Clinical observation of warm needling moxibustion for rheumatoid arthritis
2015-06-19LinBingbin林兵宾
Lin Bing-bin (林兵宾)
Acupuncture and Tuina Department, Lanxi Hospital of Chinese Medicine, Zhejiang 321100, China
Clinical observation of warm needling moxibustion for rheumatoid arthritis
Lin Bing-bin (林兵宾)
Acupuncture and Tuina Department, Lanxi Hospital of Chinese Medicine, Zhejiang 321100, China
Objective:To observe the clinical efficacy of warm needling moxibustion at points on the back in treating rheumatoid arthritis (RA).
Methods:Sixty RA patients were randomized into two groups by the random number table, 30 in each group. The observation group was intervened by warm needling moxibustion at the points from the Governor Vessel on the back and Jiaji (EX-B 2) points, while the control group was by regular acupuncture.
Results:After intervention, the morning stiffness, joint pain index, joint swelling index and erythrocyte sedimentation rate (ESR) were significantly improved in both groups (P<0.01); the inter-group difference was also statistically significant (P<0.05). The total effective rate was 93.3% in the observation group versus 76.6% in the control group, and the difference was statistically significant (P<0.01).
Conclusion:Warm needling moxibustion at points from the Governor Vessel on the back and Jiaji (EX-B 2) points can produce a higher efficacy than regular acupuncture in treating RA.
Arthritis, Rheumatoid; Warm needling Therapy; Acupuncture-moxibustion Therapy; Moxibustion Therapy; Point, Jiaji (EX-B 2); Governor Vessel
Rheumatoid arthritis (RA) is a systemic inflammatory autoimmune disorder that primarily affects peripheral joints. It’s featured by chronic symmetrical polyarthritis, and regarded as a connective tissue disease that leads to destruction of joints through the erosion of cartilage and bone. The arthritis involves inflammation of the synovial membrane[1]. Because of its high deformity and disability rates, RA has become a common refractory disease. So far, there are limited methods in treating RA. Considering the significant adverse effects of long-term administration of Western medications, acupuncture and moxibustion have attracted more and more attention from the medical fields in China and abroad, as they are safe, cost-effective, and have little side effects. During the recent years, there have immerged a large amount of reports about treating RA with acupuncture and moxibustion, including warm needling moxibustion[2], acupoint injection[3], acupoint threadembedding[4], and bee venom acupuncture[5], etc. However, it’s rarely reported to treat RA with warm needling moxibustion at acupoints on the back. To seek an effective treatment protocol for RA, we adopted warm needling moxibustion to points from the Governor Vessel on the back and Jiaji (EX-B 2) points to tonify yang qi and enhance the immunity. The results are reported as follows.
1 Clinical Materials
1.1 Diagnostic criteria
1.1.1 Diagnostic criteria of Western medicine
According to the diagnostic criteria of RA stipulated by American College of Rheumatology (ACR) in 1987[6]: morning stiffness ≥1 h and disease duration ≥6 weeks; swelling joints ≥3 and lasting for at least 6 weeks; swelling of wrist joints, metacarpophalangealjoints, and proximal interphalangeal joints ≥6 weeks; symmetric swelling joints ≥6 weeks; subcutaneous nodules; radiographic changes of the hand (at least osteoporosis and joint space narrowing); rheumatoid factors positive. RA can be confirmed when 4 of the above 7 items are met.
1.1.2 Diagnostic criteria of Chinese medicine
They are by referring the diagnostic criteria of joint Bi-impediment syndrome from the Criteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine[7]: localized pain and swelling in joints, morning stiffness that affects movement, aggravated by cold, and aversion to cold in the affected areas.
1.2 Inclusion criteria
Conforming to the above diagnostic criteria of Western and Chinese medicine; age between 20 and 65 years old; willing to participate in the study and having signed the informed consent form.
