Clinical observation on warm needling therapy for scapulohumeral periarthritis: a randomized controlled trial
2015-05-18ChenYingchun陈迎春FengZhengen冯祯根
Chen Ying-chun (陈迎春), Feng Zhen-gen (冯祯根)
Acupuncture Department, Jinhua Hospital of Traditional Chinese Medicine, Zhejiang 321000, China
Tang Shu-jie (唐树杰)
Department of Traditional Chinese Medicine, Medical School, Jinan University, Guangzhou 510632, China
Clinical Study
Clinical observation on warm needling therapy for scapulohumeral periarthritis: a randomized controlled trial
Chen Ying-chun (陈迎春), Feng Zhen-gen (冯祯根)
Acupuncture Department, Jinhua Hospital of Traditional Chinese Medicine, Zhejiang 321000, China
Objective:To evaluate the clinical effects of warm needling for scapulohumeral periarthritis (SP).
Acupuncture-moxibustion Therapy; Acupuncture Therapy; Warm Needling Therapy; Periarthritis; Shoulder Pain; Randomized Controlled Trial
The scapulohumeral periarthritis (SP) is mainly characterized by pain and loss of motion or stiffness in the shoulder joint[1]. In early stage, patients often experience paroxysmal pain. Inducing factors include fatigue and external contraction of cold-dampness. Over time, patients may experience persistent pain that aggravates at night and alleviates during the day, inability to lie on the affected side and restricted active and passive ranges of motion. This condition is often seen in people around the age of 50 and affects more women than men. Chinese medicine, especially acupuncture has been proven very effective for SP. We’ve treated a total of 43 SP cases due to wind, cold and dampness with warm needling between September 2012 and August 2014 and compared with acupuncture alone. The results are now summarized as follows.
1 Clinical Materials
1.1 Diagnostic criteria
In reference to the relevant diagnostic criteria of SP in theCriteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional ChineseMedicine[2]: commonly seen in women around the age of 50, affects more right shoulder than the left shoulder, coupled with an insidious onset; shoulder pain that aggravates at night and is often triggered by weather changes and fatigue, and restrict movement of the shoulder. In severe cases, muscular atrophy of the shoulder and arm may be present; physical examination shows generalized tenderness below the acromion, limited shoulder movement in abduction, extension, external rotation and lifting, coupled with an inability to undress or comb one’s hair; contributing factors include chronic strain, trauma or external contraction of wind-cold mostly positive in X-ray film, and osteoporosis present in those with long duration. In terms of pattern identification in Chinese medicine, it belongs to wind, cold and dampness, mainly manifested as migrating pain in the shoulder, aggravated by wind and cold and relieved by warm, aversion to wind and cold, or heavy sensation in the shoulder, a pale tongue with thin and white or greasy coating, a wiry and slippery or wiry and tense pulse.
1.2 Inclusion criteria
In conformity with the above diagnostic criteria and of wind, cold and dampness pattern in Chinese medicine; no limitation in gender; willing to participate in this study and signed the informed consent.
1.3 Exclusion criteria
Those not in conformity with the above diagnostic criteria; those complicated with skin conditions or lesions; difficult to assess the therapeutic effects due to administration of non-steroidal anti-inflammatory and analgesic medications in recent one week; women in pregnancy or ready for pregnancy; those with allergic body constitution; those with difficulty to make precise evaluation about the efficacy and safety of the therapeutic effects due to mental or conscious disorder; and those joining or ready for joining the other clinical trials.
1.4 Statistical analysis
All data were analyzed and processed by SPSS 19.0 version software. The measurement data were expressed by mean ± standard deviationThe pairedt-test was used for comparison within the group. The independent samplet-test was applied in comparison between the groups. The Chi-square test was used for comparison of the enumeration data between the groups. APvalue <0.05 was used to indicate the difference of statistical significance.
1.5 Case sources and grouping
A total of 86 cases in conformity with the inclusion criteria, treated in the acupuncture department in our hospital from September of 2012 to August of 2014, were selected and randomly divided into an observation group and a control group by their visit order. The differences were not statistically significant in gender, average age and average duration between the two groups (allP>0.05), indicating that the two groups were comparable (Table 1).
