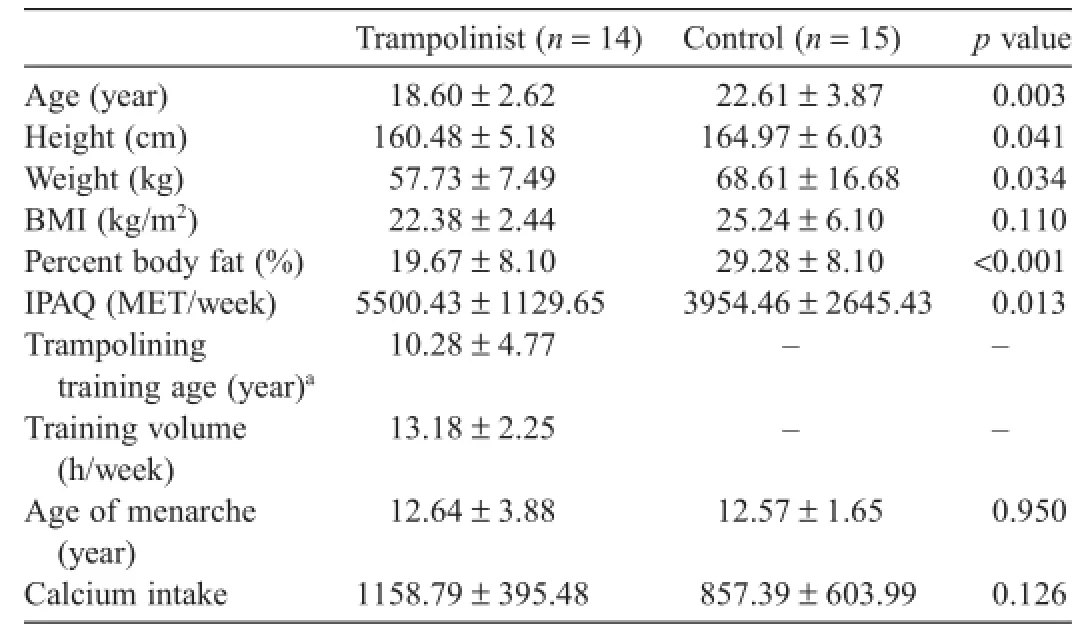
Table 1 Anthropometric and health characteristics of trampolinists compared with controls.
Hip and spine DXA,radius and tibia HR-pQCT and estimates of bone strength(radius and tibia)by FEA are outlined in Table 2.
Using DXA to assess skeletal parameters,trampolinists had greater aBMD at the TH(8%),FN(12%),and LS(9%)than controls(p<0.05).Using HR-pQCT,trampolinists had greater Tb.BMD at the tibia than controls(19%,p=0.001),with no other differences in density(total or cortical)observed between groups at either the radius or tibia.In addition to density differences,trampolinists had greater Tb.Th than controls at the tibia(18%,p=0.004),but not the radius(p=0.070).Finally, trampolinists had larger and stronger bones than controls at both the radius(7%larger Tt.Ar,p=0.040;21%higher failure load,p=0.001)and tibia(1%larger Tt.Ar,p=0.042;17% higher failure loadp<0.0001).
3.3.Muscle strength
Lean mass and muscle strength results are presented in Table 3.Derived from a total body DXA scan,trampolinists had more absolute lean mass than controls(3%,p<0.0001).At the upper body,there were no differences between groups for grip strength(p=0.837).At the lower body,trampolinists had greater KFT than controls(6%,p=0.011),however no differences were observed in KET(p=0.311).
