颅内皮样囊肿自发性破裂的CT及MRI表现
2015-12-30廖欣,詹玮,童娟等
·临床研究·
颅内皮样囊肿自发性破裂的CT及MRI表现*
**通信作者 E-mail:1066413835@qq.com
网络出版时间:2015-09-11网络出版地址:http://www.cnki.net/kcms/detail/52.5012.R.20150911.2319.060.html
廖欣1, 詹玮2, 童娟1**, 于静1, 蔡立君3, 高勤4
(1.贵州医科大学附院 影像科, 贵州 贵阳550004; 2.贵州医科大学 病理生理学教研室, 贵州 贵阳550004; 3.贵州医科大学附院 神经内科, 贵州 贵阳550004; 4.贵州医科大学附院 病理科, 贵州 贵阳550004)
[摘要]目的: 分析颅内皮样囊肿自发性破裂的CT及MRI表现。方法: 9例经手术和病理证实颅内皮样囊肿自发性破裂的CT、MRI资料,分析其病变部位、大小、形态、与脑积液关系、水肿情况等影像学特点。结果: 皮样囊肿6例位于幕上,3例位于幕下,4例位于鞍上池,2例位于鞍旁,3例位于桥小脑角区;5例囊肿形态规则,4例形态不规则,边界均清楚;8例周围无水肿,1例周围有轻度水肿,9例病灶均破裂,目脂滴进入脑脊液内;CT扫描2例呈均匀低密度,7例呈不均匀混杂密度,3例病灶内可见钙化;MRI扫描呈不均质混杂信号,其内均可见短T1脂肪信号,破裂的脂滴均呈短T1、长T2信号,脂肪抑制序列短T1信号均可被抑制;增强扫描6例病灶无强化,3例病灶壁呈明显环形强化,2例破裂脂滴邻近脑膜强化,1例室管膜强化。结论: CT及MRI能够准确显示原发部位的皮样囊肿和破裂后游离于脑脊液内的脂滴,表现具有特征性。
[关键词]皮样囊肿; 颅内疾病; 体层摄影术,X线计算机; 磁共振成像
[基金项目]*贵州省卫生厅科学技术
[中图分类号]R445.2; R445.3; R742
CT and MRI Manifestations of Spontaneous
Ruptured Intracranial Dermoid Cyst
LIAO Xin1, ZHAN Wei2, TONG Juan1, YU Jing1, CAI Lijun3, GAO Qin4
(1.DepartmentofMedicalImaging,theAffiliatedHospitalofGuizhouMedicalUniversity,Guiyang550004,Guizhou,China;
2.DepartmentofPathologicalPhysiology,GuizhouMedicalUniversity,Guiyang550004,Guizhou,China; 3.Department
ofNeurology,theAffiliatedHospitalofGuizhouMedicalUniversity,Guiyang550004,Guizhou,China; 4.Department
ofPathology,theAffiliatedHospitalofGuizhouMedicalUniversity,Guiyang550004,Guizhou,China)
Abstract[] Objective: To investigate CT and MRI manifestations of the spontaneous ruptured intracranial dermoid cyst. Methods: Nine patients with spontaneous ruptured intracranial dermoid cyst confirmed by surgical histopathology were analyzed retrospectively, to analyze intracranial dermoid cyst's locations, size, shapes, relationship to cerebrospinal fluid, edema. Results: Six dermoid cyst result presented at the supratentorium, 3 located at the infratentorium, 4 located at suprasellar cistern, 2 in parasellar and 3 in cerebellopontine angle. 5 of these cases presented regular shape and 4 irregular shape, all with clear margin. No edema was found around 8 cases, 1 case had mild edema around. The dermoid cyst of 9 cases were ruptured and lipid droplet into the cerebrospinal fluid. CT scan in 2 cases showed low density, 7 cases showed inhomogeneous density. Calcifications were shown in 3 cases. The tumors revealed inhomogeneous intensity on MRI, signal of short T1WI could be found in all 9 cases. Ruptured lipid droplets all presented T1WI and T2WI, and could be suppressed on fat suppressed sequence. After intensified scan, 6 cases showed no enhancement, and ring-shaped intense enhancement showed in 3 cases. Additionally, meningeal or ependymal enhancement were found in 3 cases. Conclusions: The imaging characteristic of the spontaneous ruptured intracranial dermoid cyst were specific. CT and MR could accurately detect the extent of tumor involvement.
