"Three essential elements" of the primary health care system:A comparison between California in the US and Guangdong in China
2015-12-06MinfangHuangDonghaiWeiLouisRubinoLianshenWangDazhuangLiBofengDingGanLi
Minfang Huang, Donghai Wei, Louis Rubino, Lianshen Wang, Dazhuang Li, Bofeng Ding, Gan Li
1. School of Health Management, Guangzhou Medical University, Guangzhou 510182,China
2. California State University,Northridge, Los Angeles 91325,USA
"Three essential elements" of the primary health care system:A comparison between California in the US and Guangdong in China
Minfang Huang1, Donghai Wei1, Louis Rubino2, Lianshen Wang1, Dazhuang Li1, Bofeng Ding1, Gan Li1
1. School of Health Management, Guangzhou Medical University, Guangzhou 510182,China
2. California State University,Northridge, Los Angeles 91325,USA
The primary health care system (PHCS) is the portal and basis for the national health delivery system. There are a number of elements which comprise the PHCS, but the system cannot be established and developed without the support of "three essential elements," including general practitioners (GPs), health insurance, and government health investment. Through comparative analysis of the "three essential elements" of the PHCS between California in the US and Guangdong in China, this article indicates that there are three important aspects in developing a PHCS in China,as follows: training qualified GPs; establishing a diversified health insurance system to strengthen the policy connections between health insurance and the PHCS thereby increasing government health investment; and broadening health financing channels.
Primary health care system (PHCS); general practitioner (GP); health insurance;government health investment; California; Guangdong
Introduction
The primary health care system (PHCS) is the portal and basis for a national health delivery system. A PHCS has a significant role in improving national health, avoiding the excessive increase in national health investment, and providing health welfare. General practitioners (GPs), health insurance, and government health investment are the "three essential elements" of a PHCS among all its components. Through a preliminary exploration of PHCS in China and the US, it has been shown that there is a similarity (e.g., welfare)and comparability between the systems of the two countries [1]. As a top economy around the world, the PHCS in the US is more mature and well-developed, thus China could draw lessons from the US experience. Based on the actual conditions of China, we compared and analyzed the "three essential elements" of the PHCS between California in the US and Guangdong in China to give some suggestions on the development of the PHCS in China.
Comparison of the "three essential elements" of PHCS between California and Guangdong
A brief introduction to California and Guangdong
The economic development, geographic location, population, and health conditions of California and Guangdong are similar(Table 1) [2–8]. With respect to economic development, both California and Guangdong are developed areas in their own countries. California, the third largest state inthe US and located in the southwest US, occupies 4.41% of the land area of the country, while Guangdong is located in south China and covers 1.87% of the land area of the country.California and Guangdong account for 11.97% and 7.76% of the US and China populations, respectively, both California and Guangdong are the most populous areas of US and China,respectively. With respect to health conditions, both of the areas have good developing states. The birth rate and life expectancy in California are above average for the US, while the death rate is below the average. The birth and death rates in Guangdong are below average for China, while life expectancy is above average. Thus, California and Guangdong could be representatives for the US and China and are comparable with respect to the PHCS.