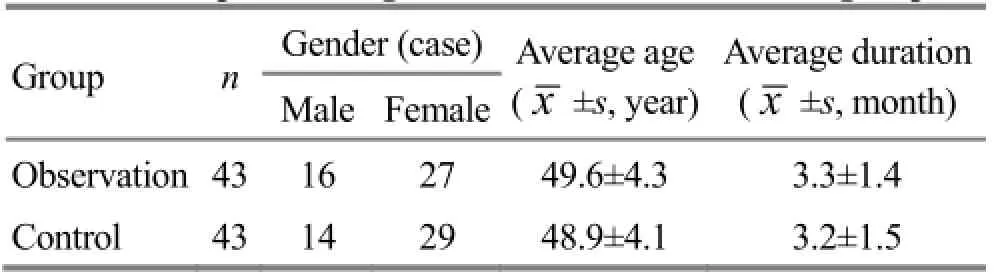
Table 1. Comparison of general data between the two groups
2 Therapeutic Methods
2.1 Observation group
The patients in the observation group were treated by warm needling moxibustion.
Acupoints: Jianyu (LI 15), Jianliao (TE 14), Jianzhen (SI 9), Jianqian (Extra) and Ashi point.
Method: After the patient took a sitting position and the local skin of the acupoints were disinfected, the disposable filiform needles of 0.35 mm in diameter and 50 mm in length were inserted quickly and manipulated by the lifting, thrusting and twisting technique till the patient had the local sore, numb, distending and painful sensation. Then, a pure moxa roll of 2 cm in length was put on the handle of every needle, about 3 cm above the skin, and ignited at the bottom. After one piece of moxa was burnt out, another piece was used. Each time, two pieces were burnt. In order to avoid causing accidental scalding, it was necessary to put a piece of folded paper on the skin of the acupoint. The needles were taken out after the second moxa section was burnt out. The needles were retained for about 30 min. The treatment was given once every day and 10 sessions made one course, two courses in total.
2.2 Control group
The patients in the control group were only treated by acupuncture. The selection and location of the acupoints, needling methods and therapeutic process were as same as those in the observation group.
3 Observation of Therapeutic Effects
3.1 Observed indexes
The scores of visual analogue scale (VAS) were used to assess the change of the patient’s shoulder pain before and after the treatment. 0 point expressed no pain, and 10 points expressed the most serious pain.
3.2 Criteria of therapeutic effects
The criteria of the therapeutic effects were self stipulated in reference to the criteria of the therapeutic effects for SP in theCriteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine[2].
Cure: Shoulder pain disappeared, and the activity of the shoulder joint was basically restored.
Remarkable effective: Shoulder pain disappeared basically, and the activity of the shoulder joint was basically normal. But, sore and heavy sensation still existed under fatigue or obvious climatic change.
Effective: Shoulder pain was relieved, and the activity of the shoulder joint was improved.
Failure: Before and after the treatment, there was no obvious change or even aggravation in pain and motor impairment.
3.3 Results
The patients in the two groups all completed the relevant study, without dropped-off case and serious adverse reaction.
3.3.1 Comparison of VAS scores before and after the treatment between the two groups
In the comparison of VAS scores before the treatment between the two groups, there was no statistical difference (P>0.05). In the comparison of the scores before and after the treatment within the two groups, the differences were statistically significant (P<0.05).
After treatment, the score of pain was obviously lower in the observation group than that in the control group, with a statistical difference (P<0.05), (Table 2).
Table 2. Comparison of VAS scores between the two groups, point)
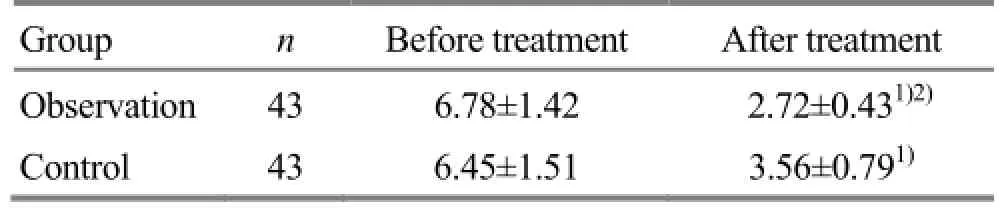
Table 2. Comparison of VAS scores between the two groups, point)
Note: Compared with the same group before treatment, 1) P<0.05; compared with the control group after treatment, 2) P<0.05
?
