Availability and social determinants of community health management service for patients with chronic diseases:An empirical analysis on elderly hypertensive and diabetic patients in an eastern metropolis of China
2015-12-06ZhijunWuWeiyanJian
Zhijun Wu, Weiyan Jian
Availability and social determinants of community health management service for patients with chronic diseases:An empirical analysis on elderly hypertensive and diabetic patients in an eastern metropolis of China
Zhijun Wu, Weiyan Jian
Objective:This study aimed to determine the availability of community health management services and the relevant social determinants for elderly patients with chronic diseases.Methods:All data were obtained from the 2013 random sampling household survey on an elderly population conducted by the School of Public Health of Peking University in an eastern metropolis in China. Information from the database of the above survey involving 1495 hypertensive or diabetic patients >60 years of age, as representatives of the city, were included. The study described the availability of follow-up services by community doctors among elderly hypertensive and diabetic patients during the 12 months before the survey. An ordinal multinomial logistic regression model was used to conduct the analysis on the influence of socio-economic background upon such availability.Results:Eighty-one percent of hypertensive patients and 84.7% of diabetic patients had not
any follow-up service from community doctors within 12 months prior to the survey.Among elderly hypertensive patients, those registered as non-agricultural household members,those with high and above-average income, as well as management personnel of government agencies, enterprises, and social programs have a greater chance of accepting follow-up service by community doctors because of their relatively higher socio-economic rankings. Among elderly diabetic patients, such socio-economic factors had no significant influence on the availability of the follow-up service for chronic diseases.Conclusion:The coverage of community health management services for elderly hypertensive and diabetic patients needs improvement. More effort should focus on promoting the availability of community health management services for elderly hypertensive patients, especially those with lower socio-economic status.
Community health management; hypertension; diabetes; socio-economic status;elderly population
Introduction
Data and methods
Data source
Information on a hypertensive and diabetic population>60 years of age with hospital diagnoses was obtained from the database of the 2013 "Influenza Vaccination and Health Status Survey on Aged Population of an Eastern Metropolis" conducted by the School of Public Health of Peking University. We received consent to use the database from the original survey.Eight hundred and seventy-three patients with hypertension,372 patients with diabetes, and 250 patients with hypertension and diabetes were included. Probability-Proportional-to-Size Sampling (PPS) was implemented to carry out the survey that covered 8 local counties, 64 urban and rural communities,and a total of 1717 residents >60 years of age. The subjects of the survey were representative of the city population. The variables of the study consisted of basic social demographics,hypertension, and diabetes prevalence, as well as information on community health services for chronic diseases.
Methods
Household type, household per capita income, educational level, and type of profession were used to describe the objective socio-economic status in the study. Subjects were divided into 5 groups based on income, which in ascending order were:lowest (20%), lower (20%), middle (20%), higher (20%), and highest (20%). Times of visits to hypertensive and diabetic patients during the past 12 months before the survey were considered the index for chronic disease management services in communities, and divided into four grades (no visit, 1–2 visit/visits, 3–4 visits, and >4 visits).
To investigate the coherence between social determinants and the follow-up services for patients with chronic diseases, the ordinal multinomial logistic regression model was adopted to calculate the age- and gender-matched odds ratio (OR). Dependent variables for indices of objective social status included four grades (no follow-up visit by community doctors, 1–2 visit/visits, 3–4 visits, and >4 visits among patients with hypertension and diabetes). If the OR was >1,then the index represented a contributing factor; if not, an impeding factor. Indices of objective socio-economic status consisted of household type (0 for rural household and 1 for non-rural), household per capita income (4 dummy variables by the contrast of the lowest 20% in an ascending order [lower 20%, middle 20%, higher 20%, and the highest 20%]; 1 for yes and 0 for no), educational level (4 dummy variables using"never been to school" in contrast to primary school, junior high school, senior high, vocational or technical secondary school, junior college and above; 1 for yes and 0 for no), type of profession (7 dummy variables in contrast with management of government agencies, enterprises, and social programs [professionals and technical, clerical, commercial and service, personnel engaged in agricultural, forestry, livestock husbandry, fishery and water resources-related production,production and transportation equipment operators, unemployed, and others]; 1 for yes and 0 for no). The statistical analysis was performed using SPSS 19.0.