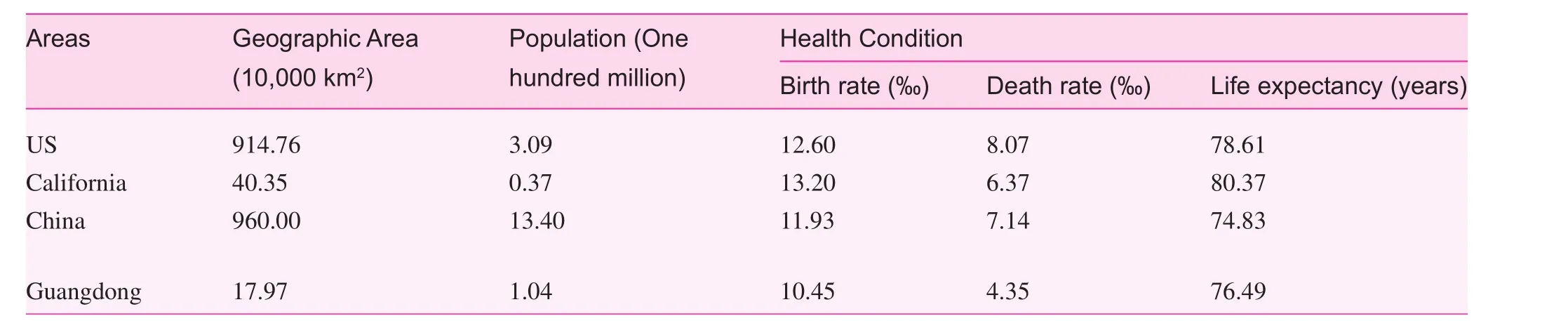
Table 1. Basic information for California and Guangdong
General practitioner
GPs are the best providers of high-quality primary health care services, as well as the best gatekeepers of health care systems [9]. As shown in Table 2, there are approximately 30,000 GPs in California [10]. The number of GPs per 10,000 population in California is 4.73, which is greater than the number of GPs per 10,000 population in the US (4.61) [11].There are 7940 GPs in Guangdong; the number of GPs per 10,000 population in Guangdong is 0.75, which is less than the number of GPs per 10,000 population in China (0.81)[8]. California has adopted the "4+4+3" training path; thus a GP receives at least 11 years of standardized training, after which the physician is considered to be qualified for practicing medicine [12]. GPs in Guangdong undergo a "5+3" training path [1]. The average annual income of GPs in California is $180,000 [13]. GPs in California are approved to practice medicine at various health agencies with autonomy, high self-esteem, and good career prospects. GPs in Guangdong practice medicine in their affiliated institutions, most of whom are in grass-roots medical agencies with low salaries and hopeless promotion prospects due to the less developed practice system [14]. An investigation has shown that [15]GPs have the lowest salaries ($8034) among all the medical practitioners ($10,765) in China; Guangdong province is no exception.
Health insurance
Health insurance in California is highly marketable and diversified; private health insurance is adopted first, followed by public health insurance (Table 3) [16]. In California, 78.80%of the population was covered by health insurance between 2010 and 2012; there were approximately 7 million uninsured people in California at that time [17]. Currently, the health insurance marketplace in California (Covered California) has been established on the basis of the new health care reform implemented by President Obama to help insurers compete in cost-efficient ways, and expand insurance coverage for more people. The health insurance system in Guangdong adopts basic health insurance first, supplementary health insurance second, and urban-rural medical assistance last [16]. This is a single-formed system which receives strong support from the government, and has the opportunity to receive financial subsidies. In Guangdong, 97.52% of the population (84,218,100)had health insurance in 2012 [18].
The PHCSs in California and Guangdong leverage the health insurance platforms to take active roles as gatekeepers in community first-contact diagnosis; however, the operatingmechanisms are different [19]. In California [20], insured people are not forced to see a GP, but under the economic constraints implemented by health insurance institutions, it is favorable for people to accept community first-contact diagnosis, which is made by GPs. If the health insurance subscribers want to be reimbursed for their medical costs, they should follow the regulatory procedure to see the physician, i.e., GPs for the first-contact diagnosis and specialists in hospitals for referred treatment. In contrast, specialists in hospitals are only allowed to treat insured patients who have a referral letter written by a GP, or they will not receive full remuneration.In Guangdong [21], health insurance providers encourage the insured to go to primary health care institutions and see physicians by raising the reimbursement in these institutions; now,the insured can choose one primary health care institution and one hospital as their regular medical agencies.