3.3.2 Comparison of clinical effect
After the treatment, the curative and remarkable effective rate was 74.4% in the observation group and 44.2% in the control group. The difference in the curative and remarkable effective rate was statistically significant between the two groups (P<0.01). But, the difference in the total effective rate was not statistically significant between the two groups (P>0.05), (Table 3).

Table 3. Comparison of clinical effects between the two groups
4 Discussion
In Chinese medicine, SP falls under the category of‘frozen shoulder’ or ‘shoulder of the 50-year-olds’. Its contributing factors include external contraction of wind, cold and dampness, deficiency of qi and blood due to aging, and obstructed flow of qi and blood due to chronic strain or trauma. Its main symptoms include pain and limited movement of the shoulder[3]. The treatment strategies are therefore to remove wind, dissipate cold, resolve dampness, warm meridians, circulate blood and unblock meridians.
Patients with SP due to wind, cold and dampness were selected as the research targets. The observation group was treated with the warm needling moxibustion. In the selected acupoints, Jianyu (LI 15) is the crossing acupoint of the Large Intestine Meridian of Hand Yangming and the Yang Heel Vessel, mainly used to treat pain of the shoulder and arm. Jianliao (TE 14) is used to treat heavy and painful sensation and motor impairment in the shoulder and arm. It is believed in modern anatomy that this acupoint is located in the deltoid muscle, and in the teres minor muscle, teres major muscle and tendon of latissimus dorsi muscle, and is closely related to abduction, adduction and outward rotation. Jianzhen (SI 9) is mainly used to treat scapular pain and disability to raise the arm. Jianqian (Extra), also termed Jianneiling (Extra), is located at the anterior border of the deltoid muscle, and at the midpoint of the line between the top end of the anterior axillary fold and Jianyu (LI 15), and is mainly used to treat pain in the shoulder and arm, and joint pain of the upper limb. Ashi point is mostly used for painful problems. All the above acupoints are combined to deal with the activity of the joints in all directions, accelerate blood circulation in the lesions of the shoulder, dredge the meridians of the shoulder and play a role that ‘if qi and blood flow smoothly, pain can be arrested’[4-6].
The warm needling has dual effect of acupuncture and moxibustion, with strong warming and dredging effects, to warm up the meridians, disperse cold, excite yang qi, dissipate dampness and dredge the collaterals. Simultaneously, acupuncture at the acupoints of the shoulder can produce a central analgesic effect[7], plus approximate infrared radiation of moxibustion, and has the strong penetration to transmit the temperature and energy to the diseased area sufficiently via the meridian system and play a role to treat the problem. It has been proved by studies that moxibustion can dilate the localblood vessels, increase blood flow volume, change the local microcirculation and tissue nutrition, accelerate the absorption of inflammatory exudates[8-10], so as to produce the anti-inflammatory and analgesic effect, for eliminating adhesion of the shoulder joint, and hence improving the functions of the shoulder joint quickly.
In summary, the warm needling moxibustion can combine the dual effect of acupuncture and moxibustion in the treatment of SP due to wind, cold and dampness. In view of its therapeutic effect better than singular application of acupuncture, the warm needling moxibustion is simple in operation and worthy of extensive clinical application.
Conflict of Interest
The authors declared that there was no conflict of interest in this article.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in this study.
Received: 3 March 2015/Accepted: 10 April 2015
[1] Li PH. Scapulohumeral Periarthritis. Beijing: People’s Military Medicine Press, 1995: 27.
[2] State Administration of Traditional Chinese Medicine. Criteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine. Nanjing: Nanjing University Press, 1994: 202-203.
[3] Wang CY, Fang JQ, Shi H, Li BW. Warm needling plus electroacupuncture atJian San Zhenfor s scapulohumeral periarthritis of adhesion stage in wind-cold-damp syndrome: a report of 19 cases. Zhongyi Zazhi, 2011, 52(20): 1752-1754.
[4] Qing P, Hu J. Therapeutic observation on shoulder triple-needle with warm needling plus point-toward-point at distal acupoints for periarthritis of shoulder. Shanghai Zhenjiu Zazhi, 2013, 32(10): 855-856.
[5] Cui SY, Wang SH, Xu MZ, Lai XS, Zheng SH, Zhong F. Influence of electroacupuncture at 3-shoulder acupoints combined with rehabilitation therapy on pain and movement function in poststroke shoulder-hand syndrome patients. Liaoning Zhongyiyao Daxue Xuebao, 2013, 15(11): 92-94.
