Validity and reliability of three methods of stiffness assessment
2016-02-05ElizethPruynMrkWtsfordAronMurphy
Elizeth C.Pruyn*,Mrk L.WtsfordAron J.Murphy
aFaculty of Health,University of Technology Sydney,Lindfeld,NSW 2070,Australia
bSchool of Science and Technology,University of New England,Armidale,NSW 2351,Australia
Validity and reliability of three methods of stiffness assessment
Elizabeth C.Pruyna,*,Mark L.Watsforda,Aron J.Murphyb
aFaculty of Health,University of Technology Sydney,Lindfeld,NSW 2070,Australia
bSchool of Science and Technology,University of New England,Armidale,NSW 2351,Australia
Background:Stiffness is commonly assessed in relation to injury and athletic performance.The purpose of this research was to compare the validity and reliability of 3in vivomethods of stiffness assessment using 1 cohort of participants.
Methods:To determine inter-day reliability,15 female netballers were assessed for stiffness twice within 1 week using unilateral hopping(vertical stiffness),free oscillations of the calf,and myometry of various muscles of the triceps surae.To establish convergent construct validity,stiffness was compared to static and dynamic strength measurements.
Results:Test–retest stiffness results revealed that vertical stiffness produced moderate to high reliability results and myometry presented moderate to very high reliability.In contrast,the free oscillation technique displayed low to moderate reliability.Vertical stiffness demonstrated a significa t correlation with rate of force development during a squat jump,whilst myometer stiffness measurements from 3 sites in the lower limb revealed significan correlations with isometric rate of force development.Further,significan negative correlations were evident between the eccentric utilisation ratio and various myometer stiffness results.No relationships were established between the free oscillation technique and any of the performance measurements.
Conclusion:These results suggest that vertical stiffness and myometry are valid and reliable methods for assessing stiffness.
©2016 Production and hosting by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Calf stiffness;Free oscillation technique;Myometry;Myoton-Pro;Vertical hop test;Vertical stiffness
1.Introduction
In a mechanical context,stiffness refers to a body resisting an applied change in length.1,2Butler and colleagues3explain that the concept of stiffness involves deformable bodies that store and return elastic energy.Relatively high stiffness in humans has previously been related to increased risk of repetitive stress injuries as well as soft-tissue injuries such as hamstring strains.4–6Further,stiffness has been related to performance of stretch–shorten cycle activities.7–10Since athletes strive to remain injury free and to perform optimally,stiffness is an important screening marker for physiotherapists,coaches,strength and conditioning trainers,and other practitioners.As detailed by Hooke’s Law,the force required to deform the body is equal to the spring constant multiplied by the distance of deformation.3The spring constant relates to the innate stiffness of the body;thus,to calculate stiffness,the required force and the distance of deformation aremeasured.Many techniques have been successfully implemented to distinguish between relatively stiff or relatively compliant participants.These include ultrasonography,11the quick-release technique,12,13the vertical hop test,1myometry,14and the free oscillation technique.15The current study will focus on the latter 3,as they are relatively simple to administer,and allow for relatively large cohorts to be tested within restricted time frames. Situations such as these are particularly relevant when testing professional athletes or conducting large-scale fiel studies.
The vertical hop test was initially outlined by McMahon and Cheng1and typically involves unilateral hopping on a force platform.Excellent levels of reliability have been reported16and the test is logistically simple to administer requiring the measurement of only 2 mechanical parameters:ground reaction force(GRF)and centre of mass displacement(ΔCOM).17Although relatively simple to administer,the nature of the calculation makes many assumptions.Firstly,it assumes that vertical stiffness(Kvert)remains constant during hopping.However, it has been reported that Kvertincreases inversely with ground contact time,18and linearly with hopping height.19,20Thus, inherent differences in hopping techniques between individualsmay affect the reliability and validity of this measurement of stiffness.
A further assumption of the vertical hop test is that the human leg works as a single linear spring,and that all components of the leg equally contribute to Kvert.However,ankle joint stiffness was reported as the primary modulator of Kvertduring hopping.20Whilst this method involves some assumptions,it is a global,inclusive,and functional measurement of lower-body stiffness.
The free oscillation technique assesses the stiffness of a limb segment based on the assumption that human muscles behave like a damped spring system.15This assumption suggests that if any perturbation is applied whilst under load,the system will oscillate at a damped natural frequency due to the nature of the muscle and tendon structures.21In a damped spring system, when a perturbation is applied,the damping coefficien causes the subsequent oscillations to subside over time.The free oscillation technique for stiffness assessment has been widely used in previous studies15,22–24and has generally been proven to be valid and reliable.24Whilst the validity and reliability of these methods have been proven to be strong,accessibility issues may arise due to the limited mobility of the assessment apparatus.Further, procedures often require the assessment of a maximum voluntary contraction prior to stiffness assessment,which requires a greater length of time per testing session.
A further method of stiffness measurement is through the use of a myometer,an electronic device that is capable of recording multiple characteristics related to muscular tone such as tension,elasticity,and stiffness.14Muscle stiffness calculation by myometry involves a small perturbation from the device applied to the skin covering the muscle.An accelerometer then measures the deformation characteristics of the muscle and calculates stiffness using the damped natural oscillations exhibited by the recoil characteristics of the muscle.14,25Commonly reported myometer models include the Myoton-2,Myoton-3, and more recently,the Myoton-Pro.