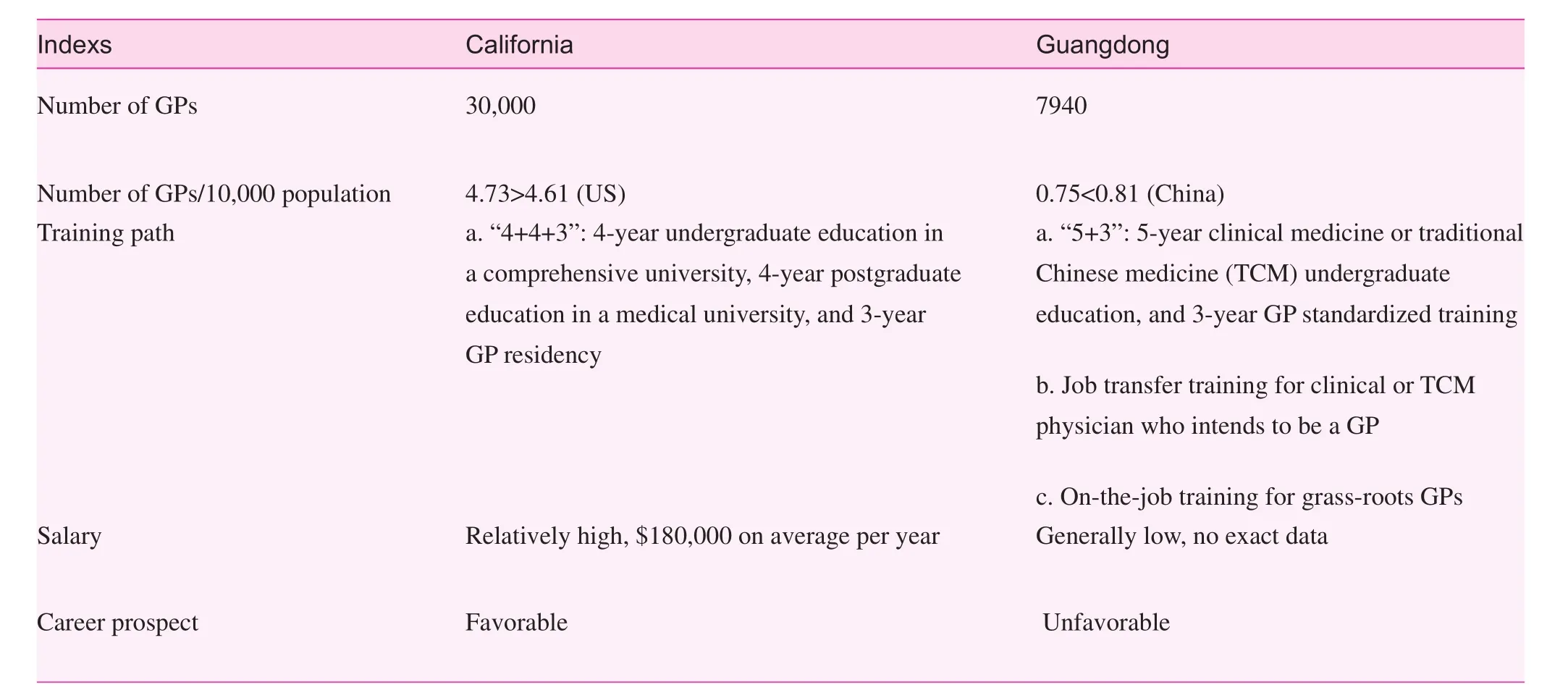
Table 2. Comparison of general practitioner teams in California and Guangdong
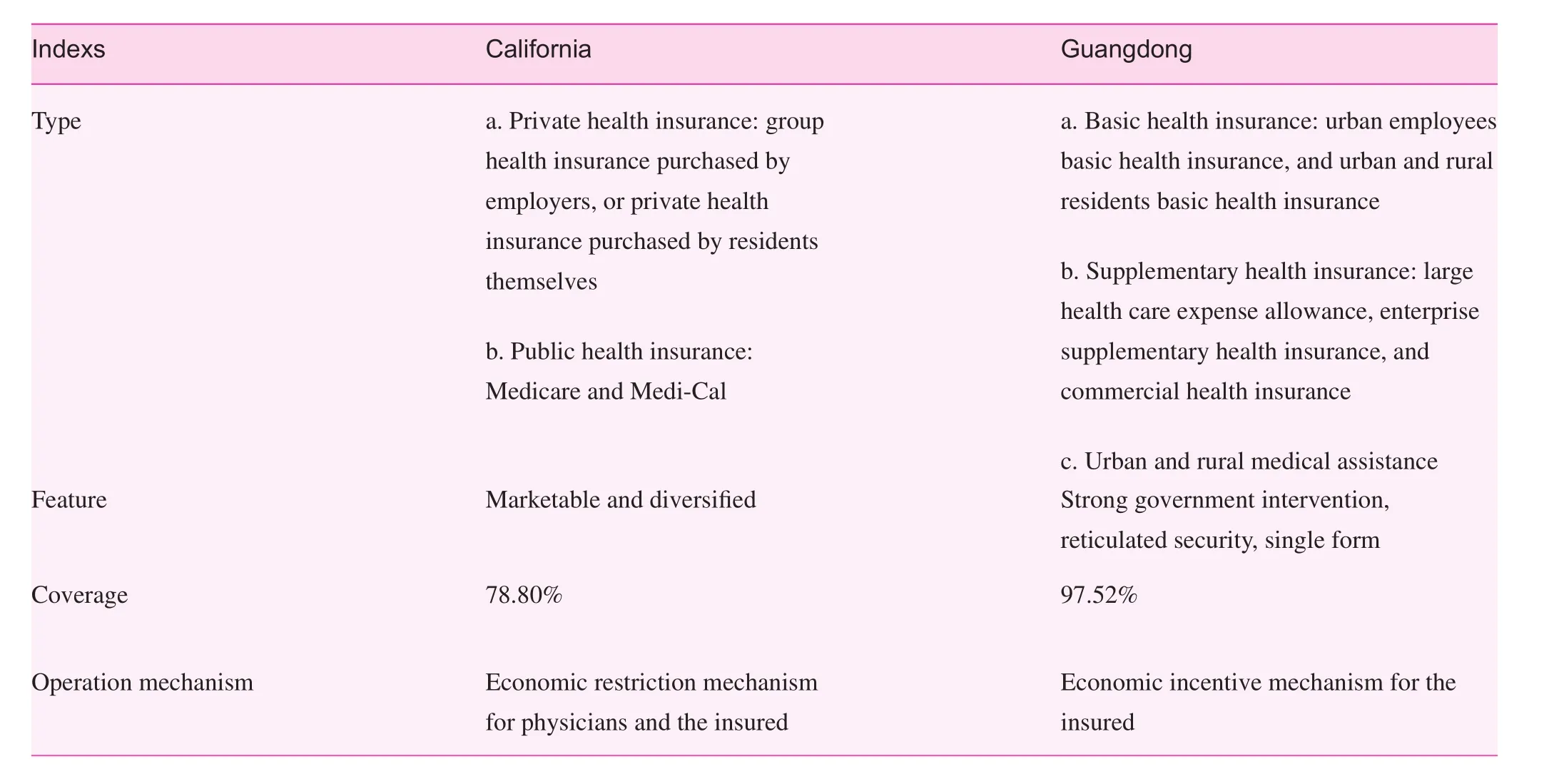
Table 3. Comparison of health insurance systems in California and Guangdong

Table 4. Financial subsidies for primary health care institutions and hospitals in Guangdong (2009–2012)
Government health investment
The World Health Organization (WHO) reported that 17.9%and 5.4% of the GDP, as well as 19.9% and 12.5% of total government health care expenditures had been spent on health care services in the US and China in 2012, respectively [22].On the basis of equity and welfare, a substantial amount of money has been invested in health care services from the US federal government, as well as local and federal authorities every year to help the disadvantaged access primary health care services. In 2011, the financial budget of the Health Resources and Services Administration (HRSA) indicated that the investment of primary health care services was 0.382 billion dollars in California, which accounted for 46.14% of the total investment, and 0.828 billion dollars of all health care services [23]. Between 2012 and 2013, the investment of health care services was $45,493,600, which accounted for 31.9% of total expenditures for the California government[24]. There were 25 million dollars invested in chronic disease prevention and health education programs in California from the financial budget of the US Centers for Disease Control and Prevention (CDC) in 2013 [25].
