Electroacupuncture combined with iontophoresis of Chinese medicine for lumbar intervertebral disc herniation
2015-06-19ZhangJinpeng张金朋TangQiang唐强ZhuLuwen朱路文
Zhang Jin-peng (张金朋), Tang Qiang (唐强), Zhu Lu-wen (朱路文)
1 Heilongjiang University of Traditional Chinese Medicine, Harbin 150040, China
2 The Second Hospital Affiliated to Heilongjiang University of Traditional Chinese Medicine, Harbin 150001, China
Electroacupuncture combined with iontophoresis of Chinese medicine for lumbar intervertebral disc herniation
Zhang Jin-peng (张金朋)1, Tang Qiang (唐强)2, Zhu Lu-wen (朱路文)2
1 Heilongjiang University of Traditional Chinese Medicine, Harbin 150040, China
2 The Second Hospital Affiliated to Heilongjiang University of Traditional Chinese Medicine, Harbin 150001, China
Objective:To observe the clinical efficacy of electroacupuncture (EA) combined with iontophoresis of Chinese medicine for lumbar intervertebral disc herniation (LIDH).
Methods:A total of 80 LIDH cases were randomly allocated into a treatment group and a control group by the random number table, 40 in each group. Cases in the treatment group were treated with EA combined with iontophoresis of Chinese medicine, whereas cases in the control group were treated with EA alone. Cases in both groups were treated once a day, 10 times for one course and there was a 3-day interval between two courses. The therapeutic efficacies in two groups were assessed after two courses of treatment. The short-form McGill pain questionnaire (SF-MPQ) and Japanese Orthopedic Association (JOA) low back pain evaluation questionnaire were used for the scoring system before treatment, after the first treatment and 2 courses of treatment.
Results:After two courses of treatment, the total effective rate was 95.0% in the treatment group, versus 87.5% in the control group, showing a statistical difference (P<0.05). The therapeutic efficacy in the treatment group was significantly better than that in the control group after the first treatment and 2 courses of treatment. The score of SF-MPQ in the treatment group was more significantly decreased and the JOA score in the treatment group was more significantly increased, showing statistical differences (P<0.01).
Conclusion:EA at Jiaji (EX-B 2) points combined with iontophoresis of Chinese medicine is better than EA alone in alleviating low back and leg pain and improving functions of the low back and leg as well as the quality of life of LIDH patients.
Intervertebral Disc Displacement; Low Back Pain; Electroacupuncture; Acupuncture Therapy; Point, Jiaji (EX-B 2); Drugs, Chinese Herbal; Iontophoresis
lumbar intervertebral disc herniation (LIDH) refers to rupture of the annulus fibrosus due to trauma or degenerative changes and subsequent outward or backward protrusion of the nucleus pulposus, which in turn compresses the nerve root and cauda equina, leading to a series of symptoms including low back and leg pain. As a common and frequently encountered medical condition, LIDH can greatly affect the patients’daily living and work. At present, conservative therapy is mostly used for LIDH treatment. Approximately 80%-90% of the LIDH patients can benefit fromnon-surgical treatment. However, some patients may not respond well to conservative therapy[1]. To explore a more effective treatment protocol for LIDH, we’ve treated LIDH with EA combined with iontophoresis of Chinese medicine. The results are now summarized as follows.
1 Research Data
1.1 Diagnostic criteria
There is no standardized diagnostic criterion for LIDH yet. The diagnostic criteria in this study were based on the Criteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine issued by the State Administration of Traditional Chinese Medicine in 1994[2]: a history of lumbar trauma, strain or contraction of cold-dampness and chronic low back pain; young adults; low back pain that radiates towards the buttocks and leg and aggravates upon increased abdominal pressure (such as sneezing or coughing); scoliosis, absence of lumbar physiological curve, presence of tenderness spots along the affected vertebrae that radiate towards the leg and restricted low back movement; hyperesthesia or dysesthesia in the region served by affected nerve roots, muscular atrophy in those with an extended period of LIDH, positive Lasègue's or Bragard's sign, weakness or absence of knee and ankle jerk reflex, and weakness of the great toe in dorsal extension; X-ray examination findings of scoliosis, absence of lumbar physiological curve, narrowing of affected intervertebral space or presence of osteophyte; and herniated location and severity confirmed by CT scan.
