肩胛骨恶性肿瘤保肢治疗 19 例报告
2015-05-14薛英森王臻郭征李宏国孙立国刘鑫成范宏斌
薛英森 王臻 郭征 李宏国 孙立国 刘鑫成 范宏斌
肩胛骨恶性肿瘤保肢治疗 19 例报告
薛英森 王臻 郭征 李宏国 孙立国 刘鑫成 范宏斌
【摘要】目的 评价不同治疗方式对肩胛骨恶性肿瘤患者的生存率、功能和外观的影响。方法 2001 年5 月至 2012 年 5 月,25 例累及肩胛骨的原发恶性骨肿瘤及转移瘤患者在我科接受治疗。其中男 17 例,女8 例,年龄 0.25~73 岁,平均 43 岁。25 例包括转移瘤 9 例,4 例行保肢手术;骨原发性恶性肿瘤 16 例,15 例行保肢手术。按照 Enneking 外科分期:II B 期 16 例,III 期 9 例。4 例转移瘤保肢患者中 2 例行肩胛骨部分切除,保留了肩肱关节;1 例行全肩胛骨切除后肱骨头悬吊;1 例行全肩胛骨切除后限制性全肩胛骨肩关节假体置换。15 例原发恶性肩胛骨肿瘤保肢患者中有 7 例行肩胛骨部分切除而保留了肩胛盂和肩肱关节;1 例行异体肩胛骨移植;1 例行病灶刮除、骨水泥填充;1 例行自体肩胛骨灭活回植;3 例行肩胛骨全切除和肱骨头悬吊;2 例进行了全肩胛骨的整体切除,人工限制性全肩胛骨肩关节置换术。19 例随访 6~60 个月,平均36 个月。结果 6 例死亡,其中 2 例肝癌肩胛骨转移瘤患者和 1 例血管肉瘤肩胛骨转移瘤患者死于原发肿瘤多处转移、脏器衰竭。1 例肩胛骨骨肉瘤患者死于肺转移。1 例肩胛骨滑膜肉瘤患者死于局部复发加肺转移。1 例肩胛骨骨髓瘤患者死于非原发疾病。依据美国骨肿瘤学会 ( musculoskeletal tomor society,MSTS ) ( 93 ) 对各类重建手术进行评分。1 例异体肩胛骨 18 分,1 例自体肩胛骨灭活回植 26 分,肩胛骨部分切除保留肩胛盂平均 24 分,肩胛骨全部切除肱骨头悬吊平均 21 分,人工限制性全肩胛骨全肩关节置换平均 24.7 分。肩关节前屈和后伸 90°~20°。外展范围在 40°~95°。结论 肩胛骨部分切除保留肩胛盂和人工全肩胛骨全肩关节置换可以最大限度地保留肩关节功能,对于学龄前儿童肩胛骨恶性肿瘤采用自体肩胛骨灭活后回植不失为一种可供选择的方法;无论是人工假体还是自体或异体肩胛骨可以恢复肩关节稳定性和部分功能,改善其外观。
【关键词】肩胛骨;骨肿瘤;肉瘤;肿瘤转移;人工关节;肩关节假体
