Electroacupuncture at Houxi (SI 3) for acute lumbar sprain: a meta-analysis of randomized controlled trials
2015-05-18WangYing王滢SunYijun孙懿君WuYaochi吴耀持ZhangJunfeng张峻峰ZhangYiyi张奕奕
Wang Ying (王滢), Sun Yi-jun (孙懿君), Wu Yao-chi (吴耀持), Zhang Jun-feng (张峻峰), Zhang Yi-yi (张奕奕)
1 Shanghai Jiao Tong University Affiliated Sixth People's Hospital, Shanghai 200233, China
2 Hongqiao Community Health Service Center, Changning District, Shanghai, Shanghai 200051, China
Systematic Review
Electroacupuncture at Houxi (SI 3) for acute lumbar sprain: a meta-analysis of randomized controlled trials
Wang Ying (王滢)1, Sun Yi-jun (孙懿君)1, Wu Yao-chi (吴耀持)1, Zhang Jun-feng (张峻峰)1, Zhang Yi-yi (张奕奕)2
1 Shanghai Jiao Tong University Affiliated Sixth People's Hospital, Shanghai 200233, China
2 Hongqiao Community Health Service Center, Changning District, Shanghai, Shanghai 200051, China
Objective:To assess the efficacy and safety of electroacupuncture (EA) at Houxi (SI 3) in treating acute lumbar sprain.
Acupuncture Therapy; Electroacupuncture; Low Back Pain; Sprain and Strains; Point, Houxi (SI 3); Meta-analysis
Acute lumbar sprain is an acute injury of the lumbar soft tissue including ligaments, muscles, or facet joints by an inappropriate lumbar activity. Clinically, it is mainly manifested by lower back pain, limited movement, stiffness and myospasm. It mainly occurs in the young and middle-aged people, though it is prevalent in any ages. Actually, acute lumbar sprain is not the terminology of traditional Chinese medicine (TCM), but according to its main clinical manifestations, it should be classified into the categories of‘Bi-impediment syndrome’ and ‘lower back pain’. As the major treatment of acute lumbar sprain, acupuncture was initially recorded inHuang Di Nei Jing(Yellow Emperor’s Classic of Internal Medicine) initially[1]. Traditional Chinese Medicine considers that lumbago due to blood stasis results from carrying a heavy load, and doctors from ancient and modern time have found that acupuncture is effective in activating blood circulation to resolve blood stasis. They have even proven that some specific acupoints can produce a remarkable therapeutic effect.
In the recent 10 years, statistical analysis of literature indicates that Houxi (SI 3) has been accepted as an essential point in treating this condition. Houxi (SI 3) comes fromLing Shu(Spiritual Pivot) and is the acupoint of the Small Intestine Meridian of Hand Taiyang and is used for body heaviness and arthralgia. Houxi (SI 3) is also one of the Eight Confluent points, connecting to the Governor Vessel, which acts to circulate qi and unblocks meridians to relieve back pain[1]. Houxi (S1 3) has a significant effect on pain along the pathways of Governor Vessel and the Taiyang Meridian. Besides, when a needle is inserted into Houxi (SI 3) towards Hegu (LI 4), it can generate an integrated effect[2]. In addition, via continuous electrical stimulation, electroacupuncture (EA) can achieve a more significant therapeutic efficacy. The basic action mechanism of electrical stimulation is to change the concentration and distribution of ions in body tissues. Abundant clinical trials have shown that low frequency pulse current can go through the filiform needle to stimulate acupuncture points, improve the pain, promote blood circulation and adjust the muscle tone[3].
This combination of modern and ancient clinical practices shows a significant clinical efficacy and safety, thus, it is widely used for acute lumbar sprain as a‘green’ treatment both at home and abroad. Although there are many relevant clinical trials about EA at Houxi (SI 3) for acute lumbar sprain in the recent 10 years, the evidence-based medical evaluation is insufficient. Therefore, this study aimed to evaluate the efficacy and safety of Houxi (SI 3) for acute lumbar sprain with meta-analysis, to provide a evidence for the further clinical study of acute lumbar sprain.