[Key words] dermoid cyst; intracranial disease; tomography, X-ray computed; magnetic resonance imaging
中枢神经系统皮样囊肿破裂伴脂滴进入脑脊液临床少见,原发破裂的病变常位于颅内或椎管内[1-3]。CT和MRI容易发现脑脊液内的脂滴,是诊断明确的有效手段。回顾性分析9例经手术和病理证实颅内皮样囊肿自发性破裂的CT及MRI表现,结合相关文献,总结颅内皮样囊肿破裂的影像诊断和鉴别诊断。
1材料与方法
1.1一般资料
收集2003年10月~2015年2月经临床手术和病理证实的颅内皮样囊肿9例,男6例,女3例,年龄21~48岁,中位年龄38岁。临床症状表现为头痛、头昏、恶心、呕吐,部分患者伴癫痫、听力或视力减退、面神经麻痹、偏身感觉和运动障碍,近期症状均突然加重。
1.2扫描技术
采用SIEMENS SOMATOM Sensation 16排螺旋CT和GE公司Signa 1.5 T超导型磁共振扫描仪头部专用线圈进行扫描。9例行CT平扫,扫描参数为120 kV,300 mAs,层厚3 mm,层间距3 mm;MRI检查9例,均行平扫、增强扫描,常规使用轴位T1WI、T2WI、T2/FLAIR、DWI、STIR,T1WI/SE(TR 500 ms,TE 20 ms),T2WI/SE(TR 4 300 ms,TE 100 ms);视野24 cm×24 cm,层厚5 mm,层间距1 mm,矩阵(256~512)×(256~512),增强对比剂为钆喷酸葡胺(Gd-DTPA),注射剂量为0.1 mmol/kg。
2结果
2.1影像概述
9例病灶均位于颅内脑外,4例位于中线,5例位于中线旁;6例位于幕上,其中4例位于鞍上池,2例位于鞍旁,3例位于幕下桥小脑角区。5例形态规则,呈圆形3例,椭圆形2例,4例形态不规则;边界均清楚,最大28 mm×30 mm×31mm,最小12 mm×15 mm×10 mm,8例周围无水肿,1例周围有轻度水肿,9例病灶邻近脑实质均受压,但未见脑积水和病灶内出血表现。9例病灶均破裂,脂滴进入蛛网膜下腔和(或)脑室系统内。
2.2CT及MRI表现
CT扫描见2例病灶呈均匀低密度,7例密度不均,呈高低混杂密度,其内可见团状、条状或点状低密度脂肪影,其中3例病灶内可见条状或点状高密度钙化,破裂的脂滴呈点状、短条状低密度影。MRI扫描9例病灶均呈不均质混杂T1、混杂T2信号,其内均可见短T1脂肪信号,1例周围的轻度水肿呈稍长T2信号,FLAIR像上病灶呈混杂信号,DWI上病灶扩散基本不受限,呈低信号。破裂的脂滴均进入邻近外侧裂池、鞍上池、环池、脚间池、四叠体池、纵裂池及大脑凸面脑沟内,呈斑点状、条带状,表现为短T1、长T2信号,脂肪抑制序列短T1信号均可被抑制。增强扫描6例病灶无强化,3例病灶壁呈明显环形强化,2例破裂脂滴邻近脑膜强化,1例室管膜强化。磁共振血管成像(MRA)显示颅内动脉血管无异常。见图1。
3讨论
中枢神经系统肿瘤样病变破裂伴脂滴进入蛛网膜下腔和脑室系统的有皮样囊肿、表皮样囊肿及畸胎瘤,皮样囊肿破裂最常见,表皮样囊肿破裂最少见[4],如无外伤和手术史,其破裂原因为自发性。皮样囊肿含有外胚层和中胚层结构,内含皮肤的各种成分,如毛发、毛囊、皮脂腺等,囊壁或囊内常见钙化,皮样囊肿仅占颅内肿瘤的0.04%~0.6%[5]。表皮样囊肿起源于外胚层组织,但内含丰富的角蛋白、胆固醇结晶、脂类物质和钙化。畸胎瘤起源于内、中、外三胚层,内含胚胎成分,同时可见牙齿、骨骼、毛发及脂肪等[6]。3种囊性病变一旦破裂,其内的脂类物质物形成脂滴漂浮于脑脊液中,并进入蛛网膜下腔、脑室系统内和脊髓中央管[1-3]。若脂滴进入脑沟、脑池内不再移动,则提示邻近脑膜反应性粘连或蛛网膜下腔腔隙较小。破裂的脂滴可引起无菌性化学性脑膜炎、室管膜炎、中脑导水管狭窄、脑积水等[5,7-8]。颅内皮样囊肿多见于年轻人,男女发病率无明显差异,患者常因头痛、惊厥、恶心、呕吐、癫痫、视力减退、面部麻木、短暂性脑缺血发作等症状就诊[3,5,9-10],部分患者无任何临床症状[8]。中枢神经系统皮样囊肿的治疗分为手术切除和保守治疗,若原发病灶体积较大,占位效应明显,对局部结构出现压迫、侵犯,临床出现明显神经系统受损,应积极采取手术切除[5,11],术中使用大量生理盐水冲洗蛛网膜下腔,临床预后较好;若原发病灶体积较小,临床症状不严重且未出现进展,可采用保守治疗及密切随访。在光镜下见皮样囊肿由角化的鳞状上皮细胞构成,囊壁由外层的纤维组织和内层的皮肤构成,囊内含皮肤附件,如毛发、毛囊、汗腺及皮脂腺产物[9]。