尽管肩胛带 ( 肱骨近端,肩胛骨,锁骨远端 ) 是恶性骨与软组织肿瘤的第三大好发部位,但累及肩胛骨的肿瘤较少见。因此,有关肩胛骨肿瘤外科治疗及其预后的报道有限[1-4]。传统的手术方法多采用肩胛带离断根治术,近年来随着新辅助化疗的应用、外科技术的发展以及多种新型关节假体出现,传统的肩胛带离断根治术已逐渐被保肢术取代。保肢术在获得安全的肿瘤切除范围的前提下,不仅可避免患肢的外观缺陷和截肢所带来的心理创伤,而且保留或部分保留了患肢功能,因此保肢术已成为肩胛区恶性肿瘤的重要手术方式。但由于肿瘤累及的范围各有不同,手术切除与功能重建的方法选择有所差异。本研究回顾性分析了 2001 年 5 月至2012 年 5 月,我科收治的 25 例累及肩胛骨的原发恶性肿瘤或转移瘤的保肢手术方案和术后疗效。
资料与方法
一、一般资料
本组 25 例,男 17 例,女 8 例,年龄 0.25~73 岁,平均 43 岁。所有患者经 X 线、CT、MRI、骨核素扫描等影像学检查,病理学明确诊断。25 例包括转移瘤 9 例 ( 肺癌转移 5 例、肝癌转移 2 例、甲状腺癌转移 1 例、血管肉瘤转移 1 例 );骨原发性恶性肿瘤 16 例 ( 其中尤文肉瘤 7 例、骨肉瘤 2 例、软骨肉瘤 2 例、浆细胞骨髓瘤 2 例、滑膜肉瘤 1 例、恶性纤维组织细胞瘤 ( MFH ) 1 例、髓细胞肉瘤 1 例。
二、手术方法
综合考虑患者的症状、体征、影像学资料、活检病理结果来选择手术方式及重建方案 ( 表 1 )。9 例转移瘤患者,5 例活检后放弃治疗,4 例行保肢手术;16 例原发性恶性肿瘤患者,2 例活检后放弃治疗,15 例行保肢手术。按照 Enneking 外科分期[5]:II B 期 16 例,III 期 9 例。根据 Malawer 分型[6]:II 型 10 例,III 型 6 例,IV 型 3 例。4 例转移瘤保肢患者,1 例肝癌肩胛骨转移和 1 例甲状腺癌肩胛骨转移患者行肩胛骨部分切除,保留了肩肱关节。1 例血管肉瘤肩胛骨转移患者行全肩胛骨切除后肱骨头悬吊。1 例肝癌肩胛骨转移患者行全肩胛骨切除后限制性全肩胛骨肩关节假体置换。15 例肩胛骨原发恶性肿瘤患者接受了保肢手术,根据肿瘤侵及范围的大小进行了边缘切除或扩大切除,并选择了不同的重建方法,其中 7 例行肩胛骨部分切除而保留了肩胛盂和肩肱关节 ( 骨肉瘤 2 例、滑膜肉瘤 1 例、尤文肉瘤 1 例、软骨肉瘤 2 例、骨髓细胞肉瘤 1 例 );2 例肩胛骨浆细胞骨髓瘤患者,1 例行异体肩胛骨移植,1 例行病灶刮除、骨水泥填充。1 例肩胛骨尤文肉瘤患者,行自体肩胛骨灭活回植。2 例尤文肉瘤和 1 例 MFH 患者,行肩胛骨整体切除和肱骨头悬吊。2 例尤文肉瘤患者行全肩胛骨切除,人工限制性全肩胛骨肩关节置换术。术后根据肿瘤性质和切除边界的病理结果辅助以放、化疗。
三、术后随访及功能评估