1 Materials and Methods
1.1 Inclusion criteria
1.1.1 Study characteristics
Randomized controlled trial (RCT) conducted in Chinese or English.
1.1.2 Study subjects
The patient's age and gender were not limited; all with a clear diagnosis standard.
1.1.3 Intervention
EA at Houxi (SI 3) in the trial group; while the intervention in control groups was not limited.
1.1.4 Outcome measures
Effective rate; recovery rate; infrared thermographic effect; recurrence rate; incidence of adverse events.
1.2 Exclusion criteria
Duplicate literatures were excluded.
1.3 Search strategy
Electronic retrieval was used. The databases covered the China National Knowledge Infrastructure (CNKI, 1979-2014), Chinese Biological Medical Literature Database (CBM, 1979-2014), Wanfang Digital Journal (1998-2014), and Chongqing VIP Database (CQVIP, 1989-2014). Online databases from abroad were PubMed (1966-2014), EMBASE (1980-2014), and the Cochrane Library (Issue 1, 2014). If the full text could not be obtained, a manual retrieval from the library of Shanghai Jiao Tong University was also adopted. All searches ended on July 23, 2014[4].
1.4 Evaluation method
1.4.1 Data extraction
Two independent evaluators read the abstract of each text. After removing the ineligible trials, the evaluators would read the full text of the rest to determine whether it could be finally included. They double-checked the evaluation results by exchanging with each other. Discussion would be held or the decision would be made by the third decision maker when there were disagreements on inclusion of a trial[4].
1.4.2 Quality evaluation
The study quality was evaluated according to the recommendation of Cochrane Handbook for Systematic Reviews of interventions[4]. The bias risk assessment tool included six items. Item 1: random distribution methods (selection bias); Item 2: allocation concealment (selection bias); Item 3: blinding for participants, practitioners, and outcome assessors (detection bias); Item 4: incomplete outcome data (attrition bias); item 5: selective outcome reporting data (reporting bias); Item 6: other bias. Each of the research results would be judged explicitly by these criteria by using ‘Yes’ (low risk of bias), ‘No’ (high risk of bias), or‘Unclear’ (uncertain risk of bias), which depended on the possibility of bias from low to high. By exchanging with each other, the two decision makers would double-check the evaluation results. The eligibility of the trials was assessed by discussion to resolve disagreements on inclusion or not, or the decision would be made by the third decision maker.
1.5 Data analysis[5]
A meta-analysis was performed by using Review Manager (version 5.2.0) provided by Cochrane network. The studies for inclusion were determined by inspection for heterogeneity andP<0.05 was taken as the inspection standard. The dichotomous data were summarized as relative risk (RR). The continuous data were reported as standard mean difference (SMD) or weighted mean difference (WMD). Their effect sizes were expressed as 95% confidence intervals, andP≤0.05 indicated a difference with statistical significance. Statistical heterogeneity between studies was assessed by means of Chi square and the extent of inconsistency was assessed by the I2test. When I2<40%, heterogeneity was considered as questionably important; 30%-60% was thought to possibly represent moderate heterogeneity; 50%-90% was regarded as possible substantial heterogeneity; and higher than 75% suggested a considerable level. If obvious clinical heterogeneity existed in the trials, a descriptive analysis would be performed. The stability of outcome was tested by sensitivity analysis when necessary.
2 Results
2.1 Search result
Initially, 181 trials were potentially identified in accordance with the search strategy. Then according to the inclusion criteria, 83 articles were excluded based on the titles and 98 articles were excluded by two layers with abstracts or full text. Ultimately, 6 studies including 1 288 patients were included for analysis (Table 1).

Table 1. Characteristics of the included trials
2.2 Characteristics of the included trials
2.2.1 Study characteristics
Three trials were multi-centered study[6-8], other three were single-centered study[9-11]. All the trials were randomized controlledtrials (treatment and control).
2.2.2 Study object
The participants all suffered from acute lumbar sprain which were from outpatient services and inpatient departments. All the trials used the criteria of acute lumbar sprain in theCriteria of Diagnosis and curative Effects of Diseases and Syndromes in Traditional Chinese Medicineissued by the State Administration of Traditional Chinese Medicine[12]. Only one trial did not report the inclusion and exclusion standards[10].