The Myoton-2 reportedly has a high level of inter-observer repeatability14and inter-day reliability.25The sensitivity of the device25and its ease of use14have been commended;however,its weakness was that it was solely suitable for surface musculature.14The Myoton-3 reportedly displays excellent absolute inter-day reliability26and significan correlations when evaluating concurrent and predictive validity.27Zinder and Padua28also reported good reliability and construct validity,noting an advantage of the device was its ability to measure isolated muscles.The Myoton-Pro has shown very high to excellent within-day reliability,and good to high between-day reliability.29However,to the best of the authors’knowledge,there are no previous reports of the validity of this device.
It is important to establish the reliability and validity of data collection techniques to ensure any subsequent results are true and consistent.Whilst there have been separate reports of validity and reliability for each individual technique,no previous literature has compared the 3 techniques using the same cohort of participants.24,25Further,no previous study has evaluated the validity and reliability of the Myoton-Pro device.Thus,the aim of the current study was first y to determine the convergent construct validity when compared to performance variables and the inter-day reliability of a new device to measure stiffness(Myoton-Pro),and secondly to compare the inter-day reliability and convergent construct validity of the vertical hop test,myometry,and the free oscillation technique.Knowledge of validity and reliability can assist with sample size calculations,as well as contribute to study design and development of appropriate methodology for future studies.
2.Materials and methods
2.1.Participants
Fifteen females who competed at various levels of competitive netball in the 2012 season,including New South Wales State League and club A-grade,volunteered to participate in this study.Participants were excluded from the study if they had sustained an injury within 3 months of testing,or fell outside the age range of 18–35 years.The study was approved by the Human Research Ethics Committee of the University of Technology,Sydney,and a written informed consent was obtained from each participant.
2.2.Procedures
The participants were assessed for stiffness twice within 1 week.To avoid any possible effects of fatigue,testing was conducted at least 48 h after competition,and sessions were at least 24 h apart.In order to maintain consistency of measurements,stiffness was assessed using 3 methods in the same order (myometry,followed by the free oscillation technique,and followed by the vertical hop test)and at the same time of day on each occasion.The participants were instructed not to deviate from their regular training patterns.In addition,the participants completed various performance tests following stiffness assessment during the firs session only,to determine the convergent construct validity of the stiffness assessment methods.Prior to the commencement of Session 1,the participants were weighed on digital scales(Tanita,Sydney,Australia)and body mass was recorded to the nearest 0.1 kg.A 5 min warm-up on a stationary bike was then conducted with a required power output of 100 W.
2.2.1.Static strength measurements
The maximum isometric force(MIF)and rate of force development(RFD)during a unilateral isometric calf raise was measured with participants positioned in a seated calf raise machine with a mechanical winch attached(Fig.1A).Hip,knee,and ankle joints were aligned at 90°,with the winch adjusted to fi this position during contraction.The participants were instructed to produce maximal force against the knee pad as fast as possible,holding for 3 s.The force data were collected via the load cell(Chase Engineering,Perth,Australia)at a rate of 1000 Hz. MIF was calculated as the peak of the force curve,whilst isometric RFD(RFDiso)was determined as the peak value of the derivative of the force curve using a 5 ms interval.9Two trials were completed on each leg,and the greatest MIF value for each limb was used to determine subsequent loads for stiffness assessment.
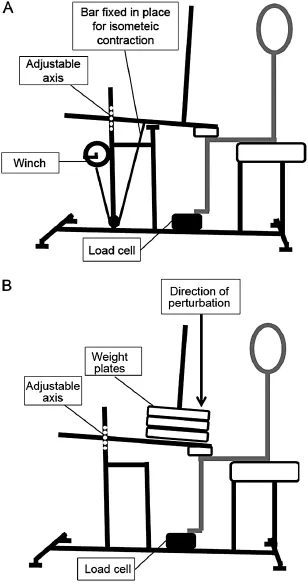
Fig.1.Diagrammatic representation of the seated calf raise machine(A)with a winch attached for an isometric contraction of the lower leg,and(B)loaded with weight plates for the free-oscillation technique.
2.2.2.Dynamic strength measurements
The participants performed 2 counter-movement jumps (CMJ)on a 1-dimensional force plate(Onspot,Wollongong, Australia)which was calibrated to a series of known masses prior to commencement.CMJ technique was in accordance with previous methods.11The researcher gave instructions to jump for maximum height,whilst keeping hands on hips during the jump and landing.Researchers did not intervene to adjust the knee angle during the eccentric phase of the jump.Participants also completed 2 squat jumps(SJ)using the same apparatus and guidelines as the CMJ;however,they were additionally instructed to squat to a knee angle of 90°(as checked by a goniometer)and hold for 3 s before jumping.The force curve was examined immediately following each SJ,to ensure that no eccentric movement occurred prior to the concentric movement. Jump height and RFD were determined from the force data for each jump,and the results from the jump with the greatest jump height were recorded for further analysis.To determine the elastic component contribution,the eccentric utilisation ratio (EUR)was calculated using CMJ height and SJ height:

with a higher ratio indicating a greater contribution from the elastic component to CMJ performance.30
2.2.3.Vertical hop test
A vertical hop test was used to assess Kvert.The participants were instructed to hop unilaterally on the 1-dimensional force plate in time to a digital metronome(Seiko,Tokyo,Japan)set at 2.2 Hz.16,19,20To eliminate the cushioning effect of footwear and any contribution from the upper body,the test was performed barefoot with participants’hands remaining on their hips throughout.Once steady-state hopping was achieved,10 s of force data were collected at 1000 Hz.Trials were accepted if at least 3 hops were within±2%of the prescribed frequency,16with a re-trial performed if frequency criteria were not met.Each participant completed the test for both right and left legs.Kvertwas calculated as the ratio of peak GRF to the maximum ΔCOM.16,31ΔCOM was calculated by a double integration of the acceleration curve and the integration constant was set to assume that the lowest COM point occurred at the same time as peak GRF.32The mean stiffness score of 3 consecutive hops was divided by body mass to produce a score relative to individual size.