Results
Basic information
胶东半岛位于华北平原东北部沿海地区,山东省东部丘陵区。该区主要为暖温带湿润季风气候,全年湿度变化幅度大,四季分明,雨热同期。地势大致为中间高四周低,半岛最高海拔位于南部崂山,主峰海拔1 133 m,地貌类型主要为山前平原、海滩、缓丘。河流由中部向南向北流动,源短流急,年流量涨落起伏大。土地总面积约为3万km2,占山东省土地总面积的19%。耕地面积为1.16万km2,以旱地为主,约占全省耕地总面积的15%,多用来种植花生、玉米等作物。行政区主要包括烟台、青岛、威海3市,共计33个县及县级市、区,见图1。
Please refer to Table 1 for subjects' basic information. Six hundred and twenty-three patients with hypertension with no co- morbidities were included. Subjects 60–69 years of age accounted for the majority (50.1%) of the patients. There were more women (60.5%) than men (39.5%). The patients were mainly from non-agricultural households (81.7%) with educational levels lower than primary or junior high school (62.9%).
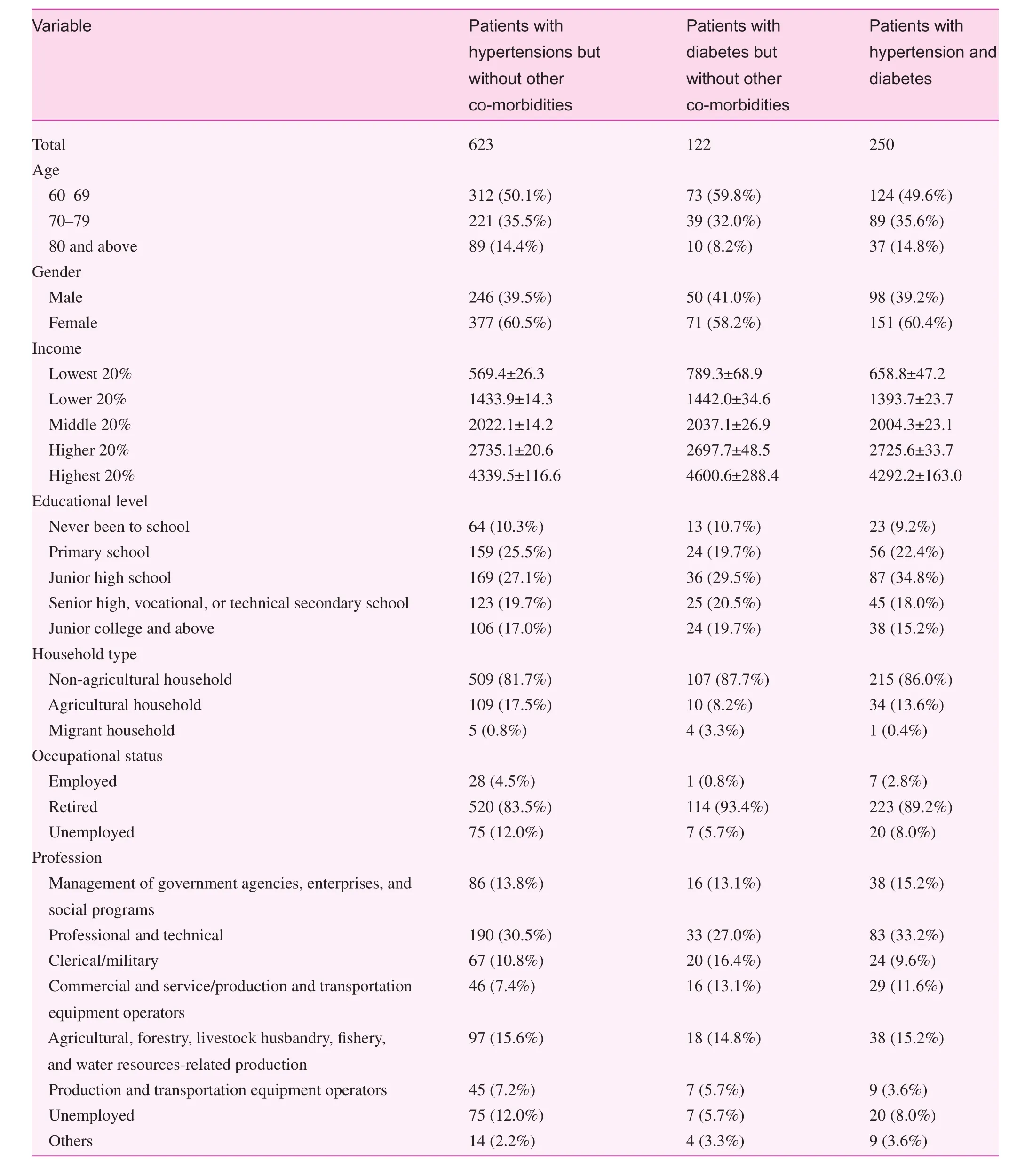
Table 1. Basic information
Occupational analysis indicated that 4.5% of the patients were employed and 83.5% were retired. Employees and exemployees were mostly professionals and technicians (30.5%).Monthly household per capita incomes of the lowest and highest 20% groups were 569.4 yuan and 4339.5 yuan respectively.