2.2.3 Intervention
The treatment groups were all intervened by EA at Houxi (SI 3); while three trials adopted Mobic for control[7-8,11], one trial used needling at Yaotongdian (EX-UE 7) for control[6], one trial used Diclofenac Sodium in the control group[11], and one adopted EA plus Nimesulid in the treatment group and Nimesulid alone in the control group[10].
2.2.4 Outcome measures
All the trials used the effective and cure rates as outcome measures, as well as the sources of curative standard were same, using theCriteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine[12]. Two trials used thermographic examination as one important outcome measure[8,9].
2.2.5 Methodological quality
Most trials were not of high quality (Figure 1). Among the six trials, five trials claimed the methods of randomization clearly, and all of them used random number table[6-10]; only one failed to describe how the random allocation sequences were generated legibly[9]. Allocated concealment was reported in 4 trials, such as opaque envelopes[6-8,9]. Two trials used single blinding method[6-7]. Four trials reported missed cases, but did not use the intention-to-treat analysis (ITT)[6-8,11]. Only one trial had a follow-up report. None of the papers described the baseline characteristics of the subjects in details, but only mentioned the general baseline characteristics and comparability[11](Figure 2).

Figure 1.Analysis of the risk of bias of the included trials
2.3 Effective rate
All of trials in this analysis used theCriteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicineissued by State Administration of Traditional Chinese Medicine[12]for effective rate calculation[9-11]. As illustrated in Figure 3, the results of subgroup analysis of EA at Houxi (SI 3) versus traditional acupuncture or Western medication were carried out. One trial of EA at Houxi (SI 3) plus Nimesulide versus Nimesulide [RR=1.33; 95% CI (1.19 to 1.49)] showed a beneficial treatment effect that did not cross the line of no effect[10]. Furthermore, three trials of EA at Houxi (SI 3) versus Mobic [RR=1.08; 95% CI (1.03 to 1.14)] showed a clinically significant effect that excluded clinically insignificant values[7-9]. At last, one trial of EA at Houxi (SI 3) versus point acupuncture at Yaotongdian (EX-UE 7) showed [RR=1.09; 95% CI (1.00 to 1.19)][6]and one trial of EA at Houxi (SI 3) plus tuina manipulation versus Diclofenac Sodium showed [RR=1.08; 95% CI (0.96 to 1.21)] that crossed the line of no effect, indicating clinically insignificant values[11]. Overall, there was no clear difference in the treatment effects of any of the interventions, i.e. the confidence interval overlapped.

Figure 2. Summary of the risk of bias of the included trials

Figure 3. Effective rate
2.4 Cure rate
The analysis for cure rate of EA at Houxi (SI 3) versus traditional acupuncture or Western medication was illustrated in Figure 4, and the subgroup analysis was carried out. Three trials of EA at Houxi (SI 3) versus Mobic [RR=1.67; 95% CI (1.45 to 1.92)] showed a significant beneficial treatment effect that did not cross the line of no effect[7-9]. Furthermore, one trial of EA at Houxi (SI 3) plus Nimesulide versus Nimesulide alone [RR 1.37; 95% CI (1.15 to 1.62)] showed a clinically significant effect that excluded clinically insignificant values[10]. At last, one trial of EA at Houxi (SI 3) versus point acupuncture at Yaotongdian (EX-UE 7) [RR=1.35; 95% CI ( 0.99 to 1.84)] and one trial of EA at Houxi (SI 3) plus tuina manipulation versus Diclofenac Sodium [RR=1.19; 95% CI (0.88 to 1.61)] that crossed the line of no effect, which indicated clinically insignificant values[11]. Although the model was applicable and gave stable estimates, given the arguable heterogeneity [χ2=6.14, df=5 (P=0.29), I2=19%] of the controls and of study populations, and the poor-quality of included studies, the reliability of the results is uncertain and they should be interpreted with caution.