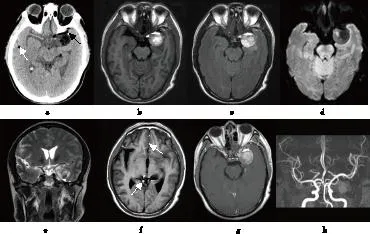
注: a为CT平扫示左侧鞍旁占位,可见点状钙化灶(黑箭头),脑沟内可见破裂的脂滴(白箭头);b为T 1WI示肿块信号 混杂,边界清楚;c为FLAIR像示肿块以高信号为主;d为DWI示肿块弥散不受限;e为T 2WI冠状位示颅内 脑外病灶,脑皮质紧贴肿块;f为T 1WI示脑沟、脑池内多发破裂的脂滴(白箭头);g为T 1WI增强示 肿块边缘环形强化;h为MRA示颅内动脉血管无异常 图1 48岁男性患者左侧鞍旁皮样囊肿破裂的CT和MRI表现 Fig.1 Ruptured dermoid cyst of the left parasellar with lipid droplets in the cerebrospinal fluid
皮样囊肿好发部位为鞍上、鞍旁和大脑纵裂前下部,以中线或中线旁居多,邻近脑实质不同程度受压。CT表现为类圆形、椭圆形及不规则形低密度灶,与脂肪组织密度接近,边界清楚,合并感染时边界模糊,蛛网膜下腔和脑室系统内散在的低密度脂滴能够清晰显示,CT值为-150~0 HU[7],周围无水肿[5]。MRI表现为T1WI混杂稍低信号或等高信号,T2WI为混杂稍高信号,信号不均匀,其内的高信号在脂肪抑制像上消失[3],FLAIR呈混杂信号,DWI上病灶扩散不受限,表现为低信号,增强扫描后病灶无明显强化,部分囊壁可见强化。MRI是目前诊断皮样囊肿的最佳影像学方法,显示微小脂滴优于CT检查[3,5]。破裂的脂滴进入蛛网膜下腔和(或)脑室系统内,表现为脑沟、脑池、脑室内斑点状、条带状、斑片状异常信号,T1WI中脂滴表现为高信号,与低信号脑脊液和等信号脑实质形成鲜明对比,是诊断最为有效的扫描序列。压脂T1WI可帮助进一步确定,T2WI表现为高信号,DWI为低信号,增强扫描不强化,若脂滴引起脑膜或室管膜炎,即可出现脂滴邻近的脑膜或室管膜线性强化。破裂的脂滴进入脑室系统内,聚集较多后可形成脂肪-脑脊液平面[5],是其特征性影像学表现。本组病例中,9例破裂的脂滴均进入蛛网膜下腔,2例进入脑室系统内,呈低密度或短T1、长T2信号,FLAIR像上为高信号,DWI上呈低信号,增强后未见强化,1例侧脑室内可见脂肪-脑脊液平面,2例破裂脂滴邻近脑膜强化,1例室管膜强化,上述表现均与文献报道相符。
虽然颅内皮样囊肿的影像学表现具有一定特点,但仍需与以下疾病相鉴别。表皮样囊肿常发生于桥小脑角区和鞍区,具有见缝就钻的特点,可沿脑池、脑裂塑形生长。囊内若含干酪样物质,CT平扫为低密度,MRI平扫T1WI为低信号,T2WI为高信号,增强T1WI病变不强化或轻微强化。囊内若含较多蛋白、脂质及胆固醇时,CT平扫为稍高密度,MRI T1WI为等或高信号,T2WI呈高低混杂信号,但DWI序列是其非常有价值的诊断、鉴别方法,因其囊内容物粘稠度高,水分子扩散受限,故表皮样囊肿表现为明显高信号,但部分学者认为这种高信号是由于T2穿透效应所致[12]。畸胎瘤发病年龄较小,常发生于松果体区和鞍区,CT扫描呈混杂密度,可见脂肪、软组织和钙化,对钙化显示敏感,T1WI和T2WI均显示信号混杂,增强T1WI病变呈不规则强化。蛛网膜囊肿好发于中颅窝和桥小脑角区,囊内成分单一,为脑脊液,无脂肪及钙化,CT为均匀低密度,MRI信号强度均匀一致,MRI平扫T1WI为低信号,T2WI为高信号,FLAIR和DWI上表现为低信号,增强T1WI病变不强化。
综上所述,颅内皮样囊肿自发性破裂的临床表现不具特征性,但CT及MRI能够准确显示原发部位的皮样囊肿和破裂后游离于脑脊液内的脂滴,表现具有特征性,尤其是MRI显示最为敏感,能够准确显示病灶累及的范围,对诊断及鉴别诊断具有重要价值,可为临床制定治疗策略提供客观依据。一旦确定破裂的原发皮样囊肿后应尽早手术治疗,以防内容物继续溢出。
4参考文献