1.2 Inclusion criteria
Those who met the above diagnostic criteria and were confirmed by CT scan (suspected cases were ruled out by MRI examination); showing indications of conservative treatment; aged between 20 and 60 years with a clear consciousness and were cooperative in collecting clinical data; willingly accepted the test and control plan and signed the informed consent.
1.3 Exclusion criteria
Those who failed to meet the above diagnostic and inclusion criteria; having lumbar spinal stenosis, spinal facet joint disorders, cauda equina tumor, lumbar fasciitis, epidural tumor, radiculitis or piriformis syndrome; having congenital lumbosacral deformity, tuberculosis or fracture; having hemorrhagic tendency, active tuberculosis or implanted pacemaker; pregnant women; having complications of other severe medical or mental problems; sciatica related to other conditions; having severe heart, lung and kidney insufficiencies; and those who were reluctant to participate in this study and dropped out voluntarily.
1.4 Drop-out and rejection criteria
Failure to complete the treatment courses due to faint during acupuncture treatment and stuck or broken needles; those who accepted other therapies or medicine during this study or failed to comply with the random allocation; having deteriorated condition or severe complications during the treatment; and those who have previously participated in this study.
1.5 Statistical analysis

1.6 General materials
A total of 80 outpatients and inpatients at the Rehabilitation Center, the Second Hospital Affiliated to Heilongjiang University of Traditional Chinese Medicine between March 2013 and August 2014 were randomly allocated into a treatment group and a control group by random number table, 40 in each group. There were 39 males and 41 females. The patients were aged between 20 and 60 years, with an average age of 43.6 years. Their duration lasted from 2 weeks to 5 years. There were no between-group statistical differences in gender, age and duration (P>0.05), indicating that the two groups were comparable (Table 1).

Table 1. Between-group comparison of general materials
2 Treatment Methods
2.1 Treatment group
2.1.1 EA at lumbar Jiaji (EX-B 2) points
Major points: Jiaji (EX-B 2) points on both sides of the affected vertebrae (LIDH confirmed by CT scan or MRI examination) and adjacent superior/inferior vertebra, Huantiao (GB 30) on the affected side and Ashi points.
Adjunct points: Yanglingquan (GB 34) on the affected side for herniated L4-5; and Weizhong (BL 40) on the affected side for herniated L5-S1.
Method: Disposable filiform needles of 0.30 mm in diameter and 40-75 mm in length were used in this study. With a prone lying position of the patient, bilateral Jiaji (EX-B 2) points were punctured with filiform needles of 50 mm in length perpendicularly (slightly towards the spine, depth: approximately40 mm), followed by even reinforcing-reducing manipulation upon needling sensation. The best effect can be achieved if the needling sensation radiates down to the buttock and leg on the affected side. Huantiao (GB 30) was punctured with a filiform needle of 75 mm in length. The rest points were punctured with filiform needles of 40 mm in length perpendicularly and followed by even reinforcing-reducing manipulation upon needling sensation. Then the needles at Jiaji (EX-B 2) points of the affected and adjacent superior/ inferior vertebrae were connected with KWD-8081 electric stimulator[3], using opposite electrodes for adjacent wires (Figure 1), a sparse-dense wave (2 Hz/100 Hz)[4-5]and tolerable intensity. Each treatment lasted 30 min.

Figure 1. Electroacupuncture
2.1.2 Iontophoresis
Ingredients: Twenty-five gram of Qiang Huo (Rhizoma et Radix Notopterygii), Du Huo (Radix Angelicae Pubescentis), Xuan Shen (Radix Scrophulariae), Bi Xie (Rhizoma Dioscoreae Hypoglaucae), Sheng Di Huang (Radix Rehmanniae), Shu Di Huang (Radix Rehmanniae preparata), Dang Gui (Radix Angelicae Sinensis), Du Zhong (Cortex Eucommiae), Fang Feng (Radix Saposhnikoviae), Rou Gui (Cortex Cinnamomi), Gui Zhi (Ramulus Cinnamomi) and Bai Zhi (Radix Angelicae Dahuricae) respectively and 30 g of Ru Xiang (Olibanum), Mo Yao (Myrrha) and Tian Ma (Rhizoma Gastrodiae) respectively.