2.5 Infrared thermographic effect
Recently, infrared thermal imaging as an important index to assess clinical therapeutic effect of acute lumbar sprain is accepted by more and more researchers. There are two studies[8,11]reported infrared thermographic effect results after treatment, and it is significantly greater with electroacupuncture than with the control [MD=2.25, 95% CI (2.20 to 2.29); two RCTs] (Figure 5). There was a significant heterogeneity between these studies (I2=87%).

Figure 4. Cure rate
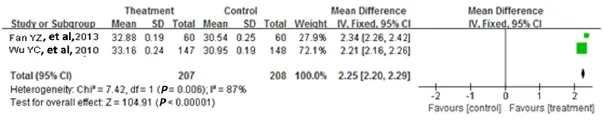
Figure 5. Infrared thermographic of acute lumbar sprain
2.6 Recurrence rate
In the two trials included in this analysis, the outcome was measured 3-6 months after treatment, and neither of them had recurrent case[6-7].
2.7 Safety assessment
Three of the studies reported adverse events[7-8,11]. There was an extremely limited amount of information reporting adverse events in the included studies. Only one of the studies reported partially about how adverse event data were collected or recorded[11]. Therefore, the study should be treated with caution (Table 2).

Table 2. Summery of Adverse events report
3 Discussion
Acute lumbar sprain is a common but refractory condition. Up to date, there are no official treatment guidelines to follow. Consequently, numerous studies have been focused on alternative therapies, because currently Western medicine does not have much to offer except anti-inflammatory analgesics. Today more and more patients turn to acupuncture, including EA. However, response varies greatly from patient to patient and different conclusions have been drawn in different clinical trials. To address inconsistency between clinical trials, provide more clinical evidence and thus set up a guideline or treatment protocol for acute lumbar sprain, we’ve conducted this systematic review and meta-analysis for the first time.
In our research, we included six randomized controlled trials, covering a total of 1 288 patients. Half of these trials[6-8]were of large samples and multi-centered, but most of them were of a low methodological quality. Although five trials mentioned their randomization methods and implementation of allocation concealment[6-10], but none of them described in details. So this might have selection bias in potential. None of the trials detailed the subject baseline characteristics, the lack of which might also conceal selection bias. In short, the low quality of the trials might lead to clinical heterogeneity and bias of the results. Caution is needed in the evaluation of these results in clinical practice.
Even though our systematic review has provided certain positive conclusions to suggest clinical practice, there still exist several limitations which may weaken the reliability of the recommendations.
First, in our research, we included six randomized controlled trials, covering a total of 1 288 patients. Half of these trials were of large samples and multi-centered[6-8], while the total numbers of RCTs and participants involved were too small to draw concrete conclusions on the therapeutic effect of EA at Houxi (SI 3).
Second, all of the included studies have some limitations, namely, the missing information of adverse effects and low methodological quality described above. Nevertheless, it cannot be avoided owing to the restriction of inherent literatures resource[13].
Third, most of the outcomes were subjective symptoms scales, which may be hard to control accurately on account of subjective feeling from the participants. So, it was important to use blinding towards the participants who received interventions. Unfortunately, owing to the regardless of blinding, it would result in high implementation bias and measurement bias.
Fourth, on account of the obvious clinical heterogeneity and considerable variation among studies, meta-analyses may be inappropriate for several important outcomes. Thus, descriptive analyses have to be conducted.
Fifth, as the included literatures were almost all from China, there was a moderate heterogeneity, e.g. the mean age and treatment source were not consistent among these studies[14].
Sixth, in spite of relatively comprehensive search strategy, incomplete retrieval of identified research cannot be avoided, together with publication bias. In summary, the results of this systematic review may be exaggerated.
In conclusion, the notion that EA at Houxi (SI 3) for acute lumbar sprain [RR=1.49; 95% CI (1.35 to 1.45)] appeared to be an efficacious auxiliary therapeutic method for acute lumbar sprain, is supported by the convictive but small amounts of data currently available, in spite of several inherent defects that the included studies had but cannot avoid. Even so, no conclusion can be drawn about their advantage over other classical also conventional treatment methods. Due to the considerable clinical heterogeneity and various outcome measures which cannot be merged by traditional statistical methods, we have on means to put forward further suggestions to guide clinical practice at present. Much more high-quality studies with adequate design and power are in need urgently, and on account of methodological limitation, much more systematic investigations in depth are also necessary to confirm the therapeutic value of EA at Houxi (SI 3) for acute lumbar sprain.