[6] Fan XP, Cheng B, Huang Y, Gu K, Zong L. Immediate effects ofHeguneedling on adhesive scapulohumeral periarthritis. J Acupunct Tuina Sci, 2013, 11(4): 258-261.
[7] Zhang XL. Acupuncture Treatment of Scapulohumeral Periarthritis. Beijing: People’s Medical Publishing House, 2009: 28.
[8] Tang ZL, Song XG, Li J, Hou ZM, Xu SY. Experimental observation and analysis on anti-inflammatory and immune effect of moxibustion. Zhen Ci Yan Jiu, 1996, 21(2): 67-70.
[9] Lan L, Chang XR, Shi J, Zhang GS, Tan J. Advances of the mechanism of moxibustion. Zhonghua Zhongyiyao Xuekan, 2011, 29(12): 2616-2620.
[10] Wang JP, Yin HY, Lu SF, yang Y, Yu SG. Review of study on warm effect induced by moxibustion. Liaoning Zhongyi Zazhi, 2012, 39(4): 760-762.
Translator: Huang Guo-qi (黄国琪)
Tuina Technique and Exercise
Discussion on the theory of paying equal attention to sinew and bone in China osteosynthesis
Tang Shu-jie (唐树杰)
Department of Traditional Chinese Medicine, Medical School, Jinan University, Guangzhou 510632, China
Abstract
‘Paying equal attention to sinew and bone’ is an important principle in China osteosynthesis (CO). Traditional bone-setting manipulations not only pay high attention to fracture reduction, but also to sinew-regulating and soft tissues protection. The advantage of this principle has also been confirmed by modern medicine. To understand the principle better, it is essential to learn its historical origin, its important role in traumatology and its significant influence on modern orthopedics. In addition, we should inherit and further develop its theory, innovate and promote the development of CO constantly.
Keywords: Tuina; Massage; Bone Setting and Tuina; Traditional Chinese Medicine; Osteology and Traumatology of Traditional Chinese Medicine
【摘要】“筋骨并重”是中国接骨学的重要治疗原则。传统中医正骨手法既重视骨折复位,又重视理筋,注重软组织保护。现代医学发展证实了这一原则的先进性。为更好理解这一原则, 必须深入了解其历史渊源及其在骨伤科治疗中的作用以及对现代骨科学发展的影响。我们应继承与发展“筋骨并重”的先进理论, 走自主创新之路, 不断推动中国接骨学向前发展。
【关键词】推拿; 按摩; 正骨推拿; 中医学; 中医骨伤科学
In 1958, Professor Fang Xian-zhi and Shang Tian-yu, the famous orthopedic specialists, founded the school of China osteosynthesis (CO), i.e., the Integrated Osteosynthesis School of Traditional Chinese Medicine (TCM) and Western Medicine. CO scholars proposed the famous four principles for fracture treatment according to the clinical experiences in traumatology of traditional Chinese medicine[1], including ‘combining movement and immobilization’, ‘paying equal attention to sinew and bone’, ‘treating fracture internally and externally’and ‘cooperation between patients and physicians’. The four principles can embody the whole fracture treatment, improve the therapeutic effectiveness of fracture and significantly promote the development of orthopedics in the world. Among the principles, ‘paying equal attention to sinew and bone’, manifesting the relation between soft tissue and bone, is the key point but also a difficult point in CO. To understand this principle better, it is essential to learn its historical origin, important role in fracture treatment and significant influence on modern orthopedics.
1 Origin of Theory of Paying Equal Attention to Sinew and Bone
With thousands of years of development and improvement, the traumatology of TCM has created its specific integrated system of theory and therapeutic concept. Many ancient books on TCM, such asNei Jing(Classic of Internal Medicine) andYi Zong Jin Jian(Golden Mirror of Medicine), have described the rudiment of ‘paying equal attention to sinew and bone’. The physicians of TCM have discovered the close relation between sinew and bone in the field of anatomy, physiology, pathology and traumatology.