Method: The LD-AE low and medium frequency thermal treatment device was used in this study. First, soak the cotton pads in approximately 1 000 mL of decoction. Next, squeeze and dry the cotton pads. Then, place the decoction-soaked cotton pads over the electrodes, positive electrodes on both sides of the herniated disc and negative electrodes on radiated pain or tenderness spots on the buttocks. Finally, place sand pockets to compress and immobilize. The treatment lasted 30 min within the patient’s tolerance (Figure 2).
Cautions: Contraindicated for skin lesion.
2.2 Control group
The treatment was conducted once a day, 10 times made up a course of treatment. There was a 3-day interval between two courses. The therapeutic efficacies were observed after two courses of treatment.

Figure 2. Iontophoresis of Chinese medicine
3 Therapeutic Efficacy Observation
3.1 Observation indices
3.1.1Short-form McGill pain questionnaire (SF-MPQ)[6]
The SF-MPQ was used to assess pain intensity. The scale consists of the following three parts.
Pain rating index (PRI): This includes 11 sensory words and 4 affective words in four qualities, none, mild, moderate and severe, corresponding to 0, 1, 2, and 3 points. The sensory score, affective score and global score can all be calculated.
Visual analogue scale (VAS): This usually adopts a horizontal line, 10 cm in length, anchored by word descriptors at each end, no pain (0) and worse pain imaginable (10). The patient marks on the line the point that they feel represents their perception of their current state. The distance from the ‘0’ end to the point the patient marked is considered the VAS score.
Present pain intensity (PPI): This includes no pain, mild, discomforting, distressing, horrible and excruciating, corresponding to 0, 1, 2, 3, 4, and 5.
The scores were calculated before treatment, after the first treatment and after two courses of treatment respectively.
3.1.2 Japanese Orthopaedic Association (JOA) low back pain evaluation questionnaire[7]
The JOA low back pain scoring system was adopted in this study to evaluate the improvement of lumbar function. It includes 4 items: subjective symptoms,clinical signs, daily living and bladder function. Each item has one or more questions. The global score is 29 points. A lower score indicates a worse functional disturbance.
3.2 Therapeutic efficacy evaluation
The therapeutic efficacies were evaluated on the basis of JOA scale[7]and the Criteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine[2].
JOA improvement rate = (Post-treatment JOA score— Pre-treatment JOA score) ÷ (29 — Pre-treatment JOA score) × 100%.
Recovery: JOA improvement rate ≥95%, absence of low back and leg pain, >70°of straight leg raise and almost return to normal life and work.
Marked effect: JOA improvement rate ≥60% but<95%, almost absence of low back and leg pain,>50°of straight leg raise and normal lumbar function that does not affect daily living and work.
Improvement: JOA improvement rate ≥25% but<60%, alleviation of low back and leg pain and better lumbar function that still affects daily living and work.
Failure: JOA improvement rate <25% and the signs and symptoms remain unchanged.
3.3 Treatment results
3.3.1 Comparison of clinical effects
After two courses of treatment, the total effective rate in the treatment group was 95.0%, versus 87.5% in the control group (P<0.05), indicating a statistical difference and a better effect in the treatment group than that in the control group (Table 2).

Table 2. Between-group comparison of therapeutic efficacies (case)
3.3.2 Comparison of SF-MPQ scores
Before treatment, there were no between-group statistical differences in comparing PRI, VAS and PPI scores (P>0.05). The PRI, VAS and PPI scores in both groups were significantly decreased after the first treatment, showing statistical differences (P<0.01). After two courses of treatment, these scores continued to decrease and showed a statistical difference compared with the scores after the first treatment (P<0.01). There were between-group statistical differences in comparing PRI, VAS and PPI scores after the first and two courses of treatment (P<0.01), showing a more significant decrease in the treatment group. This indicates that EA at lumbar Jiaji (EX-B 2) points combined with iontophoresis of Chinese medicine can obtain better analgesic effect than EA alone. In addition, the effect tends to increase with time (Table 3).