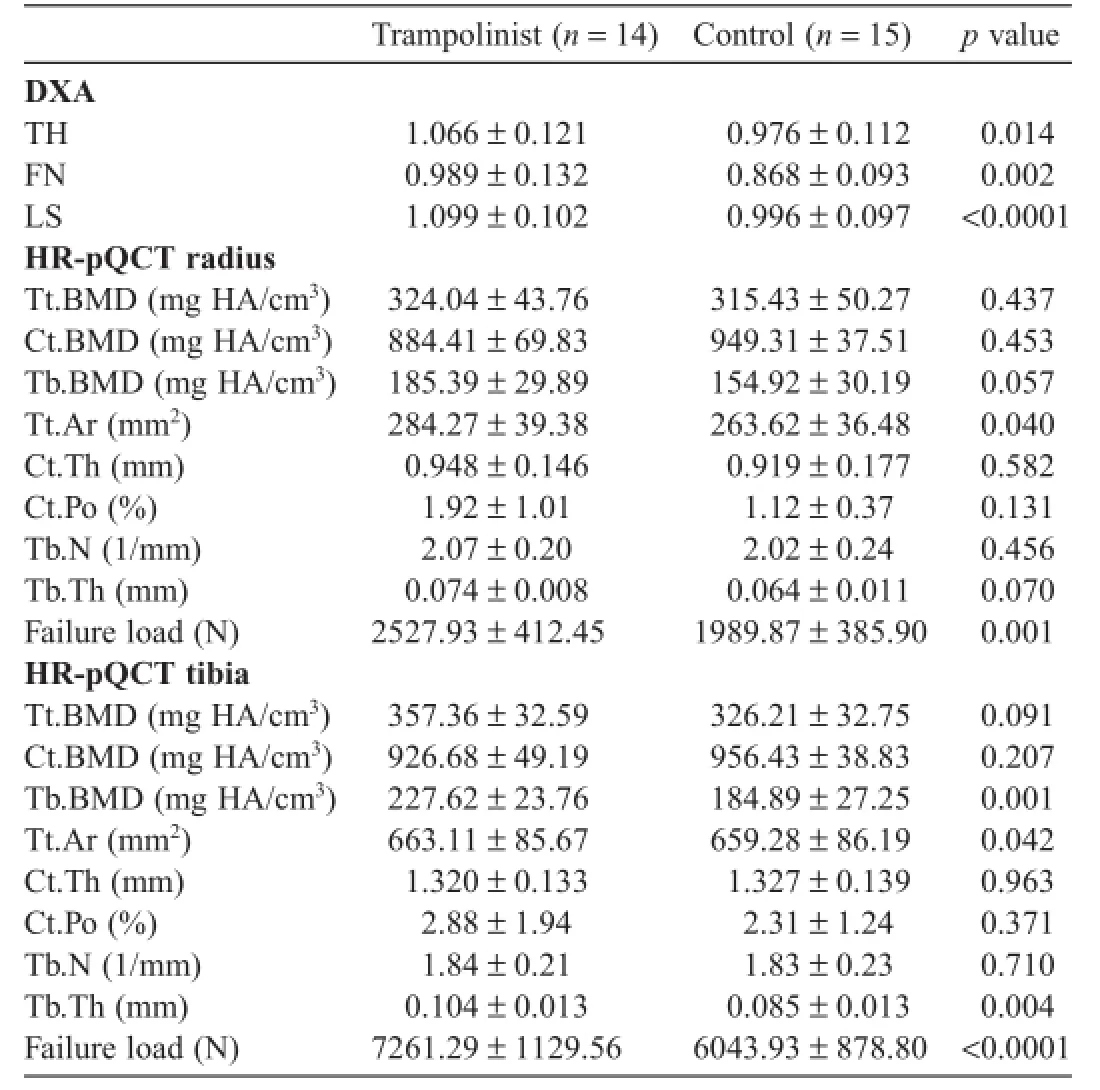
Table 2 DXA and HR-pQCT adjusted parameters for trampolinists and controls.