2.2.4.Free-oscillation technique
Calf stiffness(Kcalf)was assessed using the free oscillation technique(Fig.1B).23,24,33To isolate the musculature of the lower leg,the participants were positioned in the seated calf raise machine,with a prescribed load situated directly above the knee (Fig.1B).Once an angle of 90°at both the knee and ankle joint was achieved,an external downward force of 100–200 N8,10,15was rapidly applied to the system by the researcher setting the lower leg into oscillation.34Since the perturbations were applied manually,slight magnitude variations were expected,but were not considered to alter stiffness values as an elastic system will oscillate at its natural frequency regardless of the magnitude of applied force.23To reduce the effects of neural responses to the perturbation,the subjects were instructed not to intervene throughout the test.To assist,arms were positioned across their chest,the opposite foot was elevated,and eyes were closed during each trial.Force data were collected at 1000 Hz via a load cell situated beneath the metatarsals(Fig.1B),and the force profil was analysed after every trial to ensure that oscillations were free from subject intervention.
Custom-made software was employed to calculate Kcalf.The damped oscillations(Fig.2)were modelled to a second-order linear equation,and the damping coefficien was calculated using the natural frequency as outlined in the literature.24Kcalfwas determined by the following equations:

wheremis the mass of the system,fis the damped natural frequency(1/T;Fig.2)andcis the damping coefficien(equation 2)wherefnis the natural frequency of the system andsis the damping ratio.23
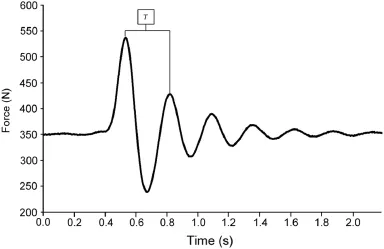
Fig.2.Representation of resultant damped oscillations following the application of a perturbation during the free oscillation technique.T=time between successive peaks.
The assessment load was prescribed at 70%of the participants’previously determined MIF(Kcalf70%).This load was selected as it has been demonstrated as the equivalent of maximal stiffness.15,24Further,an absolute load of 20 kg(Kcalf20 kg)was also implemented unilaterally to provide the ability to compare the stiffness derived from a consistent load across all participants.Two trials were performed on each leg,with the mean score of the 2 accepted as the Kcalffor each condition.
2.2.5.Myometry
A myometer was used to measure the stiffness of 4 points on each of the participants’lower limbs:lateral gastrocnemius (LG),medial gastrocnemius(MG),soleus(SOL),and Achilles aponeurosis(ACH).To maintain consistency between participants and between days,assessment points were drawn with a marker,and identical points were measured on the second testing occasion.The participants were required to be barefoot with the lower leg exposed.Measurements were collected using the latest model of a hand-held myometer,the Myoton-Pro (Myoton AS,Tallinn,Estonia),and were measured under 3 different conditions:lying,standing,and contracted.Lying involved the participants lying prone on an assessment table, with feet hanging off the table at an ankle angle of 90°.Standing measurements involved participants standing in anatomical position.Measurements for the contracted condition were collected with participants positioned in the seated calf raise machine,maintaining a position where the ankle joint was 90° whilst performing an isometric contraction equivalent to 70%MIF.Visual feedback was provided to ensure that a contraction equivalent to 70%MIF was maintained.
Myometer measurements were achieved by holding the device immediately above the skin overlaying the assessment site.Once the desired position was achieved,a mechanical impact(duration:15 ms;force:0.3–0.4 N)was delivered to the muscle by a mechanical probe,causing the tissue to deform for a brief period of time.Following this,the resultant damped natural oscillations25were recorded via an in-built accelerometer,sampled at 3200 Hz.26Stiffness was calculated as the ratio between the force applied and the muscle deformation.26Three consecutive measurements were taken at each site in each position,with the mean value used for analysis.
2.3.Statistical analysis
2.3.1.Reliability
To establish the inter-day reliability of each of the stiffness measurements,each test was assessed for systematic bias by determining paired differences by Student’sttest.Indexes of relative reliability,the intra-class correlation(ICC),35and absolute reliability,the coefficien of variation(CV)35,36were also calculated for each stiffness measurement.ICC results were interpreted based on the classificatio scale:very high(0.90–1.00),high(0.70–0.89), moderate(0.50–0.69),and low(0.26–0.49).37Finally,percentage standard error of measurement(%SEM)was calculated to determine the precision of each stiffness measurement.