Table 3. Between-group comparison of SF-MPQ scores before and after treatment

Table 3. Between-group comparison of SF-MPQ scores before and after treatment
Note: Intra-group comparison before and after treatment, 1) P<0.01; intra-group comparison before and after the first treatment, 2) P<0.01; inter-group comparison in corresponding period, 3) P<0.01
Time Treatment group (n=40) Control group (n=40) PRI VAS PPI PRI VAS PPI Before treatment 26.38±1.98 7.94±1.02 4.80±0.72 27.10±2.03 8.12±0.89 4.65±0.92 After the first treatment 12.50±2.661)4.08±1.251)3)2.56±0.521)3)13.18±1.521)5.21±1.471)2.95±0.711)After 2-course treatment 6.43±3.681)2)3)1.26±0.981)2)3)0.88±0.641)2)3)9.76±2.141)2)2.81±0.841)2)1.79±0.521)2)
3.3.3 Comparison of JOA scores
Before treatment, there were no between-group statistical differences in JOA score (P>0.05). After the first and 2-course treatment, there were intra-group statistical differences in JOA scores (P<0.01). In addition, there were statistical differences between 2-course treatment and the first treatment (P<0.01). After the first and 2-course treatment, there were between-group statistical differences in JOA scores (both P<0.01), (Table 4).
Table 4. Between-group comparison of JOA scores before and
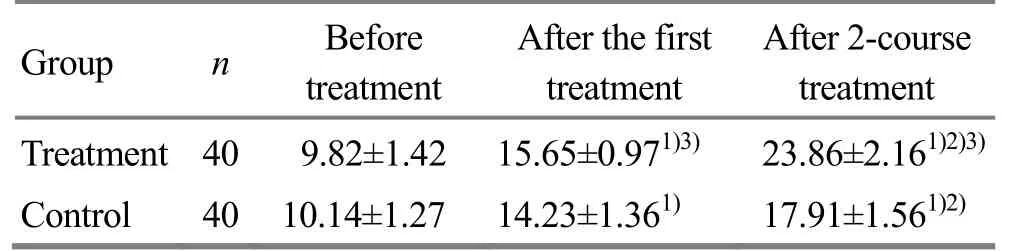
Table 4. Between-group comparison of JOA scores before and
Note: Intra-group comparison before and after treatment, 1) P<0.01; intra-group comparison before and after the first treatment, 2) P<0.01; inter-group comparison in corresponding period, 3) P<0.01
Group nBefore treatment After the first treatment After 2-course treatment Treatment 409.82±1.42 15.65±0.971)3)23.86±2.161)2)3)Control 4010.14±1.27 14.23±1.361)17.91±1.561)2)
4 Discussion
In Chinese medicine, LIDH falls under the category of‘low back and leg pain’, ‘Bi-impediment syndrome’ or‘Wei-flaccidity syndrome’. It commonly affects L4-5and L5-S1. Jiaji (EX-B 2) points are often used in acupuncture for LIDH[8], because needling these points can directly work on the affected tissue and also systematically regulate the nervous and immune systems through the association between meridians and modern anatomy[9]. Lumbar Jiaji (EX-B 2) points are located 0.5 cun lateral to the spine. Divergent meridians of the Governor Vessel and The Bladder Meridian travel along the spine. Jiaji (EX-B 2) points are located in between the two meridians and associated with the meridians and muscle regions of the Governor, Conception and Thoroughfare Vessels and Spleen, Stomach and Kidney Meridians. Consequently, needling Jiaji (EX-B 2) points can circulate qi and blood of multiple meridians, alleviate pain, harmonize yin and yang, unblock meridians and thus alleviate low back and leg pain. In modern medicine, lumbar Jiaji (EX-B 2) points are close to the nerve root. Therefore, needling these points on the affected side can directly stimulate the corresponding spinal nerve, influence the vegetative nerve and regulate functions of internal organs, boost metabolism and blood circulation. Furthermore, needling these points can relax lumbar muscle groups, nurture surrounding tissues, accelerate absorption of inflammatory edema and relieve clinical symptoms of LIDH[10].