One hundred and twenty-two patients with diabetes without co-morbidities were included. Subjects 60–69 years of age accounted for the majority (59.8%) of the patients. There were also more women (58.2%) than men (41.0%). Patients were mainly non-agricultural household members (87.7%) with educational levels lower than primary or junior high school (59.9%).Of the patients with diabetes, 0.8% were employees and 93.4%were retired. Occupational status revealed that 27.0% of employees and ex-employees were professionals and technicians. The monthly household per capita incomes of the lowest and highest 20% groups were 789.3 yuan and 600.6 yuan, respectively.
Two hundred and fifty patients with hypertension and diabetes were included at the same time. Patients 60–69 years of age constituted the majority (49.6%). There were more women(60.4%) than men (39.2%). The patients were mostly from nonagricultural households (86.0%) with educational levels lower than primary or junior high school (66.4%). Occupational status showed that 2.8% of the patients were employees and 89.2% were retired. Most of the employees and ex-employees were professionals and technicians (32.2%). The monthly household per capita incomes of the lowest and highest 20%groups were 658.8 yuan and 4292.2 yuan, respectively.
Community health management services for patients with hypertension and diabetes
As shown in Table 2, on average, weekly blood pressure (BP)measurements were obtained among 41.6% of the patients with hypertension; 39.7% had their BPs measured monthly, 14.8%failed to have the BPs measured, and 1.5% did not have BPs measured in the past year. Of the patients with hypertension,81.5% received no