Therapeutic effect of tuina combined with Jin Gui Shen Qi Decoction on lumbar spinal stenosis
2015-06-19ShangYong尚永ChenGuangmin陈广敏TangShujie唐树杰
Shang Yong (尚永), Chen Guang-min (陈广敏), Tang Shu-jie (唐树杰)
1 Department of Orthopaedics, Qingzhou Hospital of Traditional Chinese Medicine, Shandong 262500, China
2 Department of Traditional Chinese Medicine, Medical School, Jinan University, Guangzhou 510632, China
Special Topic Study
Therapeutic effect of tuina combined with Jin Gui Shen Qi Decoction on lumbar spinal stenosis
Shang Yong (尚永)1, Chen Guang-min (陈广敏)1, Tang Shu-jie (唐树杰)2
1 Department of Orthopaedics, Qingzhou Hospital of Traditional Chinese Medicine, Shandong 262500, China
2 Department of Traditional Chinese Medicine, Medical School, Jinan University, Guangzhou 510632, China
Objective: To study the effect of tuina combined with Jin Gui Shen Qi Decoction on lumbar spinal stenosis.
Methods: In the prospective study, seventy outpatients were divided into a treatment and a control group, 36 cases in the treatment group and 34 in the control group. The treatment group was treated with tuina combined with Jin Gui Shen Qi Decoction, but the control group was treated using tuina alone. The therapeutic effect was evaluated using Japanese Orthopaedic Association (JOA) score.
Results: No significant difference in JOA score was found between the two groups before treatment (P>0.05), but significant improvements were found in both groups after treatment and at the final follow-up (P<0.05), and the JOA score in the treatment group was significantly higher than that in the control group (P<0.05). After treatment and at the final follow-up, the therapeutic effect in the treatment group was significantly better (P<0.05).
Conclusion: Tuina combined with Jin Gui Shen Qi Decoction was more effective than tuina alone for lumbar spinal stenosis.
Tuina; Massage; Jin Gui Shen Qi Decoction; Spinal Stenosis; Low Back Pain
Low back pain is the most common symptom in lumbar disorders, among which lumbar spinal stenosis is associated with narrowing of the spinal canal, resulting in chronic low back pain and unilateral or bilateral leg symptoms[1]. Degenerative change is the most common etiology, and with the increasing of life expectancy, more and more people may suffer from the disease. Subsequently, the treatment of lumbar stenosis should be highlighted. Although the treatment of lumbar stenosis is controversial, most scholars recommend conservative therapy as the first choice.
In the field of orthopaedics and traumatology of traditional Chinese medicine (TCM), tuina is a common non-surgical method to treat low back pain, which was reported by many researchers[2-6]. In a randomized trial, Cherkin DC, et al concluded that tuina can provide long-lasting benefits to low back pain[7]. Some clinical reports confirmed the effect of tuina on lumbar spinal stenosis[8-11], and nowadays tuina has been widely used in treating lumbar spinal stenosis.
Jin Gui Shen Qi Decoction is a prescription in Jin Gui Yao Lue (Synopsis of Prescriptions of the Golden Chamber) written by Zhang Zhong-jing, a famous physician of TCM, used to treat low back pain due to asthenia of viscera in Han Dynasty. Nowadays, Jin Gui Shen Qi Decoction has also been reported in treating lumbar spinal stenosis[12]and lumbar disc herniation[13-14]. While, in clinics, most physicians pay high attention to external therapy such as tuina, moxibustion or acupuncture, but ignore the internal therapy such as traditional drugs and herbs in treating lumbar degenerative disc disease.
However, combined internal and external therapy is one of the important treatment principles inorthopedics and traumatology of TCM[15]. According to the principle, when treating fracture, dislocation, injury of tendon and muscle or spinal degenerative disc disease, internal therapy and external therapy should be used together, which can facilitate the recovery of trauma or other diseases. Subsequently, we assumed tuina combined with Jin Gui Shen Qi Decoction may have better effect than either method alone. However, few studies have been published on the issues in English literatures.
In order to compare the effect of tuina combined with Jin Gui Shen Qi Decoction and tuina alone in treating lumbar spinal stenosis, and to help physicians of TCM make treatment strategies, we treated 70 cases with lumbar spinal stenosis between September 2010 and July 2012. Now, we report it as follows.