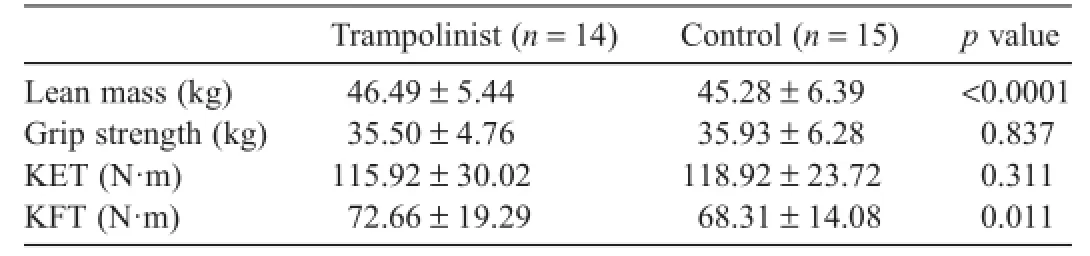
Table 3 Adjusted lean mass and muscle strength parameters for trampolinists and controls.
3.4.Predictors of bone strength
At the radius,age,height,and weight explained 21.1%of predicted bone strength,trampolining gymnastics participation explained 28.7%and grip strength did not significant y add to the model.At the tibia,age,height,and weight explained 37.0% of predicted bone strength,trampolining gymnastics participation explained 26.8%and KFT did not add to the model.A total of 49.8%of bone strength was explained by age,height,weight, and trampolining gymnastics participation at the radius and 63.9%at the tibia(Table 4).
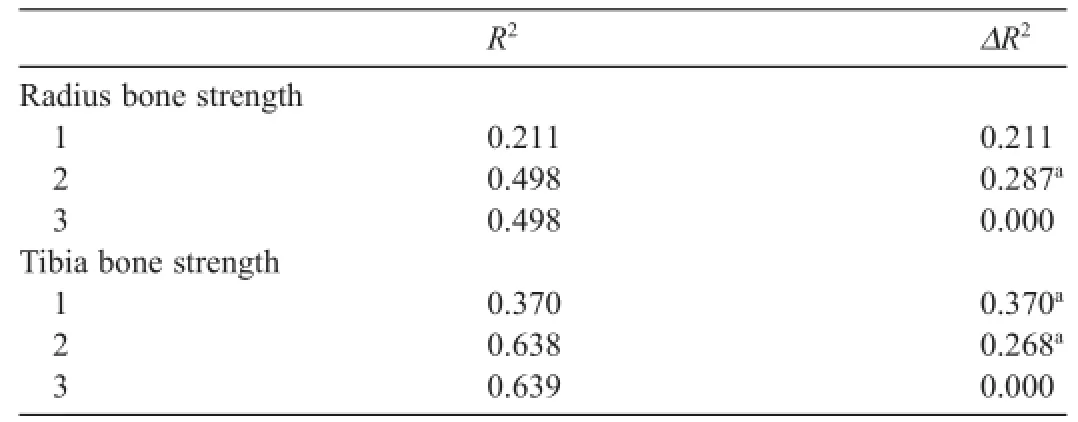
Table 4 Results from the regression analysis.
4.Discussion
This study shows a positive relationship between trampolining gymnastics participation and bone density,bone area,and bone microarchitecture in a female cohort.Musculoskeletal differences between trampolinists and controls were greater at the lower than upper extremities,which is consistent with the focus of trampolining activities.Specifical y,trampolinists had higher aBMD at the hip and spine,greater trabecular density and thicker trabeculae at the tibia as well as larger bones at both the tibia and radius.Trampolinists had higher KFT than controls with no difference in grip strength.Consistent with the bone microarchitecture and morphology,estimates of bone strength using FEA were greater for trampolinists than controls at both the radius and tibia.Overall,while undoubtedly both loading and muscle strength play a role in the higher bone strength of the trampolinists,our results suggest that loading may be the dominant factor contributing to greater bone strength.