2.3.2.Convergent construct validity
Each set of data was tested for normality using the Shapiro–Wilk test.To determine the convergent construct validity of each of the stiffness measurements,Pearson’s product moment correlations were investigated for 5 performance variables including static strength measures(MIF and RFDiso)and dynamic strength measures(CMJRFD,SJRFD,and EUR).Relationships have previously been established between stiffness and similar neuromechanical outputs,8,15,24hence their inclusion to establish convergent construct validity.When compared to unilateral static strength measurements(MIF,RFDiso),left and right legs were considered individually,resulting in a sample size of 30.When compared to bilateral dynamic strength measurements (CMJRFD,SJRFD,EUR),the mean value of left and right stiffness measurements was taken,resulting in a sample size of 15.Pearson’srvalue was used to determine the strength of the relationship,with thepvalue indicating if the relationship was significant The magnitude of the correlations were interpreted based on the scale:perfect(1.00),nearly perfect(0.90–0.99), verylarge(0.70–0.89),large(0.50–0.69),moderate(0.30–0.49), small(0.10–0.29),and trivial(0.00–0.09).38For all procedures, statistical significanc was accepted at anαlevel of 0.05.
3.Results
Fifteen female netballers(age:23.51±2.86 years;height: 1.71±0.06 m;mass:70.18±8.19 kg)participated in this study.Mean stiffness values for each assessment method and each condition are reported in Tables 1 and 2.The results from Day 1 and Day 2 were compared to assess the test–retest reliability of each method.To determine the convergent construct validity of the methods,the stiffness results from Day 1 were compared to the MIF,RFDiso,CMJRFD,and EUR(Table 3) also collected on Day 1.
Comparison of Day 1vs.Day 2 stiffness results revealed that the vertical hop test produced moderate to high relative reliability results,whilst the results for the free oscillation technique at both 70%MIF and 20 kg were low to moderate (Table 1).Relative reliability results for the myometer weremoderate to very high with ICC values ranging from 0.69 to 0.98 for the various conditions(Table 2).Further,myometer results collected in lying and standing positions showed a higher level of relative reliability when compared to myometer results collected in the seated calf raise machine(Table 2).
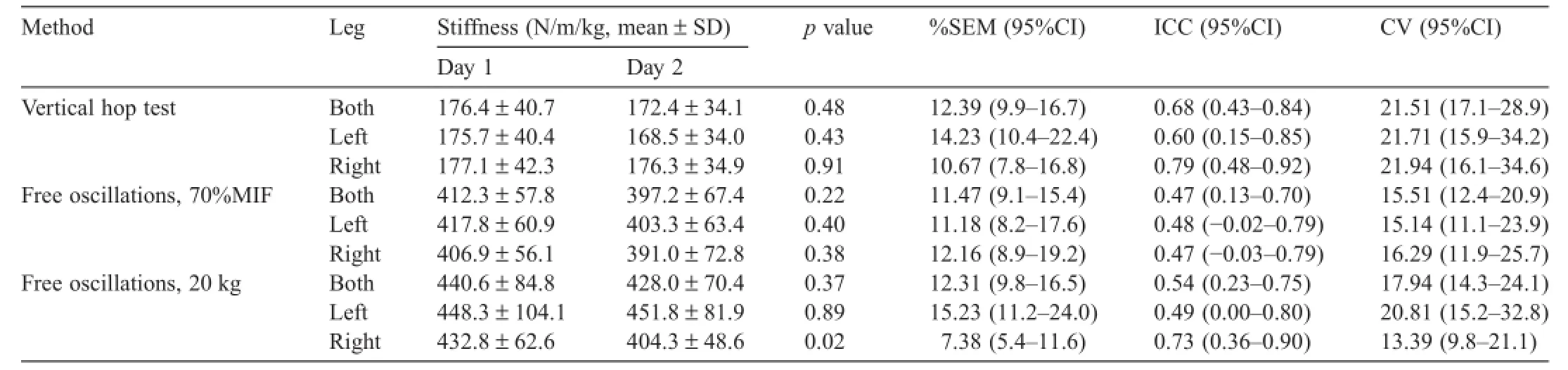
Table 1 Summary of reliability results for vertical hop test and free oscillation technique.
In terms of absolute reliability,results were questionable, with CV values ranging from 12.88%to 35.23%(Tables 1 and 2).Myometry in the lying and standing positions displayed more precision of measurement(%SEM 3.34–7.75)when compared to myometry in the seated calf raise machine(%SEM 7.15–17.41),vertical hop test(%SEM 10.67–14.23),and free oscillation technique under both loads(%SEM 7.38–15.23). Systematic bias was not present in any of the variables measured,with the exception of 2:free oscillation technique for the right leg with a 20 kg load(p=0.02),and myometry of LG in the seated calf raise machine(p=0.02)(Tables 1 and 2).
Validity results are presented in Table 4.All datasets displayed normality,with the exception of myometer measurements of SOL in the lying position.Grubb’s test for outliers was utilised to eliminate 2 outlying scores for that set of data,and the remaining data were normally distributed.Thus,the sample size for myometer measurements of SOL in the lying position was reduced to a sample size of 26 for unilateral performance measurements and 13 for bilateral performance measurements.
Data from the vertical hop test demonstrated a significan correlation with SJRFD(Table 4).Significan positive correlations were revealed between RFDisoand myometer measurements of LG,MG,and ACH,in a lying position(Table 4). Similarly,for lying,there was a significan positive correlation between MIF and the myometer measurement of ACH.Conversely,significan and large negative correlations were evident between EUR and myometer measurements of various sites and in various positions(Table 4).No significan relationship was established between the free oscillation technique and any performance measurements.