In the basic theory of TCM, bone belongs to‘extraordinary organs’.Nei Jing(Classic of Internal Medicine) points out that ‘bone serves as trunk’. As a firm structure, bones support body, protect internal organs and acts not only as the trunk of the body, but also the origin and insertion points of sinews. Sinews all belong to joints. Sinews are closely connected to bones. Big sinews connect to joints and dominate the movement of joints, while the small ones are attached to the tissues outside the bone. Besides, sinews restrict bones and bones support sinews. Bones and sinews coordinate to perform movement normally. It’sdescribed in details inYi Zong Jin Jian(Golden Mirror of Medicine) that sinews can restrict bones and facilitate the movements of joints; bones and sinews work together to dominate all the movements, guaranteeing the normal, powerful and free movements of human body. Once the restriction of sinews decreases, the normal movement may be affected adversely and diseases will develop. For example, some clinical studies showed that the decline of muscle strength around lumbar spine can result in lumbar instability and low back pain, while core stability exercises can increase the stability of lumbar spine and decrease the recurrence rate of low back pain[2].
Liver dominates sinews and kidney dominates bones. Liver dominates sinews, because the sinews are nurtured by liver blood. Only when there is sufficient blood in liver, can qi be transported to enrich the sinews, and only when the sinews are strong enough, can they restrict bones and facilitate the movements of joints.Nei Jing(Classic of Internal Medicine) points out that kidney engenders bones and marrows, governs bones, and stores essence; essence engenders marrows; marrow enriches bones. Sufficient kidney essence ensures the normal process of growth, development, repair and regeneration of bones. Modern medical research showed that kidney dominates bone by regulating osteoclast differentiation factors such as osteoprotegerin (OPG) and receptor activator of nuclear factor κB-ligand (RANKL)[3], and some studies demonstrated that the decoction based on liver dominating sinews can decrease the degeneration of cervical discs through the tumor necrosis factor (TNF)-α/nuclear factor (NF)-κB pathway[4]. These studies confirmed the close correlation between kidney and bone, liver and sinews.Nei Jing(Classic of Internal Medicine) holds that liver and kidney share the same origin. Kidney engenders marrows and marrow engenders liver; while liver stores blood and kidney stores essence, and blood and essence share the same origin. Therefore, liver yin and kidney yin engender and enrich each other, and kidney and liver can also influence each other both physiologically and pathologically. The normal function of sinews and bones depends intrinsically on kidney and liver. Subsequently, strong sinews lead to robust bones, and bone wilting leads to sinew wilting; kidney depletion not only induces bone wilting, but also sinew wilting; liver deficiency not only induces weak sinew, but also feeble bone. The abovementioned theories demonstrate the close relation between sinew and bone in physiology and pathology[5].
Moreover, TCM holds that sinews are connected to bones and fractures are usually accompanied by sinew injuries. Fracture can affect marrow-producing process in kidney, resulting in insufficient marrow. Subsequently, bone cannot obtain enough nutrient and the healing process slows down. Sinew injury affects the liver blood, resulting in insufficient blood in liver. Subsequently, the diseased sinew is difficult to recover because there is no enough blood in liver to enrich it. Sinew injury affects bone-restriction, resulting in nonunion and unrecovered joint function. Therefore, the TCM traumatology holds that sinew injury is closely correlated to bone injury in terms of pathological basis. Paying equal attention to sinew and bone, which has a long history and an extensive theory foundation in TCM, is one of the most important principles for fracture treatment.
2 Important Role of ‘Paying Equal Attention to Sinew and Bone’
The fracture treatment includes reduction, immobilization and functional training. The close relations between sinew and bone in anatomy, physiology and pathology determine that bone-setting is also the process of sinew-regulation. For example, dragging manipulation, the primary manipulation for bone-setting, takes full advantage of the concept that‘sinews restrict bones’. When dragging manipulation is performed, the broken ends are pressed by muscles around the bone, resulting in reduction or facilitating the reduction. ‘Paying equal attention to sinew and bone’ is involved in the whole process of fracture treatment.