1.3 Exclusion criteria
Those who have been using immunosuppressants, Penicillamine, Chloroquine, or gold preparations for a long time; pregnant women or women during lactation period; those who with severe disorders of liver, kidney, lung, or cardio-cerebrovasucular diseases; having a history of serious drug allergy.
1.4 Statistical method
The SPSS 11.0 version statistical software was used for data processing. The measurement data were expressed by mean ± standard deviation analyzed by t-test; the enumeration data were analyzed by Chi-square test. A P value <0.05 presents a statistical significance
1.5 General data
Totally 60 RA patients were enrolled from the outpatient of our hospital. The subjects were numbered according to their visiting sequence and then randomized into an observation group and a control group by using the random number table, 30 patients in each group. In the observation group, the age range was 21-65 years old; in the control group, the age range was 20-63 years old. The statistical analyses showed that there were no significant differences in comparing data of gender, age, and disease duration (P>0.05), indicating that the comparability (Table 1).
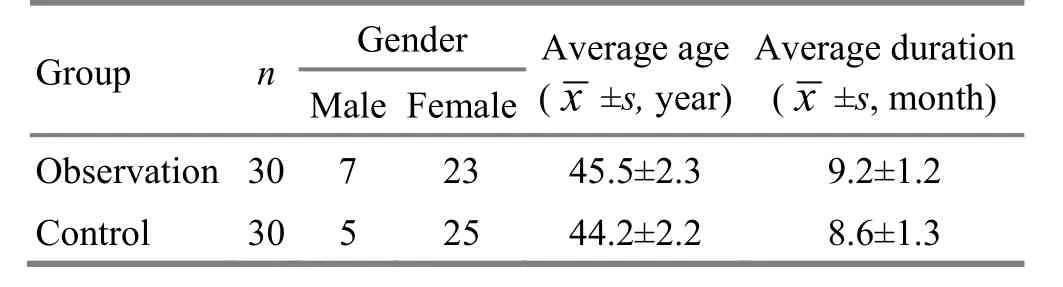
Table 1. Between-group comparison of general data (case)
2 Treatment Methods
2.1 Observation group
2.1.1 Points
Major points: Dazhui (GV 14), Shendao (GV 11), Zhiyang (GV 9), Mingmen (GV 4), and Jiaji (EX-B 2) points.
Adjunct points: Baihui (GV 20), bilateral Fengchi (GB 20), and Jianjing (GV 21).
2.1.2 Methods
The patient was seated, straddling a straight chair, with hands rest on the back of the chair. After sterilization, filiform needles of 0.25 mm in diameter and 40 mm in length were used to perpendicularly insert into Dazhui (GV 14), Shendao (GV 11), Zhiyang (GV 9), and Mingmen (GV 4) by 25 mm. Afterwards, Jiaji (EX-B 2) points (0.5 cun away from T1, T3, T5, T7, T11, L1, and L3) were punctured with the needle tip towards the spine by an angle of 45°. When needling qi was obtained, Baihui (GV 20) was applied with even reinforcing-reducing manipulation. Bilateral Fengchi (GB 20) and Jianjing (GB 21) were punctured by 25 mm. When needling qi was obtained, 6-8 points were selected crosswise from the major points to receive warm needling moxibustion, i.e. T1, T5, T9, and L1Jiaji (EX-B 2) points were selected from the left side, then T3, T7, T11, and L3Jiaji (EX-B 2) points would be selected from the right side. A moxa roll of 1.5 cm in length was placed onto the handle of the needle and ignited from the bottom. It usually took about 15 min to burn out one segment of moxa, which would be replaced by another one. Each point was treated with two segments.
2.2 Control group
2.2.1 Points
Points selection by syndrome differentiation: For Bi-impediment syndrome due to wind, Geshu (BL 17) and Xuehai (SP 10) were selected; for Bi-impediment syndrome due to cold, Shenshu (BL 23) and Guanyuan (CV 4) were selected; for Bi-impediment syndrome due to damp, Pishu (BL 20) and Yinlingquan (SP 9) were selected.