4.Discussion
The current study was designed to establish the inter-day reliability and convergent construct validity of 3 methods of assessing stiffness using an athletic cohort.It was the firs to compare the vertical hop test,free oscillation technique,and myometry,and the results will influenc future research design, especially when dealing with neuromechanical assessment of the lower body.
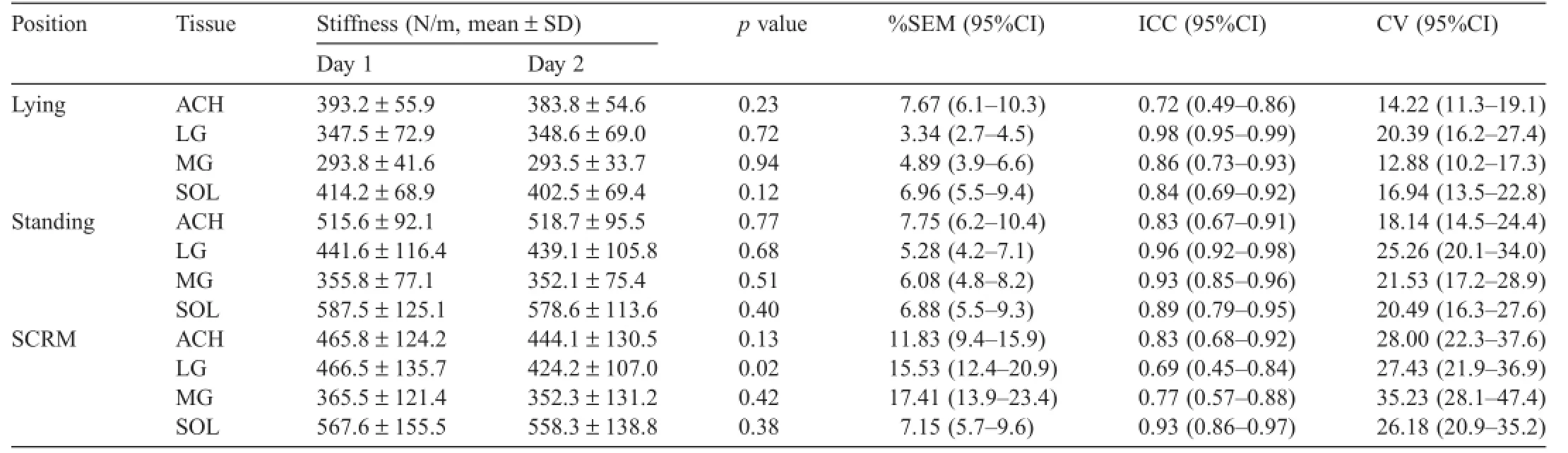
Table 2 Summary of reliability results for myometry under various conditions.
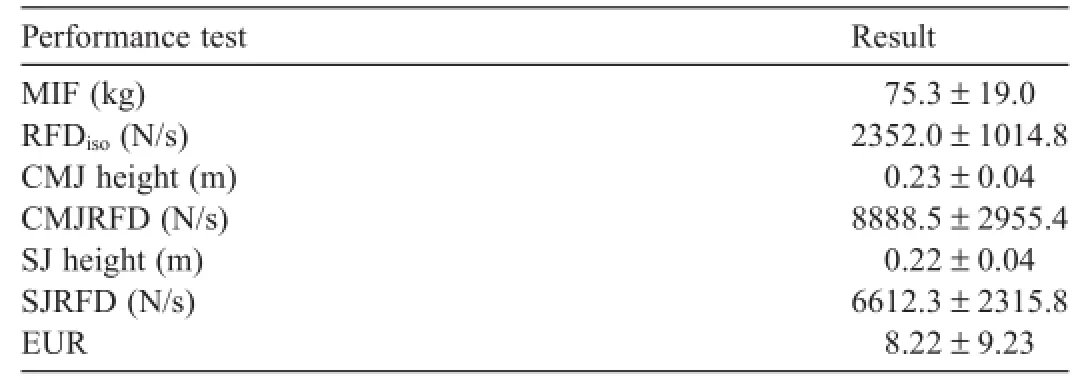
Table 3 Summary of performance test results(mean±SD).
An important result of the current study was the good relative reliability demonstrated for the vertical hop test.These results were congruent with previous reports of good relative reliability for similar methodologies.16,39In previous studies,a high ICC value(0.8)was reported when a unilateral vertical hop test was administered to males,39and high to very high ICC values(0.85–0.94)were reported for females;16however,this study conducted bilateral hopping at various frequencies.The ICC results for the vertical hop test in the current study displayed similar levels of relative reliability,ranging from moderate to high.Interestingly,the absolute reliability of the vertical hop test was questionable,with CV scores ranging from 21.51%to 21.94%.Nevertheless,the good relative reliability and lack of systematic bias suggest that the vertical hop test is a reliable measurement of stiffness.
When determining the convergent construct validity of the vertical hop test,Pearson’s correlations revealed a significan positive correlation between Kvertand SJRFD.These results were hypothesised considering the previously reported relationshipbetween lower body stiffness and concentric RFD.24Interestingly, there was no significan correlation between Kvertand RFDiso; however,given the differences in contraction types,such a relationship may not have been warranted.Since a criterion reference measure for lower body stiffness does not exist,concurrent validity cannot be established;however,the results from the current study suggest that the vertical hop test is a reliable tool for assessing lower body stiffness.Further,positive correlations between Kvertand dynamic strength measurements suggest that it is related to the construct of stiffness.