The ancient TCM physicians usually paid much attention to sinew injury when they treated fractures. They created not only bone-setting manipulations, but also sinew-regulating manipulations. When bone-righting manipulations are performed, both broken ends and disturbed sinews need reducing and regulating. For example, it’s recorded inYi Zong Jin Jian(Golden Mirror of Medicine) that the manipulations for bone-setting or sinew-regulation are to deal with the injured bones or sinews to recover their normal anatomical positions. In addition,Zheng Gu Xin Fa Yao Zhi(Essential Teachings for Bone-setting) proposed eight bone-setting manipulations, in which the manipulations, Mo-feeling, Jie-setting, Duan-holding and Ti-lifting are for bone-setting; while the manipulations, An-pressing, Mo-rubbing, Tui-pushing, and Na-grasping, are for sinew-regulation, unbroken bones, or mild displacement of joints[6]. Reducing the broken bones, regulating the disturbed sinews, as well as recovering the normal anatomical position, all play an important role in preventing or treating fracture complications. For example, in treating forearm fracture, we should not only correct the abnormal position, abnormal force line of the broken ends, but also distract interosseous membrane in order to recover the normal function of forearm.
Before bone-setting, operators must get familiar with the bone landmarks, the origins and terminations ofsinews and the distributions of sinews, and understand the injury mechanism, to facilitate the reduction process and avoid further injury[7]. Moreover, the operators should know clearly of the optimal opportunity for reduction. The bone-setting is usually performed in 6 h after injury, when the swelling of sinew is less severe and no hematoma is produced inside. Six hours later, hematoma may be formed and sinews become more swelling, resulting in difficulties for manipulations[3]. During the process of bone-setting, the manipulation should be performed neither sightlessly nor rudely, but artfully and reliably, to avoid re-injury of sinews and make patients less painful. As a key process during fracture treatment, immobilization can stabilize the broken ends and avoid re-displacement. We should pay attention to the fixation of broken ends, as well as to avoid further injury of sinews.Yi Zong Jin Jian(Golden Mirror of Medicine) pointed out that ‘do not damage sinews while clamping and binding limbs or trunk’. Clamping and binding, i.e., the fixation of fracture, is a critical step to treat fracture, during which sinew injury should be avoided[1]. ‘Perform bone-setting and sinew-regulating manipulations to recover the anatomical position of bone and sinew, then pasteWan Lingplaster, immobilize the limbs with bamboo splints and bind the splints using white cloth.’ Clamping and binding limbs, assisted with plaster, medicinal powder or medicinal lotion, will reduce swelling and pain, and facilitate the union of fractures. TCM traumatology thinks highly of externally-applied medicine which includes many kinds in terms of different effects, such as activating blood and resolving stasis, relaxing sinews and activating collaterals, clearing heat and releasing toxin, engendering flesh and removing toxin. The differentiation of patients, together with local situations, determines the selection of externally-applied medicine. The extensive use of externally-applied medicine demonstrates the importance attached to sinews in TCM traumatology. In addition, splints were used extensively for fracture fixation in TCM traumatology. Splints can be adjusted according to the extent of sinew swelling, which can avoid the necrosis or re-injury of muscles resulting from excessive swelling. The ancient physicians paid much attention to sinews when they treated fractures, which is consistent with the modern doctrine that soft tissues should be protected and re-injury be prevented in treatment.
Function training is an important step to avoid anchylosis and improve the function[8]. The physicians of TCM traumatology pay high attention to the function training. After reduction of fracture, splint fixation is usually used in TCM traumatology. Splint fixation doesn’t restrict the movement of joints, but can facilitate function training. Function training in the first place is the training of sinews. After reduction and fixation, the training should be performed as early as possible. Sinews can restrict bones. Sinews training can stabilize the broken ends, keep bones and sinews in a normal anatomical position and facilitate the union of fracture. Human body is capable of maintaining stability and balance, for instance, the exercise of back extensor is helpful for the reduction of compression fracture; after the limbs fracture is immobilized using splints, the muscle force is useful in correcting the remanent displacement, increasing the pressure stress between the broken ends and promoting the growth of callus. The thought that ‘bones are connected to sinews and sinews can restrict bones’ is the important theoretical basis for ‘paying equal attention to sinew and bone’.
3 Influence of ‘Paying Equal Attention to Sinew and Bone’ on Modern Orthopedics
The CO scholars treat many fractures using manual reduction and splints fixation, improving the cure rate of fracture greatly. In addition, they provide many new theories and new therapeutic methods innovatively in the field of orthopedics after the four principles of CO were proposed in 1958. In September 1963, the 20th World Surgery Conference was held in Rome and Professor Fang Xian-zhi made a speech titled ‘Treating Forearm Fractures Using Integrated TCM and Western Medicine’, which was paid high attention by scholars from all over the world[9]; Professor Shang Tian-yu proposed a new therapeutic method for femur fracture, using splints supplemented with skeleton traction, which was adopted and written in the authoritative textbook of Fracture; professor Jin Hong-bin invented a patella-grasping instrument and achieved the gold award in the 14th World Invention Conference. The abovementioned achievements have embodied the principles of ‘combining movement and immobilization’and ‘paying equal attention to sinew and bone’, which play an important role in the development of orthopedics in China.