Topical points selection: The points were selected depending on the affected joints including Jianzhen (SI 9), Quchi (LI 11), Waiguan (te 5), Yangxi (LI 5), Baixie (EX-UE 9), Xuehai (SP 10), Dubi (ST 35), Zusanli (ST 36), Kunlun (BL 60), Zhaohai (KI 6), Bafeng (EX-LE 10), and Ashi points around the affected joints.
The above points were selected on both sides.
2.2.2 Needling methods
Filiform needles of 0.25 mm in diameter and 40 mm in length were used for acupuncture treatment after standard sterilization with even reinforcing-reducing manipulation.
For both groups, the needles were retained for 30-40 min, 10 d as a treatment course, 3 courses in total with an interval of a week between two courses.
3 Therapeutic Efficacy
3.1 Measurements
The two groups were evaluated before and after intervention. According to the diagnostic criteria of RA stipulated by the ACR in 1987[6], the following items were estimated: joint swelling index (sum of the swelling degree of the joints), joint tender index (sum of the tender degree of the joints), and morning stiffness duration. The erythrocyte sedimentation rate (ESR) was also detected before and after intervention.
3.2 Criteria of therapeutic efficacy
The Criteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine[7]were referred.
Markedly effective: Symptoms were gone, swelling and pain were relieved from the affected joints, the joint function was restored normal, and the laboratory examinations showed normal.
Improved: Symptoms were reduced, the swelling and pain of joints were reduced, the function of joints was improved, and the laboratory examinations also showed improvement.
Invalid: Symptoms still existed, the function of the joints was not improved and the laboratory examinations didn’t show improvement.
3.3 Treatment result
3.3.1 Comparison of symptoms and examinations
In the observation group, the morning stiffness duration, joint tender index, joint swelling index, and ESR were significantly improved after the intervention (P<0.01). After treatment, there were significant differences in comparing the morning stiffness duration, joint tender index, joint swelling index, and ESR between the two groups (P<0.05), (Table 2).
Table 2. Comparison of symptom score and ESR

Table 2. Comparison of symptom score and ESR
Note: Compared with pre-treatment result in the same group, 1) P<0.01; com pared with the control group after intervention, 2) P<0.05
Group n Time Morning stiffness (h)Joint tender index Joint swelling index ESR (mm/h) Observation 30 Before treatment 1.5±0.54 9.7±0.45 6.8±0.51 37.05±11.26 After treatment 0.2±0.121)2)2.5±0.471)2)2.6±0.621)2)10.35±5.081)2)Control 30 Before treatment 1.6±0.41 9.2±0.47 6.6±0.56 38.58±9.05 After treatment 0.6±0.171)4.3±0.511)4.45±0.521)29.10±12.31)
3.3.2 Comparison of therapeutic efficacy
The total effective rate was 93.3% in the observation group versus 76.6% in the control group, and the difference was statistically significant according to Chi-square test (P<0.01), indicating that the therapeutic efficacy of the observation group is higher than that of the control group (Table 3).

Table 3. Comparison of clinical efficacy (case)
4 Discussion
RA is a chronic systemic disease of unknown etiology. The major symptoms are persistent pain, swelling, deformity, and impaired function of the affected joints. If it’s not treated properly, RA will lead to joint deformity which may seriously affect daily life. Western medicine treats RA majorly by relieving pain. In traditional Chinese medicine, RA falls under the scope of joint Bi-impediment and it’s caused by deficiency in the root and excess in the manifestations. The deficient healthy qi should be the key factor in the development of this disease. When the deficient healthy qi fails to protect the body from invasion of external pathogens, the pathogens such as wind, cold, and damp will intrude and block meridians, tendons and bones, subsequently leading to stagnation in blood vessels, accumulation of body fluids, blocked Ying-Nutrient and Wei-Defensive qi, phlegm and stasis, and thus there occurs RA. The pathogenic factors of RA can be summarized to be deficiency, pathogen, and stagnation. Therefore, RA should be treated by tonifying the healthy qi to defend the external pathogens or to expel the contracted pathogens.