We observed greater musculoskeletal differences between trampolinists and controls at the lower than upper extremities, which differs from other gymnastics studies where the difference is typically greater at the radius than tibia.29–32The greater musculoskeletal differences at the radius between gymnasts and controls in other disciplines are likely due to the unique upper limb mechanical loading33and enhanced upper body strength34,35associated with artistic gymnastics participation.In comparison, trampolining-based skills often involve single,double,or triple rotations about a vertical or transverse axis whereby no wrist contact is made with the trampoline,or minimal wrist contact is made with a rod floo(higher stiffness than a trampoline but lower than a gymnastics sprung floor)This differs from artistic gymnastics where the wrist may be exposed to impact forces varying from 1.0 to 4.1 times body weight from 30 to 90 times per 30 min of activity.36
At the radius,our trampolinists had stronger bones and a larger bone size than controls.These finding are consistent with previous studies on actively training32,37and retired29,30artistic gymnasts as well as other competitive athletes and controls.27,31,38However,unlike other gymnastics-based studies29,32,37we did not observe greater density(total or trabecular)at the radius in ourtrampolinists.This lack of between group differences in bone density,accompanied with an increase in bone size has been observed at the radius in female skiers and hurdlers,27,38aswellas retired artistic gymnasts.30This larger bone size without greater density is also common among children who participate in sport prior to and through pubertal growth.39Furthermore,it supports the theory that bone size and shape increases to accommodate for increased mechanical load.40At the radius,the greater estimate of bone strength observed in our trampolinists compared with controls is likely the result of greater bone size rather than improved microarchitecture.
At the tibia,our trampolinists had higher trabecular bone density,bone size,trabecular thickness,and bone strength than controls.Likely these positive skeletal observations at the trabecular compartment are the result of long-term repetitive loading via physical activity.41Within gymnastics studies specifical y,there have been a few reports of greater trabecular density with pQCT at the distal tibia for retired artistic gymnasts29,30and pre-pubertal artistic gymnasts32compared with controls.Another study using MRI to assess the proximal tibia observed advantages to the trabecular compartment in artistic gymnasts compared with controls.42In alignment with our results,the increase in trabecular density was driven by an increase in trabecular thickness rather than trabecular number.43Furthermore,thick dense trabeculae are required to overcome axial compressive forces such as those observed at the distal tibia.44This is supported,although cross-sectionally,by our results in which trampolinists had greater bone strength at the tibia compared with controls;however,the increase in bone size may have also contributed to the increase in bone strength observed at the tibia in our trampolinists.
Our results suggest the loading associated with trampolining gymnastics participation may be a greater contributor than muscle strength in determining bone strength at both the radius and tibia.In our models trampolining gymnastics participation explained 28.7%of the variance in bone strength at the radius and 26.8%at the tibia.At both sites,explained variance from muscle strength did not contribute to the overall model(<1%). While impact loading at the radius is minimal in trampolining, the trampolinists in this study participated in tumbling and strength-based activities in which site-specifi impact loading occurs.Even at the ankle,trampolinists would be exposed to lower ground reaction forces than artistic gymnasts.This is due to the surface difference between trampolines and artistic gymnastics sprung floors The trampoline has a lower stiffness than a gymnastics sprung floo (5000 kN/m compared with 120,000 kN/m),which allows large amounts of energy to be stored in the surface,45therefore decreasing the impact force transferred to the gymnast.We postulate that the explained variance of impact loading on bone strength may have been higher had our gymnasts been artistic gymnasts and not trampolinists.
The fact that impact loading but not muscle strength or power was a predictor of bone strength at the radius and tibia is in alignment with previous literature at the femoral neck.38In this previous study,impact loading predicted 13%of bone strength at the femoral neck.This percentage may have been higher if the athletes were all participating in high-magnitude loading activities rather than a combination of low-,odd-,and high-impact loading activities,which may explain why our explained variance was higher.
This study is limited by its cross-sectional design,which means we cannot rule out the possibility of self-selection bias in our cohort.It is possible that the trampolinists in our study were females with bigger,stronger bones and therefore more inclined to participate in trampolining gymnastics.The trampolinists in our study were younger,shorter,and lighter than the controls. Four trampolinists had previous experience in artistic gymnastics(range 2–8 years;retired for 2–10 years).These gymnasts were not different from the other gymnasts therefore all were included in the study.Trampolinists train and compete in trampoline,synchronized trampoline,tumbling and double-mini,all of which fall under the general discipline of trampolining gymnastics.We were unable to quantify the proportion of time spent training and competing on the different apparatus,which could have been different for each individual,and a function of competing at the provincialvs.national level.Furthermore,controls may have participated in unstructured physical activities for less than 3 h per week;however,we were unable to quantify this loading.While significant the larger bone size at the tibia should be interpreted with caution as it falls within the precision limits of the machine.Finally,we were unable to report total energy intake or vitamin D intake from food sources in this study.