In recent years, the minimally invasive concept has become popular in all the fields of medicine[10-11]. The concept of minimal invasion means reducing injury and recovering function to the full extent[12]. As the norm of dealing with the relation between bone and soft tissues, the essence of ‘paying equal attention to sinew and bone’ is to minimize the injury or re-injury in diagnosis, reduction, immobilization and rehabilitation, especially to protect soft tissues from damage or re-damage[13].‘Paying equal attention to sinew and bone’demonstrates the concept of minimal invasion. Under the guidance of the principle, some treatment methods of minimal invasion, such as percutaneous reduction of fractures by leverage and external fixation instrumentation in orthopedics, have been invented and used in clinical practice, which can reduce re-injury,improve healing rate and result in good clinical outcome with lower cost.
In addition, Association for Osteosynthesis (AO) school began to support the viewpoints of biological fixation, i.e., the viewpoint of biological osteosynthesis (BO)[14], suggesting the essential condition for fracture union be the connection of viable fracture piece with primary bone instead of the stability of broken ends alone, and the circulations of local tissues be protected. In fact, BO is completely consistent with the concept of minimal invasion. The ideology of BO is to minimize the injury produced by treatment, to attach importance to the protection of local circulation; the occurrence of BO indicates that Western osteosynthesis is moving toward CO, demonstrating that Western osteosynthesis has been influenced objectively by the principles of‘combining movement and immobilization’ and ‘paying equal attention to sinew and bone’. In a way, the occurrence of BO also demonstrates the treatment principles in CO are advanced, compared with Western osteosynthesis[15].
However, advanced though the treatment concepts in CO are, the treatment methods are relatively single, demonstrating the contradiction between the advanced principles and backward methods. Therefore, we should inherit and develop the advanced principles, and take the path of independent innovation, to promote the development of CO constantly.
Conflict of Interest
The author declared that there was no conflict of interest in this article.
Acknowledgments
This work was supported by Natural Science Foundation of Guangdong Province (广东省自然科学基金项目,No. 2014A030313392).
Received: 10 March 2015/Accepted: 25 April 2015
References
[1] Lü AP, Liu MY, Zhang C, Yu WY, Lü C. The 30 years’retrospect of integration of traditional Chinese medicine and Western medicine. Zhongguo Zhongxiyi Jiehe Zazhi, 2011, 31(11): 1445-1458.
[2] Zhang YJ, Tang SJ, Chen GM, Liu YM. Chinese massage combined with core stability exercises for nonspecific low back pain: a randomized controlled trial. Complement Ther Med, 2015, 23(1): 1-6.
[3] Liu MJ, Ju DH, Zhao HY, Liu H, Wang Y, Lu HQ. Study on the mechanism of Kidney dominating bone: influence on the Zuo Gui Wan contained serum on protein expression of OPG and RANKL. Zhongguo Zhongyi Jichu Yixue Zazhi, 2009, 15(3): 184-188.
[4] Chen JJ. The interference of cervical disc degeneration on account of ‘liver dominating tendon’ decoction by pass through the TNF-a/NF-kB path. Master thesis of Nanjing university of Traditional Chinese medicine, 2013.
[5] Wang WJ. The contribution ofZheng Gu Xin Fa Yao Zhito the theory of ‘pay equal attention to sinew and bone’. China J Orthop & Trauma, 2000, 13(4): 217.
[6] Zhou Z. ‘Paying equal attention to sinew and bone’ is the soul in treating fractures. TCM Res, 2011, 24(8): 71-73.
[7] Huang F, Zheng XH, Zhou QS. Discussion of the principle of ‘paying equal attention to sinew and bone’ in fracture treatment by Chen Jichang. Zhongyiyao Xuekan, 2005, 23(4): 599-601.
[8] Lei J, Dong XJ, He MY. Treating lumbar pressure fracture using lumbar muscles exercises and Chinese herbs. Hubei Zhongyi Zazhi, 2014, 36(4): 40-41.