follow-up service by community doctors,8.1% received 1–2 visit/visits, 2.6% received 3–4 visits, and 7.6% received >4 visits. Follow-up services for patients with hypertension were mainly carried out in the outpatient department (63.8%) and over the telephone (23.9%).
On average, blood glucose levels were measured every week among 17.7% of all patients with diabetes, 44.4% hadglucose determinations monthly, 32.8% did not have blood glucose determinations, and 1.9% did not have blood glucose determinations in the past year. Of the patients with diabetes,87.5% received no follow-up services by community doctors,3.5% received 1–2 visit/visits, 2.7% received 3–4 visits, and 6.1% received >4 visits. Follow-up services for patients with diabetes were mainly carried out in the outpatient department(53.3%) and over the telephone (33.3%).
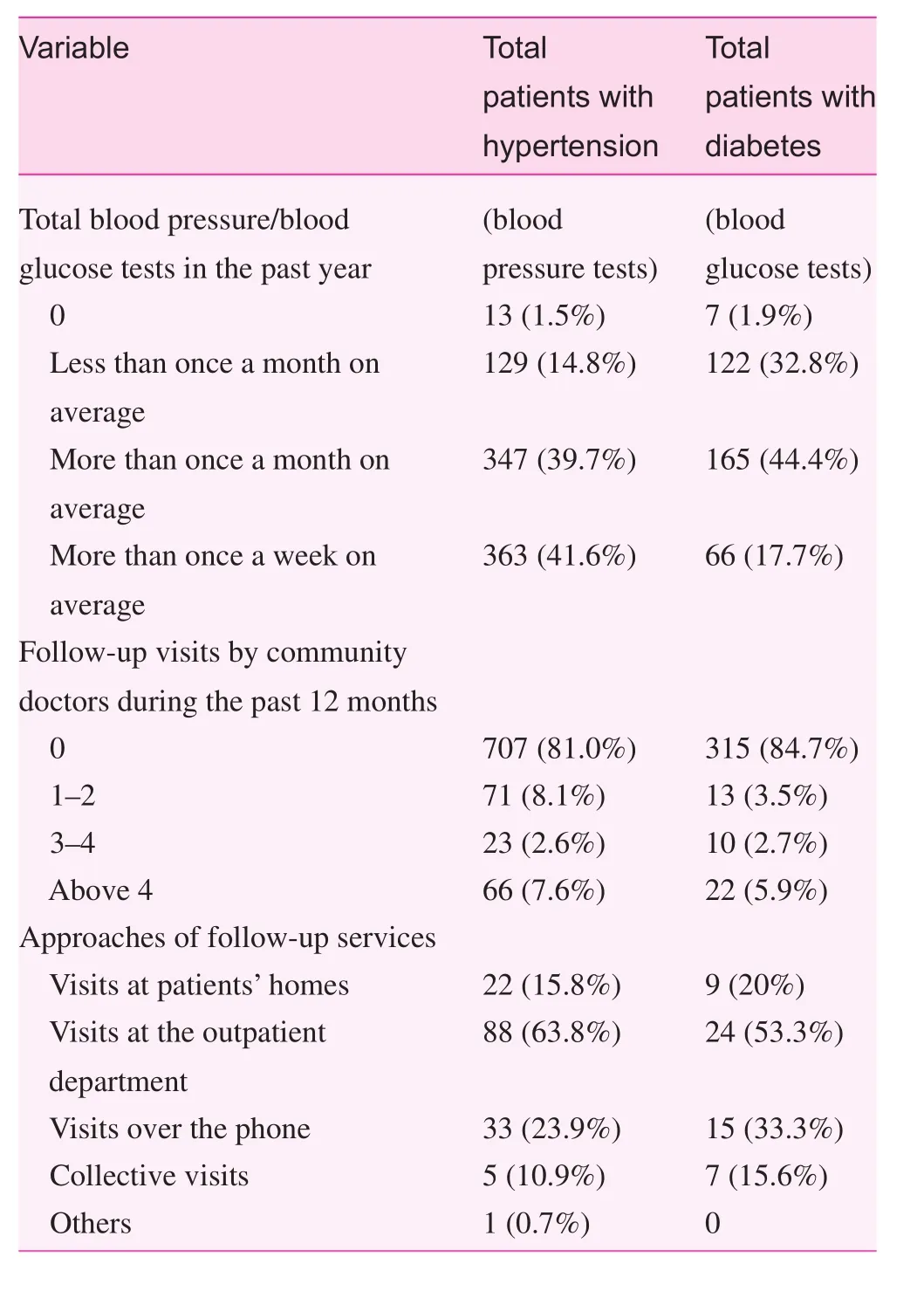
Table 2. Community health management services
Social determinants of the availability of community health management services for patients with hypertension and diabetes
Tables 3 and 4 show the results of the ordinal multinomial logistic regression analysis. Age- and gender-matchedpatients with hypertension without co-morbidities from nonagricultural households received more follow-up visits than those from agricultural households (OR=2.609,p<0.01). In comparison to the 20% group with the lowest income, the higher 20% and highest 20% groups received more follow-up visits. When compared with those working in management of government agencies, enterprises, and social programs(the group of higher-ranked employees), people engaged in agricultural, forestry, livestock husbandry, fishery, and water resources-related