5.Conclusion
To our knowledge,this is the firs study to investigate bone density,area,and microarchitecture in female trampolinists, and applied state-of-the-art imaging techniques based on HR-pQCT.Trampolinists’bone size and strength at both the radius and tibia was higher than controls.Furthermore,trampolinists have denser and thicker trabeculae coupled with a larger bone adding to higher bone strength,compared with controls.
Acknowledgment
The authors would like to thank all the participants who graciously devoted time to participate in the study,Michelle Kan for scan acquisition,and Scott Stanger for assistance in participant recruitment and data entry.
Authors’contributions
LAB and JDS designed the study and carried out data collection.LAB performed the statistical analyses.LAB,JDS, SKB drafted and revised the manuscript.All authors have read and approved the fina version of the manuscript,and agree with the order of authorship.
Competing interests
None of the authors declare competing financia interests.
1.Esposito PW,Esposito LM.The reemergence of the trampoline as a recreational activity and competitive sport.Curr Sports Med Rep2009;8:273–7.
2.Maxson DL,White C.Recreational trampoline use:injury rates and risks.J Occup Ther Sch Early Interv2009;2:217–20.
3.Loder RT,Schultz W,Sabatino M.Fractures from trampolines: results from a national database,2002–2011.J Pediatr Orthop2014;34:683–90.
4.McDermott C,Quinlan J,Kelly I.Trampoline injuries in children.J Bone Jt Surg Br2006;88:796–8.
5.Nysted M,Drogset JO.Trampoline injuries.Br J Sports Med2006;40: 984–7.
6.Dunbar SB,Carr-Hertel J,Lieberman HA,Perez B,Ricks K.A pilot study comparison of sensory integration treatment and integrated preschool activities for children with autism.IJAHSP2012;10:1–8.
7.Stanghelle J,Hjeltnes N,Bangstad H,Michalsen H.Effect of daily short bouts of trampoline exercise during 8 weeks on the pulmonary function and the maximal oxygen uptake of children with cystic fibrosisInt J Sports Med1988;9(Suppl.1):S32–6.
8.Giagazoglou P,Kokaridas D,Sidiropoulou M,Patsiaouras A,Karra C, Neofotistou K.Effects of a trampoline exercise intervention on motor performance and balance ability of children with intellectual disabilities.Res Dev Disabil2013;34:2701–7.
9.Aragao FA,Karamanidis K,Vaz MA,Arampatzis A.Mini-trampoline exercise related to mechanisms of dynamic stability improves the ability to regain balance in elderly.J Electromyogr Kinesiol2011;21:512–8.
10.Jensen P,Scott S,Krustrup P,Mohr M.Physiological responses and performance in a simulated trampoline gymnastics competition in elite male gymnasts.J Sports Sci2013;31:1761–9.
11.Burt LA,Greene DA,Ducher G,Naughton GA.Skeletal adaptations associated with pre-pubertal gymnastics participation as determined by DXA and pQCT:asystematic review and meta-analysis.J Sci Med Sport2013;16:231–9.
12.Dyson K,Blimkie C,Davison KS,Webber CE,Adachi JD.Gymnastic training and bone density in pre-adolescent females.Med Sci Sports Exerc1997;29:443–50.
13.Faul F,Erdfelder E,Lang AG,Buchner A.G*Power 3:a fl xible statistical power analysis program for the social,behavioral,and biomedical sciences.Behav Res Methods2007;39:175–91.
14.Hagstromer M,Oja P,Sjostrom M.The International Physical Activity Questionnaire(IPAQ):a study of concurrent and construct validity.Public Health Nutr2006;9:755–62.