The income sources of primary health care institutions in Guangdong include government investment (financial subsidies), health care service income, higher authority grants, and others. Government investment (35.78%) and health care service income (61.34%) are the major two sources [26]. The government investment for primary health care institutions is very important because the income of primary health care services is low. The financial subsidies for primary health care institutions in Guangdong showed a rising trend in recent years,which accounted for 22.96%, 23.90%, 17.23%, and 21.52% of the total health financial subsidies from 2009 to 2012, respectively, with a fluctuating proportion. During the same period,the financial subsidies for hospitals were rising continuously,which were about twice the amount of primary health care subsidies each year, and the proportion was always >40% of total health financial subsidies (Table 4) [26, 27–29]. In China,the financial appropriation is allocated by the central, provincial, county/municipal, and district governments hierarchically, and primary health care subsidies are mainly allocated by county/municipal and district governments.
Discussion and analysis
The number of GPs in Guangdong is inadequate, and the training path needs to be standardized.
Currently there is a shortage of GPs in California due to a dramatic increase in the insured under Obamacare. California,however, follows a uniform and strict GP education model,which supports a quality-oriented and standardized source of training of GPs, thereby meeting the demand of primary health care services for the residents. GPs in California are well-paid and they have good career prospects developments with high social recognition. The number of GPs in Guangdong is inadequate, and is far from the target number of 15,000 [30], and the intended allocation of 2–3 GPs per 10,000 population [31].It is disturbing to see that the job loss of GPs is increasing;this phenomenon is mainly due to two reasons: 1. the skills of GPs are not standardized, even after on-the-job or job-transfer training, so the residents do not completely trust GPs, and the needs of residents cannot be met properly [32], and 2. the promotion opportunities and payments for GPs are limited.
Single-type health insurance and powerless health policy in Guangdong
Both Guangdong and California are aiming to broaden the coverage of health insurance. The health insurance system in California is diversified, while it is hard for the single-type health insurance in Guangdong to meet the residents' needs for health security. Primary health care services have been added to medical service procedures under economic constraints and market mechanisms in California since the mutual coordination between physician, health insurance institution, and patient has been developed; the first-contact diagnosis by GPs is more acceptable to the patient. In Guangdong, to encourage residents to see a physician in primary health care institutions,raising health care reimbursements between different levels of health institutions is simply not enough [33]. Compared with California, the strength of economic constraints on medical service providers (especially second or third-class hospitals)in Guangdong needs to be improved because it is not working optimally.
Health investments by the Guangdong government are inadequate, and fund shortages are the bottleneck of primary health care development
The above mentioned data show that the US government has put massive funds into the PHCS. Despite some inefficient use of funds, this definitely reflects the high level of attention that government has paid to the PHCS. In China, the government investment in the PHCS is inadequate, the key investment object is the hospital and primary health care institutions receive lower subsidies. The investment is allocated from the top, level-by-level, which may cause a phenomenon referred to as "dividing investment between the central and local financial governments," and lead to less subsidy limits for the primary health care institution. On the whole, fund shortages are the bottleneck of primary health care development.
Policy proposal
Implementing "5+3" training path to cultivate qualified GPs
Qualified GPs are the key fulcrum of the PHCS operation.Some GP training has been shown to be ineffective in China with unskilled trainees and the separation between theoretical studies and practice [34]. Guangdong can draw experience from California to cancel in-service and job-transfer training, and shift the focus to a "5+3" training path. In addition, the policy "quadruple certificate" in Shanghai Province could also be the reference for GP training in Guangdong,i.e., when a Masters' student graduates, he/she will receive four certificates (graduation diploma, Masters' degree,practicing physician qualification, and standard residency training) [35]. This could enhance the title promotion and wages of GPs. In addition, the authors of this article suggest improving the salaries, social reputation, and title promotion of GPs further to give them good career prospects and to avoid talent drainage.