[9] The pioneer of China orthopedics: Fang Xian-zhi. Orthopedic J China, 2013, 21(20): 1378.
[10] Nerland US, Jakola AS, Solheim O, Weber C, Rao V, Lønne G, Solberg TK, Salvesen Ø, Carlsen SM, Nygaard ØP, Gulati S. Minimally invasive decompression versus open laminectomy for central stenosis of the lumbar spine: pragmatic comparative effectiveness study. BMJ, 2015, 350: h1603.
[11] Alsowayan O, Almodhen F, Alshammari A. Minimally invasive surgical approach to treat posterior urethral diverticulum. Urol Ann, 2015, 7(2): 273-276.
[12] Wang XS. Functional surgery, the perfect combination of minimally invasive concept and technical revolution. Weichuang Yixue, 2014, 9(6): 673-676.
[13] Jin HB. The concept of minimal invasion in ‘paying equal attention to sinew and bone’. China J Orthop & Trauma, 2003, 16(7): 385-386.
[14] Sakhvadze Sh. Biological osteosynthesis as the treatment mode for multifragmental extra-articular fractures of lower limb long bones. Georgian Med News, 2009, (168): 15-20.
[15] Duan K, Zhou JN. The development of BO and CO as well as the influence of CO on BO. Yixue Yu Zhexue, 2003, 24 (1): 56-57.
温针灸治疗肩关节周围炎的随机对照临床观察
目的:评价温针灸治疗肩关节周围炎(scapulohumeral periarthritis, SP)的临床疗效。方法:选取符合研究标准的风寒湿型SP患者86例, 随机分为观察组和对照组, 对照组施以常规针刺治疗, 观察组施以温针灸治疗。每日治疗1次, 10次为1疗程, 治疗2疗程后观察疗效和视觉模拟量表(visual analogue scale, VAS)评分变化。结果:治疗后, 两组患者VAS评分均与本组治疗前有统计学差异(P<0.05); 观察组VAS评分低于对照组, 组间差异有统计学意义(P<0.05)。观察组愈显率为74.4%, 对照组为44.2%, 两组愈显率差异有统计学意义(P<0.01)。两组总有效率差异无统计学意义(P>0.05)。结论:温针灸治疗风寒湿型SP可以综合针刺和艾灸的双重作用, 其临床疗效优于常规针刺治疗。
针灸疗法; 针刺疗法; 温针疗法; 关节周围炎; 肩痛; 随机对照临床试验
R246.2 【
】A
论中国接骨学中筋骨并重理论
R244.1 【文献标志码】A
Author: Chen Ying-chun, vice chief physician.
E-mail: chychtcm@126.com
Author: Tang Shu-jie, associate professor.
E-mail: tsj697@163.com
Methods:Eighty-six patients with SP due to wind, cold and dampness in conformity with the research criteria were randomly divided into an observation group and a control group. The control group was given the routine acupuncture treatment and the observation group was treated by warm needling. The treatment was given once every day and ten sessions made one course. After two courses, the therapeutic effects and the changes in the scores of visual analogue scale (VAS) were observed.
Results:After treatment, VAS scores were statistically different from those before treatment in the two groups (P<0.05); and VAS score was lower in the observation group than that in the control group, with a statistical difference between the two groups (P<0.05). The curative and remarkable effective rate was 74.4% in the observation group and 44.2% in the control group. The difference in the curative and remarkable effective rate was statistically significant between the two groups (P<0.01). But, the difference in the total effective rate was not statistically significant between the two groups (P>0.05).
Conclusion:The warm needling has the dual effect of acupuncture and moxibustion in the treatment of SP due to wind, cold and dampness, and its clinical effect is better than routine acupuncture treatment.
猜你喜欢
杂志排行
Journal of Acupuncture and Tuina Science的其它文章
- Electroacupuncture at Houxi (SI 3) for acute lumbar sprain: a meta-analysis of randomized controlled trials
- Clinical observation on acupuncture plus chiropractic treatment for cervical spondylosis
- Observation on clinical effect of acupuncture for cervical spondylosis of vertebral artery type
- Scalp acupuncture combined with body acupuncture for 32 cancer cases with intractable hiccups after radiochemotherapy
- Clinical effect observation on acupuncture for chronic obstructive pulmonary disease
- Clinical observation on acupuncture combined with Chinese medicine and rehabilitation training for subacute stroke patients