15.Craig CL,Marshall AL,Sjöström M,Bauman AE,Booth ML,Ainsworth BE,et al.International Physical Activity Questionnaire(IPAQ):12-country reliability and validity.Med Sci Sports Exerc2003;35:1381–95.
16.Langsetmo L,Poliquin S,Hanley DA,Prior JC,Barr S,Anastassiades T, et al.Dietary patterns in Canadian men and women ages 25 and older: relationship to demographics,body mass index,and bone mineral density.BMC Musculoskelet Disord2010;11:20.doi:10.1186/1471-2474-11-20
17.Block G,Hartman AM,Naughton D.A reduced dietary questionnaire: development and validation.Epidemiology1990;1:58–64.
18.Willett WC,Sampson L,Stampfer MJ,Rosner B,Bain C,Witschi J,et al. Reproducibility and validity of a semiquantitative food frequency questionnaire.Am J Epidemiol1985;122:51–65.
19.Macdonald HM,Nishiyama KK,Kang J,Hanley DA,Boyd SK. Age-related patterns of trabecular and cortical bone loss differ between sexes and skeletal sites:a population-based HR-pQCT study.J Bone Miner Res2011;26:50–62.
20.Boutroy S,Bouxsein ML,Munoz F,Delmas PD.In vivoassessment of trabecular bone microarchitecture by high-resolution peripheral quantitative computed tomography.J Clin Endocrinol Metab2005;90: 6508–15.
21.Pauchard Y,Liphardt AM,Macdonald HM,Hanley DA,Boyd SK.Quality control for bone quality parameters affected by subject motion in high-resolution peripheral quantitative computed tomography.Bone2012;50:1304–10.
22.MacNeil JA,Boyd SK.Improved reproducibility of high-resolution peripheral quantitative computed tomography for measurement of bone quality.Med Eng Phys2008;30:792–9.
23.Buie HR,Campbell GM,Klinck RJ,MacNeil JA,Boyd SK.Automatic segmentation of cortical and trabecular compartments based on a dual threshold technique forinvivomicro-CT bone analysis.Bone2007;41:505–15.
24.Burghardt AJ,Buie HR,Laib A,Majumdar S,Boyd SK.Reproducibility of direct quantitative measures of cortical bone microarchitecture of the distal radius and tibia by HR-pQCT.Bone2010;47:519–28.
25.MacNeil JA,Boyd SK.Bone strength at the distal radius can be estimated from high-resolution peripheral quantitative computed tomography and the finit element method.Bone2008;42:1203–13.
26.Pistoia W,Van Rietbergen B,Lochmüller EM,Lill C,Eckstein F, Rüegsegger P.Estimation of distal radius failure load with micro-finit elementanalysis models based on three-dimensional peripheral quantitative computed tomography images.Bone2002;30:842–8.
27.Schipilow J,Macdonald H,Liphardt A,Kan M,Boyd S.Bone micro-architecture,estimated bone strength,and the muscle-bone interaction in elite athletes:an HR-pQCT study.Bone2013;56:281–9.
28.Canadian Society for Exercise Physiology.The Canadian physical activity, ftness,and lifestyle approach.3rd ed.Public Health Agency of Canada; 2004.
29.Ducher G,Hill B,Angeli T,Bass S,Eser P.Comparison of pQCT parameters between ulna and radius in retired elite gymnasts:the skeletal benefit associated with long-term gymnastics are bone and site-specificJ Musculoskelet Neuronal Interact2009;9:247–55.
30.Eser P,Hill B,Ducher G,Bass S.Skeletal benefitafter long-term retirement in former elite female gymnasts.J Bone Miner Res2009;24:1981–8.
31.Greene DA,Naughton GA,Bradshaw E,Moresi M,Ducher G. Mechanical loading with or without weight-bearing activity:influenc on bone strength index in elite female adolescent athletes engaged in water polo,gymnastics,and track-and-fieldJ Bone Miner Metab2012;30: 580–7.
32.Ward K,Roberts S,Adams J,Mughal M.Bone geometry and density in the skeleton of pre-pubertal gymnasts and school children.Bone2005;36: 1012–8.