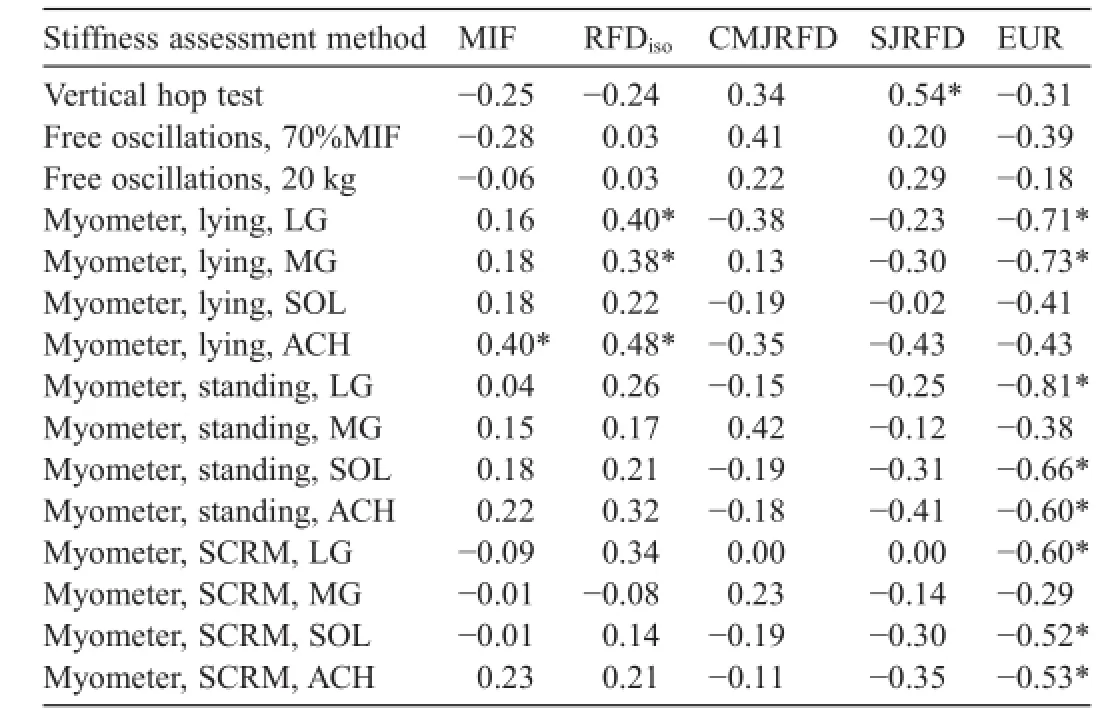
Table 4 Pearson’s correlations between measures of stiffness and selected performance variables.
Many key finding relating to myometry were also revealed in the current study.Stiffness results obtained from the Myoton-Pro showed excellent levels of relative reliability in all positions,particularly standing and lying.The same variables also displayed the lowest%SEM scores in the current study,demonstrating a high level of precision of measurement.Previous reports using the Myoton-Pro have shown good to very good within-day and inter-day inter-rater reliability when measuring the stiffness of the rectus femoris in a lying position,40and good to excellent between-day and within-session reliability when measuring the stiffness of the biceps femoris and rectus femoris in a lying position.29Similarly good reliability results have also been reported for stiffness data collected with superseded Myoton models.14,25,28
When assessing for convergent construct validity,the data collected using the myometer presented a number of significan correlations with the various performance parameters.Signifi cant positive correlations were determined between myometer stiffness of LG,MG,and ACH collected in the lying position and RFDiso.This is consistent with reports of a relationship between increased rate of contraction and increased stiffness.9,24Interestingly,large(0.50–0.69)and very large(0.70–0.89)inverse correlations were revealed between myometer stiffness collected under all 3 conditions and EUR results.Specificaly,very large inverse correlations were revealed between EUR results and myometer stiffness measurements of LG in both lying and standing positions,and MG in a lying position.Further,large inverse correlations were also observed between EUR results and ACH and SOL in the standing position.These results are consistent with previous reports where relatively compliant subjects have shown a greater pre-stretch augmentation15,24and hence,greater elastic energy contribution to concentric movement.Based on these results,stiffness measurements collected by a myometer under passive conditions(lying and standing) appear to be related to dynamic muscle activities.Further,it appears that stiffness measurements by way of myometry are more relevant for the gastrocnemius musculature in the lying position,and SOL andACH in the standing position.
The validity and reliability results for the free oscillation technique at both 70%MIF and 20 kg loads were poor.This is in direct contrast to a previous report of good reliability for the free oscillation technique measured at a load relative to 75%MIF in the same position as utilised in the current study.8This study also reported large and significan correlations between stiffness and RFDisobilaterally,and stiffness and MIF unilaterally.Similarly, good reliability has been reported for the free oscillation technique measured at various loads in a supine maximal isometric legpress.24Further,the same study reported a large and significan correlation when comparing stiffness to RFDisoand SJRFD.In contrast to the current study,both the previous reports involved male subjects.Significan differences in male and female stiffness levels have been suggested,28,41,42conceivably due to betweengender differences in:muscle mass and cross-sectional area,43tendon viscoelastic properties,41the thickness,length and pennation angle of muscle fibres41muscle recruitment strategies,42or leg posture during hopping.42The between-gender difference in stiffness could account for the differing reports of validity and reliability between those with male participants,and those with females.Regardless,it appears that stiffness results obtained using the free oscillation technique under the conditions in the current study should not be considered reliable and are not related to dynamic strength measurements.