1 Clinical Materials
1.1 Diagnostic criteria
Neurogenic intermittent claudication, as noted by leg/buttock/groin pain with or without back pain or fatigue in the legs provoked by walking, needs to be relieved by lumbar flexion; narrowed lumbar spinal canal, nerve root canal or intervertebral foramen at one or more levels confirmed by MRI.
1.2 Inclusion criteria
Met with the aforementioned diagnostic criteria; no age or gender limitation; with clear consciousness and ability to communicate effectively and to cooperate with the treatment.
1.3 Exclusion criteria
Cauda equine syndrome; Paget’s disease, severe osteoporosis or metastasis to the vertebrae; significant scoliosis (Cobb angle >25°); previous laminectomy, degenerative or lytic spondylolisthesis (≥grade 2) at the affected level or significant instability of the lumbar spine; severe comorbidity that increases the risk to the patient or interfere with the assessment of the study (e.g. severe ischemic heart disease, musculoskeletal or neurological conditions impairing walking ability, cognitive impairment).
1.4 Statistical analysis
Statistical analysis was performed by using SPSS 17.0 version statistical software. The comparisons of mean age, follow-up period and duration between the two groups were performed by One-way analysis of variance. The comparisons of gender and stenosis level were processed by using Chi-square test. The difference in treatment effect between the two groups was evaluated by paired-sample t-test and Wilcoxon signedrank test. A P value of <0.05 was considered to indicate a statistical significance.
1.5 Patients and design
This prospective controlled trial was carried out in Qingzhou Hospital of Traditional Chinese Medicine between September 2010 and July 2012. Seventy patients were included in the current study, including 28 females and 42 males. After the baseline evaluation, an independent researcher took a sealed opaque envelope for each case, from a box following a numerical sequence generated by a computer, which contained a piece of paper indicating whether the patient belonged to the treatment or the control group. There were 36 cases in the treatment group and 34 cases in the control group. The current study was approved by the Institutional Review Board of our hospital, all the patients voluntarily joined this study with informed consents. There were no statistical differences between the two groups in the basic conditions such as age, gender, lumbar stenosis level, duration and follow-up period (all P>0.05), it indicated that the two groups were comparable (Table 1).

Table 1. Patient demographics and parameters in the current study
2 Treatment Methods
2.1 Treatment group
2.1.1 Tuina therapy
The patient takes a prone position. The operator applies Gun-rolling manipulation along the Bladder Meridian for 5 min (Figure 1). Next, An-presses and Rou-kneads Weizhong (BL 40), Yinlingquan (SP 9), Taixi (KI 3), Mingmen (GV 4), Dachangshu (BL 25), Shenshu (BL 23), 20 s for each point (Figure 2). And then applies Ca-rubbing manipulation to the Bladder Meridian and the Governor Vessel on the back (Figure 3), transversely Ca-rubs the lumbosacral area until a localized warm sensation occurs. After that, the operator stands on one side of the patient's head, applies a Tui-pushing manipulation along the Bladder Meridian 2-3 times withone or two hands (Figure 4). Finally, the operator Pai-taps from the upper back to the sacrum until the local skin turns slightly red (Figure 5).
Tuina was performed once daily, with ten days for one therapeutic course.
2.1.2 Jin Gui Shen Qi Decoction
Composition: Shu Di Huang (Radix Rehmanniae Preparata) 30 g, Shan Yao (Rhizoma Dioscoreae) 20 g, Shan Zhu Yu (Fructus Corni) 20 g, Mu Dan Pi (Cortex Moutan) 15 g, Fu Ling (Poria) 15 g, Gui Zhi (Ramulus Cinnamomi) 10 g, Fu Zi (Radix Aconiti Lateralis Preparata) 10 g, and Ze Xie (Rhizoma Alismatis) 15 g.