production received fewer follow-up visits.No significant difference existed between educational level and the number of follow-up visits. For patients with diabetes with no co-morbidities, the influence of household type,income, education, and vocation on the availability to followup services were insignificant.
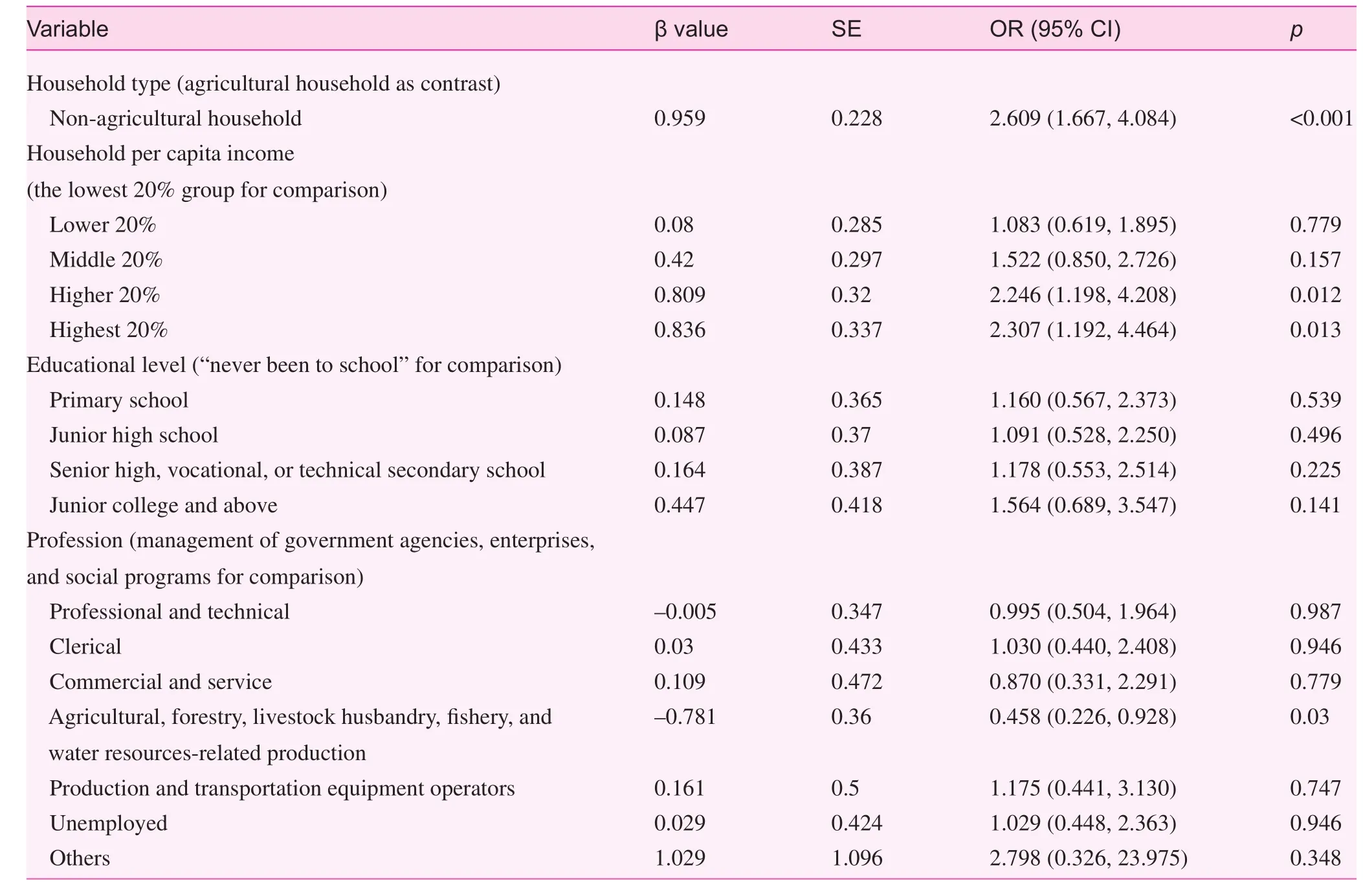
Table 3. Age- and gender-matched relationship between socio-economic status and follow-up visits among elderly hypertensive population
Discussion
Insufficient coverage of health management services for community chronic diseases
Effective control cannot be achieved with insufficient coverage of chronic disease management. With most chronic disease patients out of the health management service, true efficiency can never be achieved regardless of how effective the prevention and control measures are. As indicated by this study,<20% of the elderly patients with hypertension and diabetes living in the city received follow-up services by community doctors during the past 12 months before the survey. Scholars suggest that those with BPs under control should receive community follow-up services at least once every 6 months,and even once a month for those in whom BPs are not wellcontrolled [9]. The study revealed that only 10.2% of elderlyhypertensive patients had received follow-up services at least twice a year. Some scholars also advise that the frequency of community follow-up services should be thrice a year (every March, June, and December) for patients with type 2 diabetes[10]. As shown in this study, however, only 8.6% of elderly patients with diabetes living in the city had received follow-up services at least thrice a year.