The results from the current study are limited by various assumptions that exist in the methodology and calculation of stiffness.The vertical hop test assumes that the leg works as one linear mechanical spring,and the free oscillation technique and myometry assume the region or muscle will oscillate according to the damped spring model.A further limitation of the study is the use of convergent construct validity rather than criterionreferenced validity.Future research to establish a criterionreference measure of lower-body stiffness would certainly be warranted.
5.Conclusion
The results from the current study demonstrate that the use of either the vertical hop test or myometry will produce valid and reliable results for the assessment of stiffness.These results are favorable to researchers,as both methods are relatively simple to administer,allowing for a potentially large cohort to be tested, and are performed under low-load conditions,posing minimal risk to participants.Further,since the vertical hop test can provide a“global”measure of lower body stiffness,whereas myometry measures the stiffness of isolated muscles,it may be suggested that a combination of both methods would provide an excellent representation of the stiffness levels of the lower body.
Authors’contributions
ECP was involved in participant recruitment,data collection,data reduction,statistical analysis and manuscript editing; MLW conceived of the study,assisted with statistical analysis and manuscript editing;AJM was involved in study design and editing the manuscript.All authors have read and approved the fina version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
None of the authors declare competing financia interests.
1.McMahon TA,Cheng GC.The mechanics of running:how does stiffness couple with speed?J Biomech1990;23:65–78.
2.Seyfarth A,Geyer H,Gunther M,Blickhan R.A movement criterion for running.J Biomech2002;35:649–55.
3.Butler RJ,Crowell 3rd HP,Davis IM.Lower extremity stiffness: implications for performance and injury.Clin Biomech(Bristol,Avon)2003;18:511–7.
4.Ekstrand J,Gillquist J.The avoidability of soccer injuries.Int J Sports Med1983;4:124–8.
5.Pruyn EC,Watsford ML,Murphy AJ,Pine MJ,Spurrs RW,Cameron ML, et al.Relationship between leg stiffness and lower body injuries in professional Australian football.J Sports Sci2012;30:71–8.
6.Watsford ML,Murphy AJ,McLachlan KA,Bryant AL,Cameron ML, Crossley KM,et al.A prospective study of the relationship between lower body stiffness and hamstring injury in professional Australian Rules footballers.Am J Sports Med2010;38:2058–64.
7.Bret C,Rahmani A,Dufour AB,Messonnier L,Lacour JR.Leg strength and stiffness as ability factors in 100 m sprint running.J Sports Med Phys Fitness2002;42:274–81.
8.Murphy AJ,Watsford ML,Coutts AJ,Pine MJ.Reliability of a test of musculotendinous stiffness for the triceps-surae.Phys Ther Sport2003;4:175–81.
9.Spurrs RW,Murphy AJ,Watsford ML.The effect of plyometric training on distance running performance.Eur J Appl Physiol2003;89:1–7.
10.Wilson GJ,Murphy AJ,Pryor JF.Musculotendinous stiffness:its relationship to eccentric,isometric,and concentric performance.J Appl Physiol1994;76:2714–9.
11.Kubo K,Yata H,Kanehisa H,Fukunaga T.Effects of isometric squat training on the tendon stiffness and jump performance.Eur JAppl Physiol2006;96:305–14.
12.Lambertz D,Mora I,Grosset JF,Perot C.Evaluation of musculotendinous stiffness in prepubertal children and adults,taking into account muscle activity.J Appl Physiol2003;95:64–72.
13.Lambertz D,Perot C,Kaspranski R,Goubel F.Effects of long-term spacefligh on mechanical properties of muscles in humans.JAppl Physiol2001;90:179–88.
14.Viir R,Laiho K,Kramarenko J,Mikkelsson M.Repeatability of trapezius muscle tone assessment by a myometric method.J Mech Med Biol2006;6:215–28.
15.Wilson GJ,Wood GA,Elliott BC.Optimal stiffness of series elastic component in a stretch-shorten cycle activity.JAppl Physiol1991;70:825–33.
16.McLachlan KA,Murphy AJ,Watsford ML,Rees S.The interday reliability of leg and ankle musculotendinous stiffness measures.J Appl Biomech2006;22:296–304.
17.Brughelli M,Cronin J.A review of research on the mechanical stiffness in running and jumping:methodology and implications.Scand J Med Sci Sports2008;18:417–26.
18.Arampatzis A,Schade F,Walsh M,Bruggemann GP.Influenc of leg stiffness and its effect on myodynamic jumping performance.J Electromyogr Kinesiol2001;11:355–64.
19.Farley CT,Blickhan R,Saito J,Taylor CR.Hopping frequency in humans: a test of how springs set stride frequency in bouncing gaits.JAppl Physiol1991;71:2127–32.
20.Farley CT,Morgenroth DC.Leg stiffness primarily depends on ankle stiffness during human hopping.J Biomech1999;32:267–73.