Figure 1. Gun-rolling manipulation

Figure 2. An-pressing and Rou-kneading manipulations

Figure 4. Tui-pushing manipulation
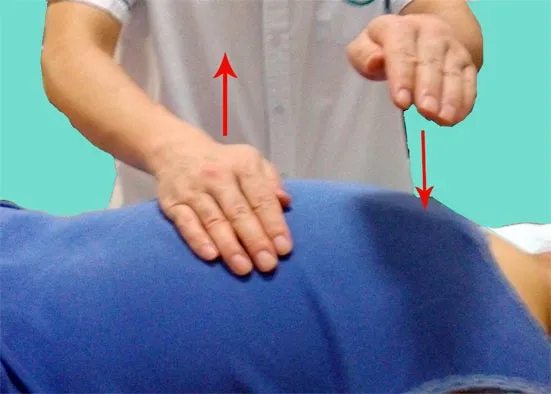
Figure 5. Pai-tapping manipulation
Modified: Gan Jiang (Rhizoma Zingiberis) was added for severe cold. Fang Ji (Radix Stephaniae Tetrandrae) was added for severe dampness. Zao Ren (Semen Ziziphi Spinosae) was added for insomnia. Rou Cong Rong (Herba Cistanches) or Jiu Da Huang (Radix et Rhizoma Rhei) was added for constipation. Sang Piao Xiao (Ootheca Mantidis) was added for clear abundant urine or profuse urination at night.
The decoction was orally taken, one dose a day, in the morning and evening on an empty stomach, for ten days as a therapeutic course.
2.2 Control group
In the control group, the patients were treated by using tuina alone, with the same manipulations and treatment courses as those for the treatment group.
The therapeutic effect was evaluated in the two groups after four therapeutic courses and at the final follow-up.
3 Therapeutic Effect Observation
3.1 Criteria for the therapeutic effect.
The Japanese Orthopedics Association (JOA) score was used to assess the clinical outcomes (Table 2)[16]. A perfect score is 29 points.
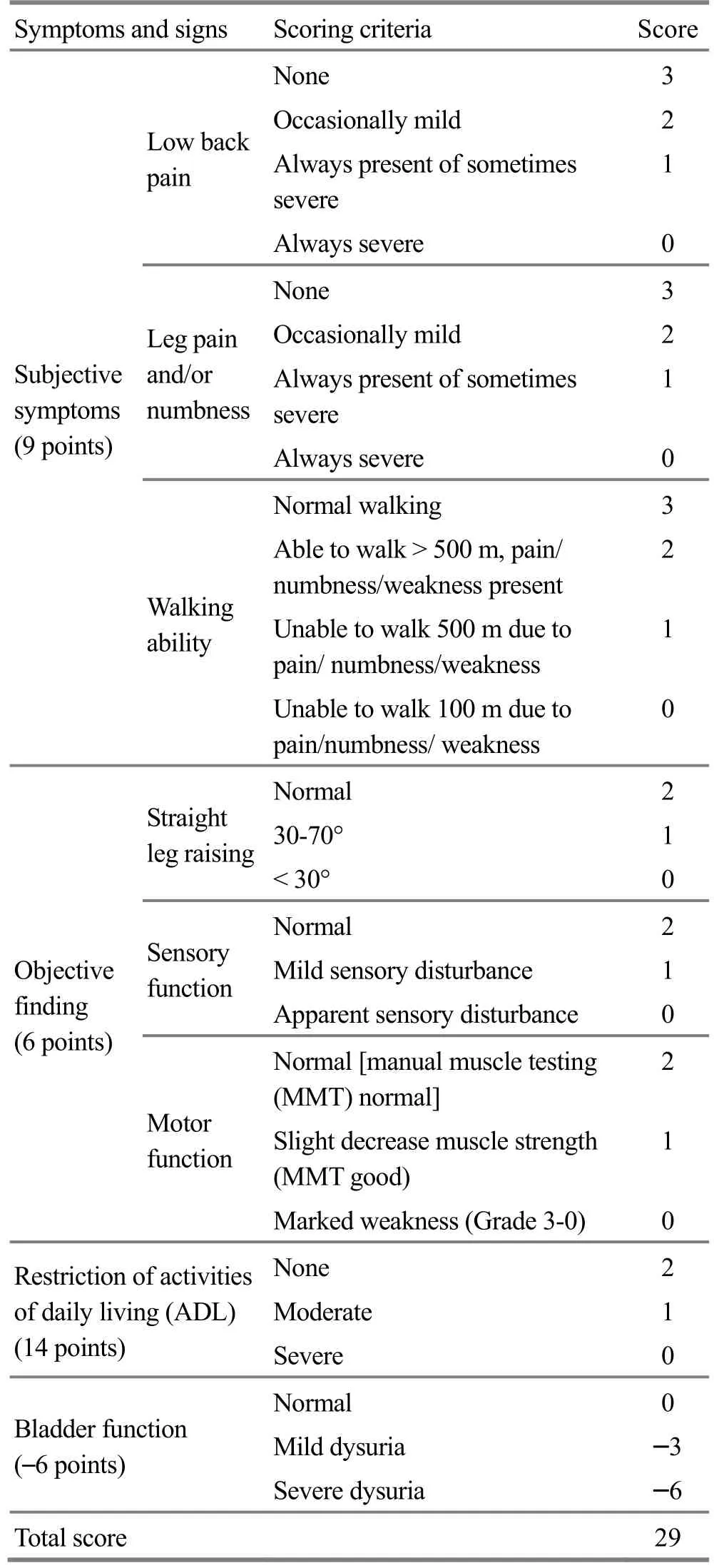
Table 2. JOA for lower back pain
JOA recovery rate (%) = (JOA score at the final follow-up - JOA score before treatment)÷ (29 -JOA score before treatment) × 100[17].
Treatment outcomes were assessed based on JOA recovery rate[18].
Excellent: JOA recovery rate ≥90%.
Good: JOA recovery rate ≥75%, but ≤89%.
Fair: JOA recovery rate ≥50%, but ≤74%.