EA at Jiaji (EX-B 2) points can stimulate deeper muscles (erector spinae), generate rhythmic contraction and relaxation, restore dynamic and static balance of the lumbar vertebrae and improve lumbar functions. In addition, electric stimulation on Jiaji (EX-B 2) points can also improve microcirculation of the affected area, speed up cell metabolism, transform or degrade inflammatory substances and increase absorption of edema[11]. EA can alleviate pain by inhibiting the pathological reaction in the cerebral cortex through increasing opioid peptide release of periphery inflammatory tissues[12]. EA at contralateral Jiaji (EX-B 2) points[3,13-14]can help to eliminate aseptic inflammation in intervertebral space through the current impulse, alleviate inflammatory irritation, and relieve compression to the nerve root. Through rhythmic muscle contraction generated by sparse-dense wave[15], EA can accelerate tissue metabolism, nurture the surrounding tissue and absorb inflammatory edema.
Through one-way modulated middle frequency impulse current, iontophoresis of Chinese medicine enables ion of Chinese herbal medicine to enter the body and directly work on the affected area. At the same time, the middle frequency impulse current can work on deeper muscles, stimulate nerve roots, accelerate metabolism and alleviate pain. In addition, it can also increase blood circulation, relax muscles, unblock meridians and achieve the double treatment effect of Chinese medication and middle frequency electrotherapy[16].
The research findings have shown that EA at Jiaji (EX-B 2) points combined with iontophoresis of Chinese medicine can obtain double and synergetic effect for LIDH and achieve better clinical efficacy and scores than EA alone. This indicates that this method can significantly improve the therapeutic efficacy in LIDH patients, improve their lumbar functions and speed up their recovery. As a result, this method is worthy of further application.
Conflict of Interest
The authors declared that there was no conflict of interest in this article.
Acknowledgments
This work was supported by the Top Talent Program of Heilongjiang University of Traditional Chinese Medicine (黑龙江中医药大学领军人才计划项目, No.2012RCL02); Science & Technology Innovation Team Program in Heilongjiang Colleges and Universities (黑龙江省高校科技创新团队计划项目, No. 2013TD007).
Statement of Informed Consent
Informed consent was obtained from all individual participants included in this study.
Received: 16 September 2014/Accepted: 25 October 2014
[1] Liang GW. Therapeutic efficacy observation on comprehensive rehabilitation therapy for lumber disc herniation. Zhonghua Wuli Yixue Yu Kangfu Zazhi, 2009, 31(3): 191-193.
[2] State Administration of Traditional Chinese Medicine. Criteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine. Nanjing: Nanjing University Press, 1994: 214-215.
[3] Yang SB, Mei ZG, Cai SJ, Chen JH, Zhou C. Clinical observation on treatment of different connectors used in electroacupuncture at Jiaji (EX-B 2) points for treatment of relapsed lumbar disc herniation. Hubei Zhongyi Zazhi, 2011, 33(6): 14-16.
[4] Ma GZ, Zhang Y, Chen L, Feng XX. Comparative study on the therapeutic efficacies of electroacupuncture with various waves for lumbar disc herniation and the effect on serum interleukin 6. Shanghai Zhenjiu Zazhi, 2014, 33(2): 153-156.
[5] Wang Y, Zhang Y, Wang W, Cao Y, Han JS. New evidence in synergetic analgesic effect of endomorphin and dynorphin. Zhongguo Tengtong Yixue Zazhi, 2002, 8(2): 118 -119.
[6] Miu HS. Theory and Practice of Rehabilitation Medicine.Shanghai: Shanghai Scientific & Technical Publishers, 2000: 1167-1168.
[7] Liu ZX. Common Diagnostic Classification Methods and Functional Assessment Criteria in Orthopedics. Beijing: Beijing Science and Technology Press, 2005: 335, 339-340.
[8] Lu YY. Chinese herbal fumigation combined with electroacupuncture at Jiaji (EX-B 2) points for lumbar disc herniation in 60 cases. Zhongguo Zhongyiyao Keji, 2012, 19 (1): 87-88.