21.Watsford ML,Murphy AJ,Spinks WL,Walshe AD.Creatine supplementation and its effect on musculotendinous stiffness and performance.J Strength Cond Res2003;17:26–33.
22.Cavagna GA.Elastic bounce of the body.J Appl Physiol1970;29:279–82.
23.Shorten MR.Muscle elasticity and human performance.In:Van Gheluwe B,Atha J,editors.Current research in sports biomechanics.Basel:Karger; 1987.p.1–18.
24.Walshe AD,Wilson GJ,Murphy AJ.The validity and reliability of a test of lower body musculotendinous stiffness.Eur J Appl Physiol Occup Physiol1996;73:332–9.
25.Bizzini M,Mannion AF.Reliability of a new,hand-held device for assessing skeletal muscle stiffness.Clin Biomech(Bristol,Avon)2003;18:459–61.
26.Ditroilo M,Hunter AM,Haslam S,De Vito G.The effectiveness of two novel techniques in establishing the mechanical and contractile responses of biceps femoris.Physiol Meas2011;32:1315–26.
27.Chuang LL,Wu CY,Lin KC.Reliability,validity,and responsiveness of myotonometric measurement of muscle tone,elasticity,and stiffness in patientswith stroke.ArchPhysMedRehabil2012;93:532–40.
28.Zinder SM,Padua DA.Reliability,validity,and precision of a handheld myometer for assessingin vivomuscle stiffness.J Sport Rehabil2011;6:1–8.
29.Mullix J,Warner M,Stokes M.Testing muscle tone and mechanical properties of rectus femoris and biceps femoris using a novel hand held MyotonPRO device:relative ratios and reliability.Work Pap Health Sci2013;1:1–8.
30.McGuigan MR,Doyle TL,Newton M,Edwards DJ,Nimphius S,Newton RU.Eccentric utilization ratio:effect of sport and phase of training.J Strength Cond Res2006;20:992–5.
31.Ferris DP,Farley CT.Interaction of leg stiffness and surfaces stiffness during human hopping.J Appl Physiol1997;82:15–22.
32.Hebert-Losier K,Eriksson A.Leg stiffness from doubly integrated ground reaction forces depend on the integration constant.American Society of Biomechanics.Omaha,NE,USA.September 4–7,2013.
33.Ditroilo M,Watsford M,De Vito G.Validity and inter-day reliability of a free-oscillation test to measure knee extensor and knee fl xor musculo-articular stiffness.J Electromyogr Kinesiol2011;21:492–8.
34.Rees SS,Murphy AJ,Watsford ML,McLachlan KA,Coutts AJ.Effects of proprioceptive neuromuscular facilitation stretching on stiffness and force-producing characteristics of the ankle in active women.J Strength Cond Res2007;21:572–7.
35.Bruton A,Conway JH,Holgate ST.Reliability:what is it,and how is it measured?Physiotherapy2000;86:94–9.
36.Abdi H.Coefficien of variation.In:Salkind N,editor.Encyclopedia of research design.Thousand Oaks,CA:Sage;2010.
37.Dumholdt E.Physical therapy research:principles and applications. Philadelphia,PA:WB Saunders Co.;1993.
38.Hopkins WG.Spread sheets for analysis of validity and reliability.Sport Sci2001;19:36–42.
39.Pruyn EC,Watsford ML,Murphy AJ,Pine MJ,Spurrs RW,Cameron ML, et al.Seasonal variation of leg stiffness in professional Australian rules footballers.J Strength Cond Res2013;27:1775–9.
40.Aird L,Samuel D,Stokes M.Quadriceps muscle tone,elasticity and stiffness in older males:reliability and symmetry using the MyotonPRO.Arch Gerontol Geriatr2012;55:e31–9.
41.Blackburn JT,Padua DA,Weinhold PS,Guskiewicz KM.Comparison of triceps surae structural stiffness and material modulus across sex.Clin Biomech(Bristol,Avon)2006;21:159–67.
42.Granata KP,Padua DA,Wilson SE.Gender differences in active musculoskeletal stiffness.Part II.Quantificatio of leg stiffness during functional hopping tasks.J Electromyogr Kinesiol2002;12:127–35.
43.Blackburn JT,Riemann BL,Padua DA,Guskiewicz KM.Sex comparison of extensibility,passive,and active stiffness of the knee fl xors.Clin Biomech(Bristol,Avon)2004;19:36–43.
Received 10 September 2014;revised 30 January 2015;accepted 11 June 2015
Available online 8 December 2015
Peer review under responsibility of Shanghai University of Sport.
*Corresponding author.
E-mail address:elizabeth.pruyn@uts.edu.au(E.C.Pruyn).
http://dx.doi.org/10.1016/j.jshs.2015.12.001
2095-2546/©2016 Production and hosting by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
杂志排行

Journal of Sport and Health Science的其它文章
- Biomarker-guided classificatio scheme of neurodegenerative diseases
- Mechanism of neurodegeneration through tau and therapy for Alzheimer’s disease
- Examining the relationship between sport and health among USA women: An analysis of the Behavioral Risk Factor Surveillance System
- The microbiome,microbial-generated proinflammato y neurotoxins, and Alzheimer’s disease
- Longitudinal trajectories of physical activity in women using latent class growth analysis:The WIN Study
- Evidence of a conservative gait strategy in athletes with a history of concussions