Poor: JOA recovery rate ≤49%.
3.2 Results
3.2.1 Comparison of the JOA score
The JOA scores of the two groups were listed in Table 3, and there was no significant difference in JOA score between the two groups before treatment. However, significant improvements of JOA were observed in both groups after treatment and at the final follow-up. The JOA score in the treatment group was significantly increased after treatment, and at the final follow-up (P<0.05), and the control group also increased significantly after treatment and at the final follow-up (P<0.05). In addition, the JOA scores after treatment and at the final follow-up were significantly higher in the treatment group than those in the control group(P<0.05), (Table 3).
Table 3. Comparison of the JOA score between the two groups
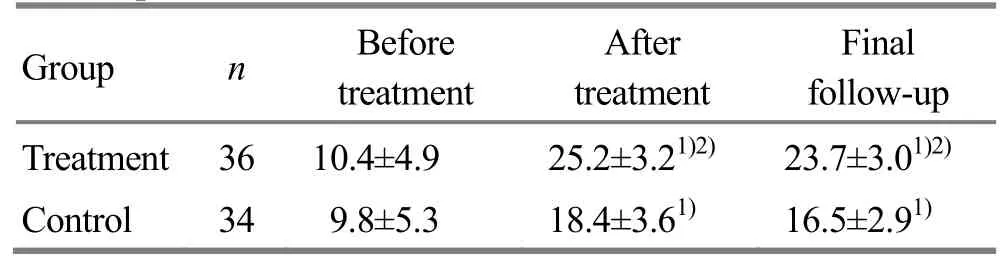
Table 3. Comparison of the JOA score between the two groups
Note: Intra-group comparison, 1) P<0.05; compared with the control group at same time, 2) P<0.05
Group n Before treatment After treatment Final follow-up Treatment 3610.4±4.9 25.2±3.21)2)23.7±3.01)2)Control 349.8±5.3 18.4±3.61)16.5±2.91)
3.2.2 Comparison of therapeutic effect
After treatment, in the treatment group, 15 patients achieved an excellent result, 14 patients got a good result, 7 patients got a fair result. In the control group, 8 patients achieved an excellent result, 11 patients got a good result, 11 patients got a fair result and 4 patients got a poor result. The therapeutic effect is significantly better in the treatment group than that in the control group (P<0.05), (Table 4).