[9] Wu WQ, Liu FM, Guo YP. Application and action mechanism of Jiaji (EX-B 2) points in lumbar disc herniation. Zhongguo Zhongyi Jizheng, 2011, 20(12): 1997-1998.
[10] Guo HQ. Needling Jiaji (EX-B 2) points for lumbar disc herniation in 43 cases. Zhongyi Zazhi, 2007, 48(4): 338-339.
[11] Zhao JY. Electroacupuncture at lumbar Jiaji (EX-B 2) points for lumbar disc herniation. JCAM, 2008, 24(4): 10-11.
[12] Yan HL, Tao RG, Cao J, An J. Electroacupuncture for lumbar disc herniation in 31 cases. JCAM, 2002, 18(5): 39-40.
[13] Yuan FG, Liu F. Electroacupuncture using electrodes connecting lumbar vertebrae for lumbar disc herniation in 96 cases. Hebei J TCM, 2003, 25(10): 767-768.
[14] Li L, Yuan K, Zhang LH, Wang H. Randomized controlled observation on treating lumbar disc herniation by EA at Jiaji (EX-B 2) points. Zhonghua Zhongyiyao Xuekan, 2013, 31(3): 630-632.
[15] Chen XH, Guo SF, Han JS. Selection of optimal analgesic stimulation using sparse-dense wave in electroacupuncture. Beijing Yike Daxue Xuebao, 1993, 25(5): 338.
[16] Cai YL, Wang SS, Wang Y. Observation and TCM care on low-temperature radiofrequency ablation combine with iontophoresis of Chinese medicine for lumbar disc herniation. Neimenggu Zhongyiyao, 2014, (6): 93.
Translator: Han Chou-ping (韩丑萍)
电针结合中药离子导入治疗腰椎间盘突出症
目的:观察电针腰夹脊穴配合中药离子导入治疗腰椎间盘突出症(lumbar intervertebral disc herniation,LIDH)的疗效。方法:采用随机数字表法将80例LIDH患者随机分为观察组和对照组,每组40例。观察组采用电针腰部夹脊穴结合中药离子导入治疗,对照组采用与观察组相同的电针治疗。两组患者均每日治疗1次,10次为1个疗程,2个疗程中间休息3 d,治疗2个疗程后进行疗效观察。治疗前、首次治疗后及治疗2个疗程后,进行简式McGill 疼痛询问量表(short-form McGill pain questionnaire, SF-MPQ)和日本骨科协会(Japanese Orthopedic Association, JOA)下腰痛评分量表评分。结果:经2个疗程治疗后,治疗组总有效率为 95.0%,对照组为87.5%,两组总有效率差异有统计学意义(P<0.05);其中首次治疗与2个疗程治疗后比较,治疗组的疗效均明显优于对照组,SF-MPQ评分均明显降低,下腰痛JOA评分升高明显,治疗组更为显著,差异有统计学意义(P<0.01)。结论:电针腰夹脊穴结合中药离子导入能够有效缓解LIDH患者的腰腿痛,改善腰腿部功能障碍,从而提高患者的生活质量,其疗效优于单纯电针腰夹脊穴。
椎间盘移位; 腰痛; 电针; 针刺疗法; 穴,夹脊; 中草药; 离子导入
R246.2 【
】A
in the control group
the same EA (points and stimulation parameters) as the treatment group.
Author: Zhang Jin-peng, master degree candidate
Tang Qiang, professor.
E-mail: tangqiang1963@163.com
猜你喜欢
杂志排行
Journal of Acupuncture and Tuina Science的其它文章
- Effect of acupuncture combined with rehabilitation training on walking function after arthroscopic meniscus repair
- Professor Tian Cong-huo’s commonly used acupuncture methods and their clinical application
- Effect of row needling in muscle regions combined with seven-star needle tapping on cognitive function and quality of life in patients with post-stroke upper limb spasticity
- Effect of ginger-partitioned moxibustion on immunocytokines in patients with chronic nonbacterial prostatitis
- Triple needling plus moxibustion and Tanbo-plucking tender points for the third lumbar vertebra transverse process syndrome
- Summary of Professor Jin Yi-cheng’s academic thoughts on pediatric tuina therapy