Establish a diversified medical security system, and strengthen the connection of policies on health insurance and PHCS
China could learn from the US to build a diversified health insurance system, so as to meet the multi-level medical security needs of residents. Building a diversified medical security system includes introducing social capital to develop commercial health insurance, increase the type of health insurance,grant designated qualifications, encourage private individuals and enterprises to purchase commercial health insurance,set up national or provincial welfare health insurance, assure care for the indigent, build mutual funds with social fund help,and broaden the channels of medical assistance. China should strengthen the policy connections between health insurance and PHCS, i.e., reform the mode of health insurance payments, confirm reimbursement rates, enhance the guidance for insured people on seeking health services, restrict force of health service provider's behavior, and introduce the market mechanism properly to develop a coordinated internal environment between physicians, insurance, and patient to ensure the stability of the PHCS.
Enhance the intensity of government health investment and broaden the funding channel of health care services
Adequate financial support is an essential factor for the sustainable development of the PHCS. The authors of this article suggest that the Chinese government increase the investments in PHCSs to give priority to the development of primary health care institutions, and confirm the share of the financial obligation between all levels of government to ensure the government subsidies are being allocated to primary health care institutions timely and sufficiently. The compensation mechanism of primary health care institutions in China should be improved, and the financing channel needs to be broadened by introducing private capital, charitable funds, and others to support the development of PHCSs.
In summary, during the constant exploration and development of the PHCS in China, training qualified medical practitioners, establishing an effective medical insurance system,and ensuring adequate health care funding for the primary care system are critically needed under our national health care reform. Certainly, there are many influencing factors for improving the primary care system beyond the above-mentioned "three essential elements." For example, the cooperation between public hospitals and primary care institutions and how they work with each other are also important areas for improving the primary care system and need further research.
Acknowledgements
The authors would like to thank all the professionals who participated in this study.
Conflict of interest
The authors declare no conflict of interest.
Funding
This article is funded by China Medical Board (CMB) [11-076].
1. Xu GP. A perspective on the development of family medicine in China. Fam Med Community Health 2014;2:28–34.
2. United States Census Bureau [www.census.gov/en.html]. State and County Quick Facts. Available from: http://quickfacts.census.gov/qfd/states/06000.html.
3. People's Government of Guangdong [www.gd.gov.cn/].Geographic position, scope and area. [2014-10-03]. Available from: www.gd.gov.cn/gdgk/sqgm/zrdl/201501/t20150121_208133.htm.
4. National Bureau of Statistics of the People's Republic of China.Communiqué of the National Bureau of Statistics Of the People's Republic of China on Major Figures of the 2010 Population Census (No.2). 2010.
5. Martin JA, Hamilton BE, Osterman MJK, Curtin SC, Mathews TJ. Births: Final data for 2012. Natl Vital Stat Rep 2013;62:66.
6. National Vital Statistics Report: "Deaths: Final Data for 2011".Available from: www.cdc.gov/nchs/data/nvsr/nvsr62/nvsr62_09.pdf.
7. California Life Expectancy live longer live better: California Life Expectancy. [2014-7-30]. Available from: www.worldlifeexpectancy.com/usa/california-life-expectancy.
8. Statistical Information Center of National Health and Family Planning Commission of the People's Republic of China. China Health Statistical Yearbook 2013. 2013.
9. Xian FH, Lu XQ, Lv ZF. Chinese general practitioner training scheme: challenges and strategies. Chin Gen Pract 2012;22:2498–501.
10. Judy L. Facing doctor shortage, California lawmaker seeks to boost services. US: Associated Press, 2013. Available from:www.thereporter.com/ci_23521832/facing- doctor-shortagecalifornia-lawmaker-seeks-boost-services.
11. Esther H, Chun JH. State variability in supply of office-based primary care providers: United State 2012. NCHS Data Brief 2014;1–8. Available from: www.cdc.gov/nchs/data/databriefs/db151.pdf.
12. American Academy of Family Physicians: Medical School& Residency. Available from: www.aafp.org/medical-schoolresidency.html.
13. Medscape: Physician Compensation Report 2013. Available from: www.medscape.com/features/slideshow/compensation/2013/familymedicine.
14. Xu GP. Great efforts are needed to develop primary medical service in China: correcting the mistranslation of "Primary Health Care" as the first step. Fam Med Community Health 2014;2:6–9.