The Governor Vessel is the sea of the yang meridians, i.e. the gathering place of the yang meridians. It functions to regulate the general yang qi and activate the body function. The Governor Vessel is closely related to the kidney, brain, and marrow, and directly or indirectly associated with Zang-fu organs and meridians. Therefore, stimulating the points from the Governor Vessel can modulate the qi-blood of all meridians and the function of Zang-fu organs[8]. Baihui (GV 20), Dazhui (GV 14), Shendao (GV 11), Zhiyang (GV 9), andMingmen (GV 4) are where the yang qi of the Governor Vessel accumulates. Baihui (GV 20) works to enhance yang qi; Dazhui (GV 14) is the crossing point of the hand and foot yang meridians with the Governor Vessel, and it can reinforce yang qi to expel cold and regulate the general yang qi; Shendao (GV 11) tonifies yang qi and calms mind; Zhiyang (GV 9) supplements yang qi of the heart and lung and also tonifies qi and blood; Mingmen (GV 4) works to strengthen kidney yang, and cultivate the primordial.
Jiaji (EX-B 2) points are located in between the Governor Vessel and Bladder Meridian of Foot Taiyang, and connected with Zang-fu organs, brain, and marrow via meridians. According to the Western medicine, the distribution of Jiaji (EX-B 2) points is extremely related to the spinal nerves. The posterior branches of spinal nerves run through this group of points, which should be the major neurophysiological foundation of the action of Jiaji (EX-B 2) points. Acupuncture at Jiaji (EX-B 2) points does not only unblock and regulate the qi-blood of meridians, but also modulate the sensory and motor nerves[8-10]. Fengchi (GB 20) is the crossing point of the Meridian of Foot Shaoyang and Yang Link Vessel, and works to dispel wind and refresh mind.
When moxa is burning, the heat can be induced into skins, muscles, tendons, and bones via the acupuncture needles, working to dilate capillaries, accelerate the topical circulation of blood and lymph, promote metabolism, for dispelling cold and damp, supplementing qi and blood, and activating blood circulation to relieve impediment. Besides, moxibustion can trigger the production of heat shock protein, and the heat shock protein further evokes the immune system, which is believed to be a significant action mechanism of moxibustion[11-12]. Warm needling therapy combines the needling and moxibustion, producing both the effects of acupuncture and moxibustion to warm meridians and expel cold[13-15].
The current study shows that warm needling moxibustion at the back points can significantly relieve the symptoms of RA, enhance the immune function, and it can produce a higher therapeutic efficacy than regular acupuncture.
Conflict of Interest
There was no conflict of interest in this article.
Statement of Informed Consent
All of the patients in the study signed the informed consent.
[1] Chen HZ. Internal Medicine. Beijing: People’s Medical Publishing House, 1996: 804.
[2] Qi Y, Yang R. Warm needling moxibustion plus medication for acute rheumatoid arthritis. Zhenjiu Linchuang Zazhi, 2009, 25(1): 40-41.
[3] Gu Y, Xie JP, Yang Y. Acupoint injection with Xue Lian for 60 rheumatoid arthritis. Shanxi Zhongyi, 2009, 25(3): 30.
[4] Gao DR, Gao DG, Gao L, Lu J, Yang LX, Hong JG. Efficacy of acupoint thread-embedding for rheumatoid arthritis. Shanghai Zhenjiu Zazhi, 2007, 26(5): 27.
[5] Liu XD, Zhang JL, Zheng HG, Liu FY, Chen Y. Clinical randomized study of bee-sting therapy for rheumatoid arthritis. Zhen Ci Yan Jiu, 2008, 33(3): 197-200.
[6] Arnett FC, Edworthy SM, Bloch DA. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum, 1988, 31: 315-334.