33.Panzer V,Wood G,Bates B,Mason B.Lower extremity loads in landings of elite gymnasts.In:de Groot G,Hollander AP,Huijing PA,van IngenSchenau GJ,editors.BiomechanicsXI-B.Amsterdam:Free University Press;1988.p.727–35.
34.Scerpella T,Davenport M,Morganti C,Kanaley J,Johnson L.Dose related association of impact activity and bone mineral density in pre-pubertal girls.Calcifed Tissue Int2003;72:24–31.
35.Vicente-Rodriguez G,Dorado C,Ara I,Perez-Gomez J,Olmedillas H, Delgado-Guerra S,et al.Artistic versus rhythmic gymnastics:effects on bone and muscle mass in young girls.Int J Sports Med2007;28: 386–93.
36.Burt LA,Naughton GA,Higham DG,Landeo R.Training load in pre-pubertal female artistic gymnastics.Sci Gymnastics J2008;2:5–14.
37.Dowthwaite J,Scerpella T.Distal radius geometry and skeletal strength indices after peripubertal artistic gymnastics.Osteoporos Int2011;22: 207–16.
38.Nikander R,Sievanen H,Uusi-Rasi K,Heinonen A,Kannus P.Loading modalities and bone structures at nonweight-bearing upper extremity and weight-bearing lower extremity:a pQCT study of adult female athletes.Bone2006;39:886–94.
39.Haapasalo H,Kontulainen S,Sievanen H,Kannus P,Jarvinen M,Vuori I. Exercise-induced bone gain is due to enlargement in bone size without a change in volumetric bone density:a peripheral quantitative computed tomography study of the upper arms of male tennis players.Bone2000;27:351–7.
40.Frost HM,Schönau E.The“muscle-bone unit”in children and adolescents: a 2000 overview.J Pediatr Endocrinol Metab2000;13:571–90.
41.Kontulainen S,Sievanen H,Kannus P,Pasanen M,Vuori I.Effect of long-term impact-loading on mass,size,and estimated strength of humerusand radius of female racquet,sports players:aperipheralquantitative computed tomography study between young and old starters and controls.J Bone Miner Res2002;17:2281–9.
42.Modlesky C,Majumdar S,Dudley G.Trabecular bone microarchitecture in female collegiate gymnasts.Osteoporos Int2008;19:1011–8.
43.Notomi T,Okimoto N,Okazaki Y,Tanaka Y,Nakamura T,Suzuki M. Effects of tower climbing exercise on bone mass,strength,and turnover in growing rats.J Bone Miner Res2001;16:166–74.
44.Heinonen A,Sievanen H,Kannus P,Oja P,Vuori I.Site-specifi skeletal response to long-term weight training seems to be attributable to principal loading modality:a pQCT study of female weightlifters.Calcifed Tissue Int2002;70:469–74.
45.Stefanyshyn D,Nigg B.Work and energy influence by athletic equipment. In:Nigg B,MacIntosh B,Mester J,editors.Biomechanics and biology of movement.Champaign,IL:Human Kinetics;2000.p.49–65.
Received 8 August 2014;revised 18 November 2014;accepted 12 January 2015
Available online 30 April 2015
Peer review under responsibility of Shanghai University of Sport.
*Corresponding author.
E-mail address:skboyd@ucalgary.ca(S.K.Boyd).
http://dx.doi.org/10.1016/j.jshs.2015.01.007
2095-2546/©2016 Production and hosting by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
杂志排行

Journal of Sport and Health Science的其它文章
- Biomarker-guided classificatio scheme of neurodegenerative diseases
- Mechanism of neurodegeneration through tau and therapy for Alzheimer’s disease
- Examining the relationship between sport and health among USA women: An analysis of the Behavioral Risk Factor Surveillance System
- The microbiome,microbial-generated proinflammato y neurotoxins, and Alzheimer’s disease
- Longitudinal trajectories of physical activity in women using latent class growth analysis:The WIN Study
- Evidence of a conservative gait strategy in athletes with a history of concussions