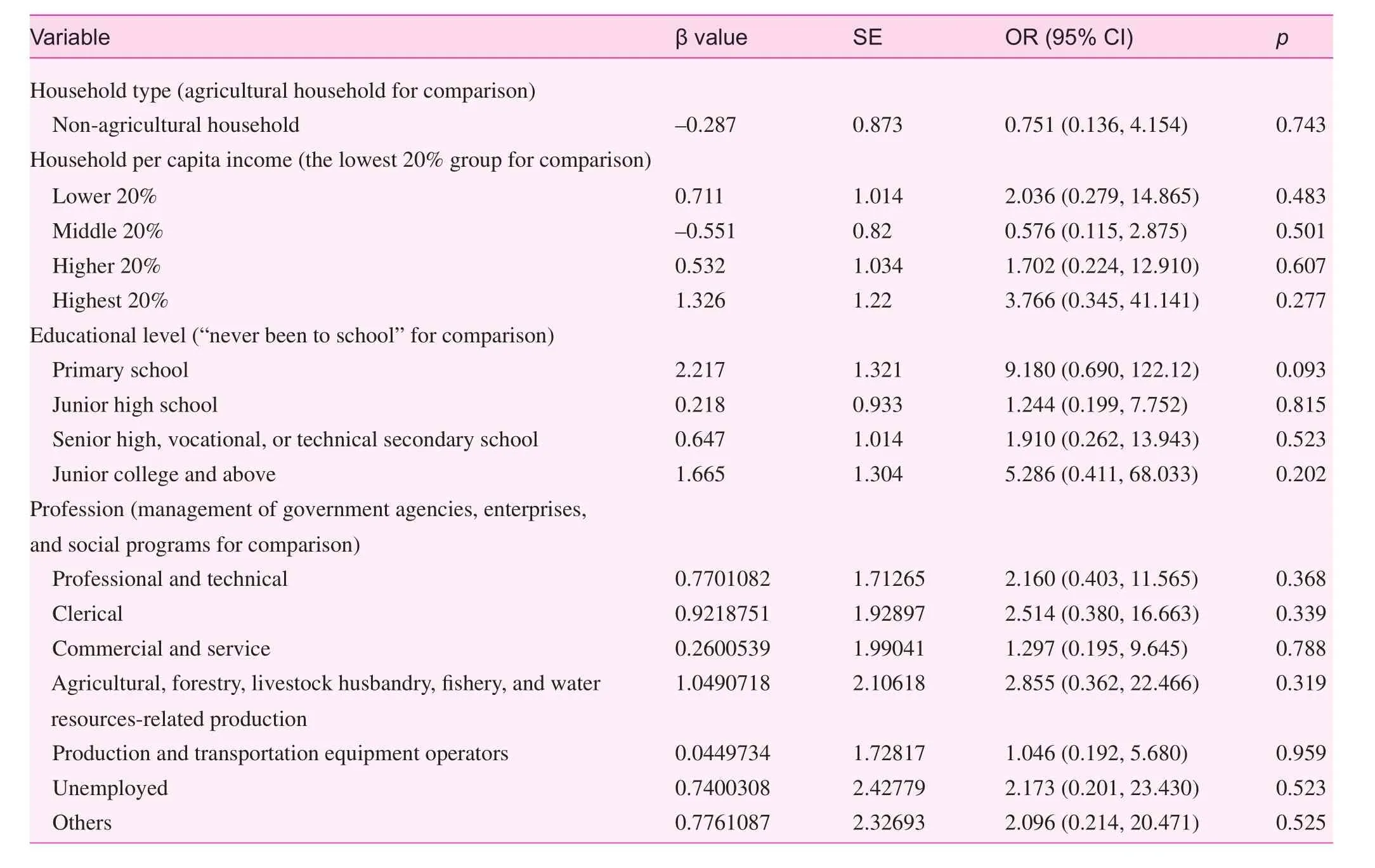
Table 4. Age- and gender-matched relationship between socio-economic status and follow-up visits among elderly diabetic population
Another weak link of the chronic disease management in the city is the "service approach." Chronic disease management is different from medical services. The latter clearly depends on the "initiative of the demand side." Instead, chronic disease management is needed before the demand side has encountered any trouble, thus community health service providers must take the initiative for the demand side. According to the results of this study, approximately 20% of patients with hypertension and diabetes received chronic disease follow-up services at home, while most patients received such services in the outpatient department. The sufficiency and quality of the service cannot be guaranteed when the provider and demand sides both lack initiative.
Different socio-economic rankings and different chronic disease management services among the elderly population
The study observed less availability of those diagnosed with chronic diseases for follow-up services among patients from agricultural households, lower income, and engaged in agricultural, forestry, livestock husbandry, fishery, and water resources-related production. Thus, the availability for chronic disease management services varies as per different socio-economic rankings. Such availability of those at lower socio-economic levels is also lower.
There are two reasons that possibly account for this result. First, those with higher socio-economic rankings enjoy better community environment and facilities, thus the quality of health care service is better as well. As a consequence, they are apt to acquire correct health information, participate in physical exercises, and form a healthy life style. Second, when the provider side shows a lack of initiative, the demand side holds the key to the availability of chronic disease management services. People with higher socio-economic rankings, especially those that have been better educated, care more for their own health condition[11, 12], and are thus more prone to proactively seek health care services. As a result, the availability of being included in health care management is higher among those ranking higher in socio-economic status.
Coping strategy and advices
Based on the analysis above, efforts to improve the outcome of chronic disease management services should be focused on the two aspects below.