[7] State Administration of Traditional Chinese Medicine. Criteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine. Nanjing: Nanjing University Press, 1994: 29.
[8] Cao Y, Li PF, Chen XS. Simple analysis on Professor ZHANG Dao-zong's academic thought of dredging the Governor Vessel and regulating mentality. Zhongguo Zhen Jiu, 2006, 26(10): 741-743.
[9] Zhang XR, Wang X, Sun CL, Wang Y. Expression of NF-κB in spinal ganglia of CIA rats and therapeutic action of acupuncture Jiaji points. Xiandai Zhongxiyi Jiehe Zazhi, 2007, 16(11): 1460-1462.
[10] Li G, Wang XJ, Ge HQ, Niu HC, Han JF, Zhang HS, Tan HC, Li XZ. Study of Chinese medicine paster on negative emotion and quality of life in patients with ankylosing spondylitis. Xiandai Zhongxiyi Jiehe Zazhi, 2010, 19(24): 2999-3001.
[11] Song JL, Fan FJ, Han ZP, Hong WX. Advances of studies on traditional moxibustion therapy for treatment of cancer. Zhongguo Zhen Jiu, 2006, 26(3): 227-229.
[12] Xu L, Wang YS. Relationship of acupuncture and heat shock protein. Liaoning Zhongyiyao Daxue Xuebao, 2011, 13(1): 204-206
[13] Wu CJ, Liu WZ, Liu JP, Xie X. Effect of warm needling moxibustion on pain index and substance P in patients with lumbar intervertebral disc protrusion. Zhonguo Zhongyi Gushang Zazhi, 2008, 16(8): 35-36.
[14] He QY, Zhang J. Professor ZHANG Ji's clinical experience. Zhongguo Zhen Jiu, 2006, 26(12): 890-892.
[15] Mei J, Yang ZR, Li H. Therapeutic observation of early-stage and mid-stage knee osteroarthristis treated with warm needling. Shanghai Zhenjiu Zazhi, 2014, 33(1): 52-54.
Translator: Hong Jue (洪珏)
温针灸治疗类风湿性关节炎临床观察
目的:观察温针灸背部腧穴对类风湿性关节炎(rheumatoid arthritis, RA)的临床疗效。方法:将60例RA患者按随机数字表随机分为2组,每组30例。观察组采用温针灸背部督脉穴及夹脊穴治疗,对照组采用常规针刺治疗。结果:治疗后,两组患者晨僵、关节疼痛指数、关节肿胀指数及红细胞沉降率(erythrocyte sedimentation rate, ESR)都有明显改善,与本组治疗前差异均有统计学意义(P<0.01);观察组与对照组亦有统计学差异(P<0.05)。观察组总有效率为93.3%,对照组为76.6%,两组总有效率差异有统计学意义(P<0.01)。结论:温针灸背部督脉穴及夹脊穴治疗RA的疗效优于常规针刺治疗。
关节炎,类风湿; 温针疗法; 针灸疗法; 灸法; 穴,夹脊; 督脉
R246.2 【
】A
30 August 2014/Accepted: 15 October 2014
Author: Lin Bing-bin, bachelor, associate chief physician of traditional Chinese medicine.
E-mail:2684888272@qq.com
猜你喜欢
杂志排行
Journal of Acupuncture and Tuina Science的其它文章
- Therapeutic effect of tuina combined with Jin Gui Shen Qi Decoction on lumbar spinal stenosis
- Electroacupuncture down-regulates the expressions of colonic NGF and NGFR in visceral hypersensitivity rats
- Summary of Professor Jin Yi-cheng’s academic thoughts on pediatric tuina therapy
- Triple needling plus moxibustion and Tanbo-plucking tender points for the third lumbar vertebra transverse process syndrome
- Effect of ginger-partitioned moxibustion on immunocytokines in patients with chronic nonbacterial prostatitis
- Effect of row needling in muscle regions combined with seven-star needle tapping on cognitive function and quality of life in patients with post-stroke upper limb spasticity