Similarly, at final follow-up, in the treatment group, 14 patients achieved an excellent result, 13 patients got a good result, 8 patients got a fair result and 1 patient got a poor result. In the control group, 7 patients achieved an excellent result, 10 patients got a good result, 12 patients got a fair result and 5 patients got a poor result. The therapeutic effect is significantly better in the treatment group than that in the control group (P<0.05), (Table 5).
Table 4. Comparison of therapeutic effect after treatment between the two groups

Table 4. Comparison of therapeutic effect after treatment between the two groups
Note: Compared with the control group, 1) P<0.05
Group n Excellent Good Fair Poor Excellent rate (%) Total effective rate (%) Treatment 36 15 14 7 0 41.7 1001)Control 34 8 11 11 4 23.5 88.2
Table 5. Comparison of therapeutic effect at final follow-up between the two groups

Table 5. Comparison of therapeutic effect at final follow-up between the two groups
Note: Compared with the control group, 1) P<0.05
Group n Excellent Good Fair Poor Excellent rate (%) Total effective rate (%) Treatment 36 14 13 8 1 38.9 97.2 Control 34 7 10 12 5 20.6 85.2
4 Discussion
Lumbar spinal stenosis, resulted from degenerative changes of central canal, lateral recess, foramina or any combination of these locations, is one of the most commonly reasons to produce low back pain. The stenosis leads to the compression of cauda equine or nerve roots, promotes edema or aseptic inflammation of nervous tissue, and subsequently, low back pain or intermittent claudication occurs[19-20].
The disease belongs to the category of lumbago in the field of orthopedics and traumotology of TCM. TCM holds that the pathogenic factors, such as wind, dampness, cold, heat, sprain, static blood, qi stagnation and congealing phlegm, are all secondary factors for low back pain, while kidney deficiency is the primary factor. Lumbago is closely correlated with injury, wind-cold-dampness and strain, but kidney deficiency is the primary etiology[15]. Consequently, in the field of TCM, lumbar stenosis is attributed to kidney deficiency, and it should be treated mainly with tonifying kidney, accompanied by dissipating cold, dispelling dampness, activating blood, and so on.
In the current study, tuina was performed along the Governor Vessel and Bladder Meridian, which can regulate the meridians and collaterals of low back, dredge the meridian and collaterals, reduce the excess and tonify the deficient kidney. The JOA score in the control group improved after treatment, demonstrating the definite effect of tuina on lumbar spinal stenosis. Although tuina can’t release the spinal stenosis resulted from hyperosteogeny or ossification of ligaments, but it can improve the blood circulation, facilitating the decrease of the local edema and aseptic inflammation of nervous tissue, and subsequently relieve the compression on nervous tissue and improve the symptoms of low back pain[21]. The current outcome is consistent with some reports[7-11].
In the recipe of Jin Gui Shen Qi Decoction, Shu Di Huang (Radix Rehmanniae Preparata) acts as sovereign medicinal to tonify yin and kidney. Shan Zhu Yu (Fructus Corni) and Shan Yao (Rhizoma Dioscoreae) act as ministerial medicinal to tonify the liver and boost the spleen to reinforce essence and blood, in which Shan Zhu Yu (Fructus Corni) can tonify the kidney and liver, and Shan Yao (Rhizoma Dioscoreae) can nourish kidney and enrich essence. In addition, Fu Zi (Radix Aconiti Lateralis Preparata) and Gui Zhi (Ramulus Cinnamomi) can warm the kidney and reinforce yang, supplement fire of life gate and return fire to its source. Ze Xie (Rhizoma Alismatis), Fu Ling (Poria) and Mu Dan Pi (Cortex Moutan Radicis) act as assistant medicinal, among which Ze Xie (Rhizoma Alismatis) can regulate the waterways and discharge heat in kidney, Fu Ling (Poria) can fortify the spleen and percolate dampness, and Mu Dan Pi (Cortex Moutan Radicis) can clear ministerial fire in liver and gallbladder[22]. In addition, the medicines for activating blood, dispelling wind-dampness, and dispersing cold were added according to syndrome differentiation.