[1] Kabbasch C, Dorn F, Mpotsaris A, et al. Rupture of a spinal dermoid cyst may lead to dissemination and progress of Fatty tissue in the central spinal canal and intracranial subarachnoid space. A case report[J]. Neuroradiol J, 2014(6):759-763.
[2] Garg K, Kumar R. Isolated central canal rupture of spinal dermoid. Report of 3 cases[J]. J Neurosurg Spine, 2014(3):361-366.
[3] Sharma M, Mally R, Velho V. Ruptured conus medullaris dermoid cyst with fat droplets in the central canal[J]. Asian Spine J, 2013(1):50-54.
[4] 孟令惠,何杰,崔建岭.中枢神经系统肿瘤破裂脂滴进入脑脊液三例分析及文献复习[J].中华神经医学杂志, 2014(6):630-632.
[5] Esquenazi Y, Kerr K, Bhattacharjee MB, et al. Traumatic rupture of an intracranial dermoid cyst: Case report and literature review[J]. Surg Neurol Int, 2013(4):80.
[6] Loumiotis I, Morris JM. Central nervous system epidermoid cyst rupture[J]. Arch Neurol, 2012(1):136-137.
[7] Zimny A, Zińska L, Bladowska J, et al. Intracranial lesions with high signal intensity on T1-weighted MR images-review of pathologies[J]. Pol J Radiol, 2013(4):36-46.
[8] Asil K, Gunduz Y, Ayhan LT, et al. Spontaneous rupture of intracranial dermoid tumor in a patient with vertigo. Computed tomography and magnetic resonance imaging findings[J]. Pol J Radiol, 2013(4):79-82.
[9] Kim KH, Cho JH. Ruptured intracranial dermoid cyst associated with rupture of cerebral aneurysm[J]. J Korean Neurosurg Soc, 2011(5):453-456.
[10]Skovrlj B, Mascitelli JR, Steinberger JM, et al. Progressive visual loss following rupture of an intracranial dermoid cyst[J]. J Clin Neurosci, 2014(1):159-161.
[11]De Maio PN, Mikulis DJ, Kiehl TR, et al. AIRP best cases in radiologic-pathologic correlation: Spinal conus dermoid cyst with lipid dissemination[J]. Radiographics, 2012(4):1215-1221.
[12]文宝红,程敬亮,张勇,等.颅内表皮样囊肿破裂的MRI诊断[J].放射学实践, 2013(1):34-37.
(2015-06-13收稿,2015-08-11修回)
中文编辑: 文箐颍; 英文编辑: 赵毅