15. Wan M. Survey of doctor's payment in medical website: the average yearly income of doctors in Guangdong is 80 thousands.Southern Urban Daily. Available from: www.cq.xinhuanet.com/2013-12/04/c_118410466.htm.
16. Lu ZX. Social medical insurance science. 3rd ed. Beijing:People's Medical Publishing House; 2007;7:38–45.
17. Paul Fronstin. California Health Care Almanac: California's Uninsured By the Numbers. Available from: www.chcf.org/~/media/MEDIA%20LIBRARY%20Files/PDF/C/PDF%20CaliforniaUninsured2013.pdf.
18. Statistical Bureau of Guangdong. Guangdong Statistical Yearbook 2013. 2013.
19. O'Donnell RR. New models for chronic disease management in the United States and China. Fam Med Community Health 2014;2:13–9.
20. California Department of Insurance: Compare PPOs. EPOs,and HMOs. Available from: www.insurance.ca.gov/01-consumers/110-health/10-basics/compare.cfm.
21. China Social Insurance: Health Insurance. Available from: www.gdsi.gov.cn/zcfg_elbx/.
22. World Health Organization. Global Health Observatory (GHO)data. Available from: www.who.int/gho/countries/en/.
23. Health Facts Trust for America's Health. Investing In America's Health: A State-by-State Look at Public Health Funding and Key. 2013.
24. California's Governor's Budget 2012–2013 Enacted Budget Detail: Health and Human Services. Available from: www.ebudget.ca.gov/2012-13-EN/Enacted/StateAgencyBudgets/4000/agency.html.
25. Centers for Disease Control and Prevention. Fiscal Year 2013 Grants Summary Profile Report for California. Available from:wwwn.cdc.gov/FundingProfiles/ FundingProfilesRIA/Report_Docs/PDFDocs/Rpt2013/California-2013-CDC-Grants-Profile-Report.pdf.
26. Health Department of Guangdong. Guangdong Health Statistics Yearbook 2012. 2012.
27. Health Department of Guangdong. Guangdong Health Statistics Yearbook 2009. 2009.
28. Health Department of Guangdong. Guangdong Health Statistics Yearbook 2010. 2010.
29. Health Department of Guangdong. Guangdong Health Statistics Yearbook 2011. 2011.
30. People's Government of Guangdong. The notification of the implementation scheme of basic drug system and new basic operating mechanism in Guangdong. 2013.
31. People's Government of Guangdong. The suggestion of establishing general practice system in Guangdong. 2012.
32. Qin JM, Zhang YC, Zhang LF, Liu LQ, Zhou W, Liu CL, et al.Comprehensive reform of community health service in east, middle and west regions of China: from patients' perspective. Fam Med Community Health 2013;1:15–9.
33. Qingdao Daily: Hierarchical diagnosis and treatment can not only depend on the price leverage. [2015-03-10]. Available from: http://news.163.com/14/1027/13/A9ILLA3H00014AED.html.
34. Ji T. Thought and consideration of Chinese general practitioner training model. Chin J Med Educ 2013;33:185–7.
35. Zhang A, Xia W, Bao Y. Efficiency of community health service in urban and suburban areas of Shanghai: based on production function. Fam Med Community Health 2013;1:5–8.
Donghai Wei School of Health Management,Guangzhou Medical University,Guangzhou 510182, China
E-mail: weidhai@vip.163.com
12 January 2015;
Accepted 15 February 2015
杂志排行
Family Medicine and Community Health的其它文章
- Effectiveness of an employment-based smoking cessation assistance program in China
- Team-based stepped care in integrated delivery settings
- The Accountable Care Organization results: Population health management and quality improvement programs associated with increased quality of care and decreased utilization and cost of care
- Menopause and the risk of metabolic syndrome among middle-aged Chinese women
- Availability and social determinants of community health management service for patients with chronic diseases:An empirical analysis on elderly hypertensive and diabetic patients in an eastern metropolis of China
- Evaluating the process of mental health and primary care integration:The Vermont Integration Profile