Therefore, Jin Gui Shen Qi Decoction is one of the famous decoctions to tonify kidney. When used in patients with low back pain resulted from degenerative disc disease, both true yin and yang in kidney will be reinforced, and kidney qi will be supplemented[22-23], which aims at the primary pathogenesis of lumbago and facilitate the symptom removing. In the current study, the JOA score in the treatment group is significantly increased after treatment and at the final follow-up. In addition, 14 patients achieved an excellent result and 13 patients a good result in treatment group at the final follow-up, presenting with an excellent rate of 38.9%. While in the control group, 7 patients achieved an excellent result and 10 patients a good result, and the excellent rate was 20.6%. The therapeutic effect is significantly better in treatment group than that in the control group. This demonstrates the effect of Jin Gui Shen Qi Decoction combined with tuina improved significantly in treating lumbar spinal stenosis. In addition, the current study confirmed the correctness of the principle of combined internal and external therapy in orthopedics and traumatology of TCM.
To sum up, the current study confirmed that tuina combined with Jin Gui Shen Qi Decoction was moreeffective than tuina alone. However, the period of follow-up in the present study is short, and a prospective trial studied during a long-term follow-up would certainly provide more useful information. Subsequently, more studies would need to be performed in the future.
Conflict of Interest
The authors declared that there was no potential conflict of interest.
Statement of Informed Consent
All of the patients in the study signed the informed consent.
[1] Genevay S, Atlas SJ. Lumbar spinal stenosis. Best Pract Res Clin Rheumatol, 2010, 24(2): 253-265.
[2] Zheng Z, Wang J, Gao Q, Hou J, Ma L, Jiang C, Chen G. Therapeutic evaluation of lumbar tender point deep massage for chronic non-specific low back pain. J Tradit Chin Med, 2012, 32(4): 534-537.
[3] Zhang J, Han L, Wang P, Yu D, Lu M, Lin DK, Song TB, Lin JH, Sun SC. Observation of clinical curative effect of‘oblique-pulling’ maneuver in the treatment of lumbar intervertebral disc herniation. Zhongguo Gu Shang, 2010, 23(2): 84-86.
[4] Feng W, Feng TY, Wang F, Bi YM, Wang SQ. Treatment of the lumbar disc herniation of sequestered type with Feng's spinal manipulation. Zhongguo Gu Shang, 2008, 21(7): 529-531.
[5] Fang M, Zhu QG, Hong SZ. Analysis of the principle of lever about adjustment of spinal ‘Gucuofeng’ with manipulative maneuver. Zhongguo Gu Shang, 2010, 23(10): 780-783.
[6] Kong LJ, Fang M, Zhan HS, Yuan WA, Pu JH, Cheng YW, Chen B. Tuina-focused integrative Chinese medical therapies for inpatients with low back pain: a systematic review and meta-analysis. Evid Based Complement Alternat Med, 2012, 2012: 578305.
[7] Cherkin DC, Eisenberg D, Sherman KJ, Barlow W, Kaptchuk TJ, Street J, Deyo RA. Randomized trial comparing traditional Chinese medical acupuncture, therapeutic massage, and self-care education for chronic low back pain. Arch Intern Med, 2001, 161(8): 1081-1088.
[8] Pang RC, Zhang AR, Hu B, Zhao JN, Yang HP, Wang HG. Treating lumbar spinal stenosis using kinesitherapy and tuina. Zhonguo Kangfu, 2006, 21(6): 397.
[9] Zhang Y, Chen P, Ke JL. Treating lumbar spinal stenosis using tuina and fumigating and washing: report of 112 cases. Zhejiang Zhongyi Zazhi, 2010, 45(11): 838-839.
[10] Cai K. Tuina treating lumbar degenerative spinal stenosis: report of 56 cases. Zhongyi Zhenggu, 1999(3): 27-28.
[11] Liu HB. Tuina treating lumbar spinal stenosis: report of 38 cases. Xiandai Kangfu, 2000, 14(7): 1051.
[12] Song CY. Jin Gui Shen Qi pill treating lumbar degenerative spinal stenosis in old people: report of 48 cases. Liaoning Zhongyi Zazhi, 1997, 24(3): 23.
[13] Yang ST. Jin Gui Shen Qi pill treating lumbar disc herniation: report of 30 cases. Zhongguo Yiyao Zhinan, 2011, (32): 396-397.