Comprehensive approaches to promote the initiative of community health care service providers:
It can be extremely difficult for community health care providers to actively offer diagnosis and management services at the homes of patients with chronic diseases. One of the countermeasures is to reduce the "cost" for community doctors to perform chronic disease management. Currently, automated health examination equipment is already allocated to "community health homes" [13–15] in a few areas, which with a"health ID card" allows residents to easily obtain their measurements, such as height, body weight, BP, and blood glucose. These measured results are then transferred and input into residents' electronic health records (EHRs) [16] so that community doctors can conveniently grasp the health status of community residents, identify patients with chronic diseases or residents with high risks, and provide relevant management services accordingly.
Additionally, it is necessary to reform the incentive mechanism for health care providers. Allowing for relevant experience globally, a "capitation fee" [17–21] based on "contract services of family doctors" could be considered. On the basis of residents "voting with their feet," community doctors could have the "surplus after balancing revenue and expenditures."In this way, if no residents at high risk develop chronic diseases, or conditions of the latter are under steady control, no or less medical resources would be then consumed, and the revenue for community doctors would increase. Eventually,such an incentive mechanism would urge community doctors to expand the coverage of quality health care management services. Moreover, it could also be considered that a special"chronic disease management" budget out of the per capita public health care fund be secured to support the "performance payment" for community doctors. With respect to contracting details, the payment of community doctors could be determined by evaluating the coverage, course, and outcome indices of the chronic disease management services. Similarly, the revenue of community doctors would be directly related to the performance of their services.
Strategies on the prevention and control of chronic diseases covering"socio-economic determinants of health"and community-specific strategies with encouraged participation of local residents:Socio-economic status is extremely influential on the risks of developing chronic diseases [22–26], and people from different socio-economic levels may face different chronic disease risks. Therefore, targeted strategies to prevent and control chronic diseases at different socio-economic levels are necessary for a better service outcome. Specifically, two management measures should be considered.
First, prevention and control strategies should be "lowered" to the level of communities [27–29]. Presently, such strategies are mostly released and executed at the levels of cities or districts in China. The difference between prevention and control strategies of different areas is small, even less between different socio-economic levels of the same area [30]. Communities are aggregations of people from the same socio-economic levels, so it should be preferred to adopt targeted strategies to prevent and control chronic diseases in specific communities as per their own characteristics, and carry out related interventions with the support of local neighborhood committees. All community doctors must be incorporated into the prevention and control services for chronic diseases so that continuing health care guidance could be assured on the premise that the overall condition of patients with chronic diseases and high-risk residents of the specific community is perfectly procured.
Second, more local residents should be encouraged to participate in community strategy that helps to prevent and control chronic diseases. Whether or not a prevention and control strategy could be realized mainly depends on the participation and acceptance of community residents. Hence, local residents should take part in the development of community strategies and action plans to prevent and control chronic diseases, and pass on to others the scientific health concepts which would prove conducive to implementing prevention and control strategies, as well as the health care management service at the community level. Comparatively, community residents could be better motivated to carry out a "self-made" health care action plan than a set of regulations "imposed" by the outside.
This study is a preliminary investigation on community management services for chronic diseases. Although the study does provide evidence to avail future service improvements,the study is limited in sample size, especially with respect to the sample size of diabetic patients, thus the results still have some limitations. More research on this topic needs to be conducted in the future to formulate a better improved management service system that tackles chronic diseases.
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
1. Rothman AA, Wagner EH. Chronic illness management: what is the role of primary care? Ann Intern Med 2003;138:256–61.
2. Yang N, Wei XL, Li HT, Zhang ZZ, Rodas J, Wong SYS, et al.Elderly healthcare service at the community health centers in the Pearl River Delta region, China. Fam Med Community Health 2013;1:30–6.
3. Zhang A, Xia W, Bao Y. Efficiency of community health service in urban and suburban areas of Shanghai: based on production function. Fam Med Community Health 2013;1:5–8.
4. Li LQ, Zhou XJ. Analysis on necessity of community health service development based on limits-to-growth archetype – taking Jiangxi province as an example. Fam Med Community Health 2013;1:20–5.
5. Xu GP. A perspective on the development of family medicine in China. Fam Med Community Health 2014;2:28–34.
6. Zhao LL. Thoughts on community chronic disease service carried out by disease prevention and control institutions. Chin J Prev Contr Chron Non-commun Dis 2014;5:221–3.
7. Chinese Center for Disease Control and Prevention, Bureau of Disease Control and Prevention, Ministry of Health, P.R.China.Report on chronic disease in China 2006.
8. Ministry of Health, et al. China work plan on the prevention and control of chronic diseases (2012–2015). (2012-5-8)[2014-10-13].www.nhfpc.gov.cn/jkj/s5878/201205/167d45ff9ec7492bb9a4e2 a5d283e72c.shtml.