Conflict of Interest
The authors declared that there was no conflict of interest in this article.
Acknowledgments
This work was supported by Lu’s Acupuncture Inheritance Study of Shanghai Schools of Traditional Chinese Medicine (海派中医流派陆氏针灸传承研究, No. ZYSNXD-CC-HPGC-JD-004); Project of Shanghai Jiao Tong University Affiliated Sixth People's Hospital (上海市第六人民医院院级课题, 院内-1656).
Received: 5 March 2015/Accepted: 8 April 2015
[1] Li XC, Wang L. Natures of acupoint Houxi (SI 3) and its clinical application. Shanghai Zhongyiyao Zazhi, 2004, 38(5): 44-45.
[2] Yang L, Pei JC. Functions of acupoint Houxi (SI 3) and its clinical applications. Zhongyiyao Xuekan, 2004, 22(41): 726-745.
[3] Qiu ML, Zhang SC. Science of Acupuncture and Moxibustion. Shanghai: Shanghai Scientific and Technical Publishers, 1998: 173.
[4] Higgins J, Green S. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.0.1. The Cochrane Collaboration, 2008.
[5] Higgins J, Green S. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.2.0. The Cochrane Collaboration, 2008.
[6] Wu YC, Zhang BM, Wang CM. Clinical observations on the treatment of acute lumbar sprain by electroacupuncture of point Houxi. Shanghai Zhenjiu Zazhi, 2005, 24(12): 22-24.
[7] Wu YC, Zhang JF, Li SS, Zhou JH, Zhang SH, Sun YJ. Clinical effect and infrared thermogram on electroacupuncture for acute lumbar sprain. J Acupunc and Tuina Sci, 2010, 8(6): 380-383.
[8] Wu YC, Zhang BM, Wang CM, Zhang JF, Shao P, Liu GZ. Observations on the short-term and long term effects of point Houxi (SI 3) electroacupuncture on acute lumbar sprain. J Acupunct Tuina Sci, 2006, 4(6): 356-359.
[9] Zhang BM, Wu YC, Wang CM. Acupuncture at point Houxi (SI 3) for 58 cases of acute lumbar sprain. Zhongguo Linchuang Kangfu, 2003, 8(2): 321.
[10] Chen YQ. Observations on the clinical therapeutic effect of electroacupuncture at point Houxi (SI 3) combined with medication on acute lumbar sprain. Shequ Yixue Zazhi, 2010, 8(13): 39.
[11] Fan YZ, Wu YC. Clinical therapeutic effect of acupuncture combined tuina manipulation on acute lumbar sprain and infrared thermography research. Zhongyi Xuebao, 2013, 28(186): 1752-1754.
[12] State Administration of Traditional Chinese Medicine. Criteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine. Nanjing: Nanjing University Press, 1944: 201.
[13] Lu G, Ades AE. Combination of direct and indirect evidence in mixed treatment comparisons. Stat Med, 2004, 23(20): 3105-3124.
[14] Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ, 2003, 327(7414): 557-560.