[14] Yang GX. Jin Gui Shen Qi pill treating lumbar disc herniation: report of 15 cases. Hubei Zhongyi Zazhi, 1997, 19(2): 18.
[15] Tang S, Liu F. Treating thoracic verterbra related disease using chiropractic combined with Du Huo Ji Sheng Decoction. Chin J Sports Med, 2012, 31(8): 681-683.
[16] Hioki A, Miyamoto K, Hosoe H, Sugiyama S, Suzuki N, Shimizu K. Cantilever transforaminal lumbar interbody fusion for upper lumbar degenerative diseases (minimum 2 years follow up). Yonsei Med J, 2011, 52(2): 314-321.
[17] Ogawa H, Hori H, Oshita H, Akaike A, Koyama Y, Shimizu T, Yamada K, Ishimaru D. Sublaminar wiring stabilization to prevent adjacent segment degeneration after lumbar spinal fusion. Arch Orthop Trauma Surg, 2009, 129(7): 873-878.
[18] Chen Z, Zhao J, Liu A, Yuan J, Li Z. Surgical treatment of recurrent lumbar disc herniation by transforaminal lumbar interbody fusion. Int Orthop, 2009, 33(1): 197- 201.
[19] Kim YS, Park SJ, Oh IS, Kwan JY. The clinical effect of gait load test in two level lumbar spinal stenosis. Asian Spine J, 2009, 3(2): 96-100.
[20] Inoue M, Kitakoji H, Yano T, Ishizaki N, Itoi M, Katsumi Y. Acupuncture treatment for low back pain and lower limb symptoms: the relation between acupuncture or electroacupuncture stimulation and sciatic nerve blood flow. Evid Based Complement Alternat Med, 2008, 5(2): 133-143.
[21] Su CM. Tuina treating lumbar spinal stenosis: review of literatures. Anmo Yu Daoyin, 2008, 24(1): 43-45.
[22] Qian Z. Treatment of chronic low back pain using Liu Wei Di Huang pill and Jin Gui Shen Qi pill. Shangdong Zhongyi Zahi, 2006, 25(9): 609.
[23] Zhao C. Treatment of lumbar disc herniation using Jin Gui Shen Qi pill: a report of twenty cases. Changchun Zhongyiyao Daxue xuebao, 2011, 27(1): 109.
推拿结合金匮肾气汤治疗腰椎椎管狭窄症疗效分析
目的:探讨推拿结合金匮肾气汤治疗腰椎管狭窄症的疗效。方法:将70例腰椎管狭窄症门诊患者随机分为两组,治疗组36人,对照组34人。治疗组采用推拿结合内服金匮肾气汤治疗,对照组仅采用推拿治疗。根据日本骨科协会(Japanese Orthopaedic Association, JOA)腰痛评分评价疗效。结果:治疗前两组JOA评分无明显差异((P>0.05);治疗后与最后随访两组评分均有明显改善(P<0.05),而且治疗组评分明显高于对照组(P<0.05);治疗后与最后随访,治疗组疗效均优于对照组(P<0.05)。结论:推拿结合金匮肾气汤治疗腰椎管狭窄症疗效优于单纯推拿治疗。
推拿; 按摩; 金匮肾气汤; 椎管狭窄; 腰痛
R246.2 【
】A
18 July 2014/Accepted: 25 September 2014
Author: Shang Yong, bachelor, attending physician
Tang Shu-jie, M.D., associate professor.
E-mail: wkdd2009@hotmail.com
猜你喜欢
杂志排行
Journal of Acupuncture and Tuina Science的其它文章
- Effect of acupuncture combined with rehabilitation training on walking function after arthroscopic meniscus repair
- Professor Tian Cong-huo’s commonly used acupuncture methods and their clinical application
- Electroacupuncture combined with iontophoresis of Chinese medicine for lumbar intervertebral disc herniation
- Effect of row needling in muscle regions combined with seven-star needle tapping on cognitive function and quality of life in patients with post-stroke upper limb spasticity
- Effect of ginger-partitioned moxibustion on immunocytokines in patients with chronic nonbacterial prostatitis
- Triple needling plus moxibustion and Tanbo-plucking tender points for the third lumbar vertebra transverse process syndrome