9. Lin Y, Zuo HJ, Feng CR, Zhang J, Liu SQ, Yang XH, et al.Analysis on hypertension control and follow up among elderly patients with hypertension in communities. Chin J Prev Med 2007;2:122–5.
10. Yang JQ, Li YH. The construction and practice of the comprehensive management model on diabetes in communities. Chin J Health Manage 2009;3:242–5.
11. Wang FQ. Socioeconomic status, lifestyle and health inequality.Chin J Soc 2012;2:125–43.
12. Heraclides A, Brunner E. Social mobility and social accumulation across the life course in relation to adult overweight and obesity: the Whitehall II study. J Epidemiol Community Health 2010;64:714–9.
13. Kong LZ. Thoughts on chronic diseases prevention and control in China. Chin J Health Policy 2012;5:2–5.
14. Yang JX, Jiang J. Discussing the strategies for communitybased preventing and controlling chronic diseases in view of its main part. The Chin Health Service Management 2011;10:729–31.
15. Feng W, Zhang JT, Zhu CF, Yin J. The function and significance of "health homes" in community chronic disease management at Community Health Service Centers. JCM 2013;14:64–5.
16. Kushner K, Schell G. A population-based approach to the management of depression in a patient-centered medical home. Fam Med Community Health 2015;3:47–52.
17. Du XP, Hang K. Application of capitation fee in community health institutions. Chin Gene Prac 2013;9:731–3.
18. Jiang Q, Zhang ZZ, Zhao YX, Yu LH, Lang QQ, Chang HH,et al. Thinking of design principles on capitation. Chin Health Economics 2013;1:34–8.
19. Zhao Y, Pan XJ. Strengthen health management functions of primary health care institutions through capitation payment. Chin Health Economics 2013;8:39–41.
20. Lu FW, Gao C, Xu F, Liu GE, Xiong XJ. Capitation payment and first diagnosis reform: Based on analysis of urban household survey. Chin Health Economics 2014;6:37–9.
21. Zhang ZS, Xu AH. Evaluation of capitation reform of payment system on diabetes mellitus. Chin Rural Health Service Administration 2014;9:1058–60.
22. Guo Y, Tang SN. Social determinants of health and chronic disease prevention and control. Chin Prev Med 2010;11:1167–9.
23. Harwood GA, Salsberry P, Ferketich AK, Wewers ME. Cigarette smoking, socioeconomic status, and psychosocial factors: examining a conceptual framework. Public Health Nurs 2007;24:361–71.
24. Colhoun HM, Hemingway H, Poulter NR. Socio-economic status and blood pressure: an overview analysis. J Hum Hypertens 1998;12:91–110.
25. Regidor E, Gutiérrez-Fisac JL, Banegas JR, Domínguez V,Rodríguez-Artalejo F. Association of adult socioeconomic position with hypertension in older people. J Epidemiol Community Health 2006;60:74–80.
26. Zienczuk N, Egeland GM. Association between socioeconomic status and overweight and obesity among Inuit adults: International Polar Year Inuit Health Survey, 2007–2008. Int J Circumpolar Health 2012;71:1–7.
27. Li XM, Huang JS. Exploration of significance and model for the integration of health management and community health delivery on chronic diseases prevention. Chin J Disease Control Prevention 2008;12:53–7.
28. Yang JX, Wang ZZ. Thoughts about strategies for chronic disease integrated control on the basis of community health management. Chin Health Economics 2010;29:67–9.
29. Yang JX, Ma QL. Framework building of the community comprehensive strategy of chronic disease prevention and control.Chin Health Economics 2011;30:55–8.
30. Fan H, Wang QY, Wu YY. Types of community health services selected by urban and suburban residents in Nanjing and influencing factors. Fam Med Community Health 2014;2:8–14.
School of Public Health, Peking University, Haidian District 100191 Beijing, China
Weiyan Jian School of Public Health, Peking University, Haidian District 100191 Beijing, China
E-mail: jianweiyan@bjmu.edu.cn
13 January 2015;
Accepted 9 February 2015
猜你喜欢
杂志排行
Family Medicine and Community Health的其它文章
- Effectiveness of an employment-based smoking cessation assistance program in China
- Team-based stepped care in integrated delivery settings
- The Accountable Care Organization results: Population health management and quality improvement programs associated with increased quality of care and decreased utilization and cost of care
- "Three essential elements" of the primary health care system:A comparison between California in the US and Guangdong in China
- Menopause and the risk of metabolic syndrome among middle-aged Chinese women
- Evaluating the process of mental health and primary care integration:The Vermont Integration Profile