电针后溪穴治疗急性腰扭伤临床随机对照试验Meta分析
目的:评价电针后溪穴治疗急性腰扭伤的疗效和安全性。方法:收集电针后溪穴治疗急性腰扭伤临床随机对照试验(Randomized controlled trial, RCT)。计算机检索PubMed (1966-2014), EMBASE (1980-2014), Cochrane Library (2014年第1期), 重庆维普数据库(1989-2014), 万方数据库 (1998-2014), 中国生物医学文献数据库 (1978-2014)和中国期刊全文数据库(1979-2014)。同时采用手工检索上海交通大学图书馆收录期刊收集相关的数据。所有收集的数据首先由两名研究者分别对每个纳入试验进行偏倚风险和质量评估, 再使用RevMan 5.2.0软件进行Meta分析。结果:共纳入6个研究, 合计1 288例患者。Meta分析结果显示电针后溪穴组在总有效率上优于尼美舒利药物组[RR=1.33; 95% CI (1.19-1.49)]和莫比可药物组[RR=1.08; 95% CI (1.03-1.14)],但与针刺腰痛点组[RR=1.09; 95% CI (1.00-1.19)]和双氯芬酸钠组[RR=1.08;95% CI (0.96-1.21)]疗效比较差异无统计学意义。而在治愈率方面, 电针后溪穴组优于莫比可组[RR=1.67; 95% CI (1.45-1.92)]和尼美舒利组[RR=1.37; 95% CI (1.15-1.62)],与针刺腰痛点组[RR=1.35; 95% CI (0.99-1.84)]和双氯芬酸钠药物组[(RR=1.19; 95% CI (0.88-1.61)]疗效差异无统计学意义。结论:截止至检索结束, 几乎没有收集到评价电针后溪穴治疗急性腰扭伤临床疗效的大样本高质量的RCT文献, 且大部分为中文文献。忽略其在临床试验中存在的固有的缺点, 电针后溪穴仍然作为一个有效且具有安全性的辅助治疗方法用于治疗急性腰扭伤, 但仍需更多的大样本RCT进行验证其在治疗急性腰扭伤的疗效。
针刺疗法; 电针; 腰痛; 扭伤和劳损; 穴, 后溪; 超分析
R246.2 【
】A
Author: Wang Ying, bachelor
Wu Yao-chi, master of medicine, professor
E-mail: nn_wang18@126.com
Methods: Randomized controlled trials (RCTs) involving EA at Houxi (SI 3) for acute lumbar sprain were retrieved from PubMed (1966-2014), EMBASE (1980-2014), Cochrane Library (Issue 1, 2014), CQVIP Database (1989-2014), Wanfang Digital Journal (1998-2014), the Chinese Biological Medical Literature Database (CBM, 1978-2014), and China National Knowledge Internet (CNKI, 1979-2014). The collection of data also adopted hand-search of the relevant journals from the Library of Shanghai Jiao Tong University. All of the data were first evaluated and extracted by two reviewers independently with a specially designed form. Then, the available data were analyzed by the Cochrane Collaboration's RevMan 5.2.0 software.
Results:A total of 6 trials involving 1 288 patients were eligible. Meta-analysis showed that the total effectiveness rate in the EA group was significantly different when compared with Nimesulide [RR=1.33; 95% CI (1.19 to 1.49)] and Mobic [RR=1.08; 95% CI (1.03 to 1.14)], but similar to that of acupuncture at Yaotongdian (EX-UE 7) [RR=71.09; 95% CI (1.00 to 1.19)] and Diclofenac Sodium [RR=1.08; (95% CI 0.96 to 1.21)]. The recovery rate in the EA group was significantly different when compared with Mobic [RR=1.67; (95% CI 1.45 to 1.92)] and Nimesulid [RR=1.37; (95% CI 1.15 to 1.62)], but similar to that of acupuncture at Yaotongdian [(RR=1.35; 95% CI 0.99 to 1.84)] and Diclofenac Sodium [(RR=1.19; 95% CI 0.88 to 1.61)].
Conclusion:Up to the search date, there are few high quality RCTs to evaluate the clinical efficacy of EA at Houxi (SI 3) for acute lumbar sprain, especially studies in English. Yet EA at Houxi (SI 3) still appeared to be an efficacious method for acute lumbar sprain, despite several inherent defects of the included studies. Further large scale trials are required to define the role of EA at Houxi (SI 3) in the treatment of this disease.
猜你喜欢
杂志排行
Journal of Acupuncture and Tuina Science的其它文章
- Clinical observation on warm needling therapy for scapulohumeral periarthritis: a randomized controlled trial
- Clinical observation on acupuncture plus chiropractic treatment for cervical spondylosis
- Observation on clinical effect of acupuncture for cervical spondylosis of vertebral artery type
- Scalp acupuncture combined with body acupuncture for 32 cancer cases with intractable hiccups after radiochemotherapy
- Clinical effect observation on acupuncture for chronic obstructive pulmonary disease
- Clinical observation on acupuncture combined with Chinese medicine and rehabilitation training for subacute stroke patients