本组 25 例,19 例随访 6~60 个月,平均 36 个月。功能评估采用 1993 年美国骨肿瘤学会 ( musculoskeletal tomor society,MSTS ) 功能评分系统对各类重建手术进行评分[7]。
结 果
本组获随访的 19 例中 6 例死亡,31.6%。其中 2 例肝癌肩胛骨转移和 1 例血管肉瘤肩胛骨转移患者死于原肿瘤多处转移、脏器衰竭。1 例肩胛骨骨肉瘤患者死于肺转移。1 例肩胛骨滑膜肉瘤患者死于局部复发合并肺转移。1 例肩胛骨骨髓瘤死于非原发疾病。Kaplan-Meier 曲线分析 5 年生存率为68.4% ( 图 1 )。
所有患者均能保留完整的肘部和手部功能。MSTS 93 评分显示:1 例异体肩胛骨 18 分,1 例自体肩胛骨灭活回植 26 分,肩胛骨部分切除保留肩胛盂平均 24 分,肩胛骨全部切除肱骨头悬吊平均 21 分,人工限制性全肩胛骨全肩关节置换平均 24.7 分。肩关节前屈和后伸范围 90°~20°,外展范围在 40°~95°。
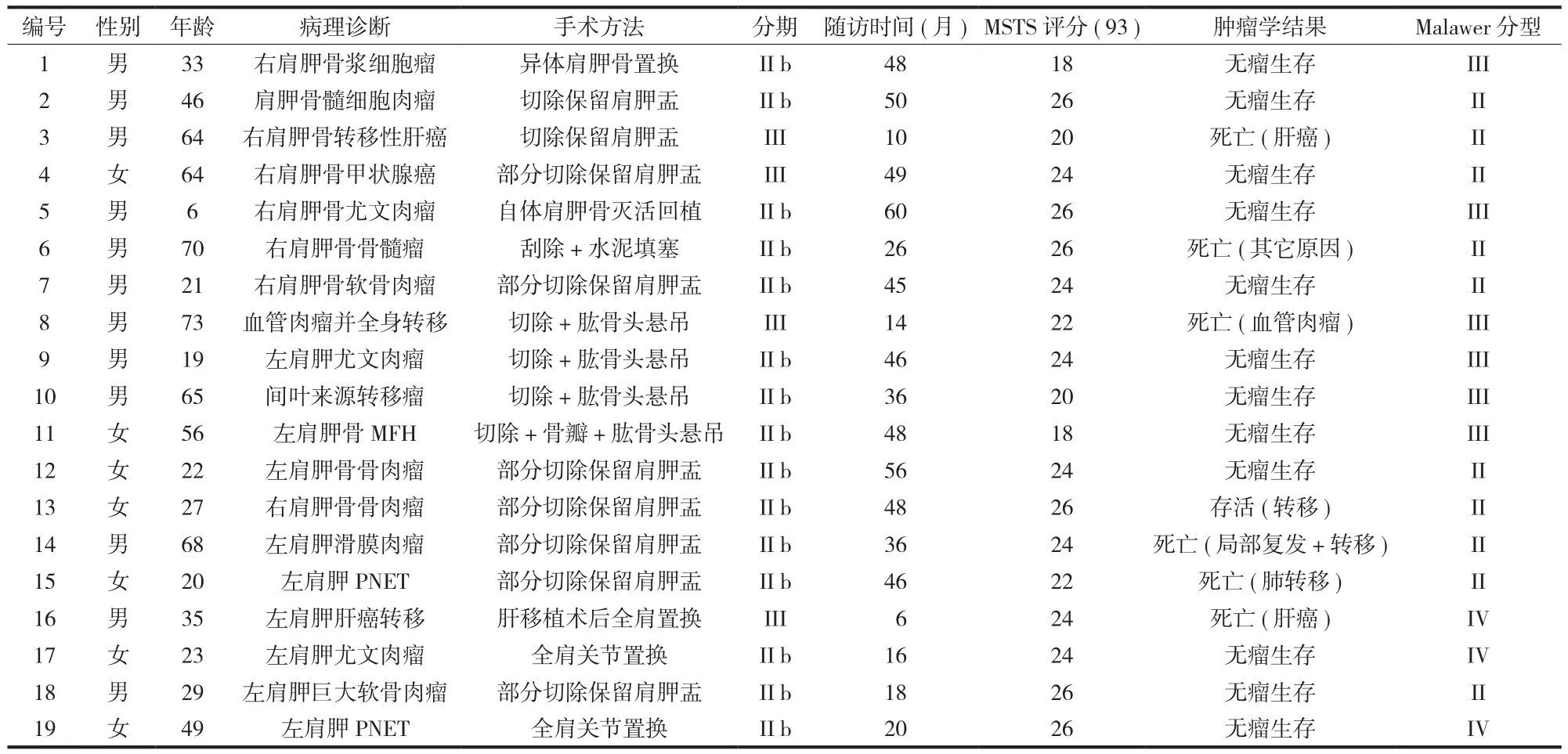
表 1 19 例接受保肢体手术肩胛骨肿瘤患者的临床资料Tab.1 Clinical data of 19 scapular tumor patients receiving limb salvage surgery

图 1 19 例接受保肢手术肩胛骨肿瘤患者的 Kaplan-Meier 生存曲线Fig.1 Kaplan-Meier estimated survival curve of 19 patients received limb salvage surgery
讨 论
一、手术方式
保肢手术的目的主要是彻底切除肿瘤,减少局部复发率,延长生命,其次是尽可能地保留肩关节,手以及肘关节功能。本组 19 例的手术选择方式主要依据 Malawer 等的分类方法:I 型,肱骨近端关节内切除;II 型,肩胛骨部分切除;III 型,关节内全肩胛骨切除;IV 型,关节外全肩胛骨和肱骨头切除;V 型,关节外肱骨近端及关节盂切除;VI 型,关节外肱骨和全肩胛骨切除。I~III 型为关节内切除,通常用来处理肩关节未受累、骨外侵犯范围小的肿瘤;IV~VI 型为关节外切除,用于肩关节受累、骨外侵犯范围广的高度恶性肿瘤[6]。
肩胛骨部分切除保留肩胛盂的术式是治疗肩胛骨肿瘤比较常用的术式 ( II 型 )。Gibbons 等[8]报道 14 例肩胛骨与软组织肿瘤接受了肩胛骨部分切除保留肩胛盂的术式,结果 14 例全部存活,其中 10 例肩关节功能得到很好的保留。Mayil Vahana 等[9]报道 23 例肩胛骨部分切除保留肩胛盂的肩胛骨肿瘤的结果,19 例存活,3 例死于肺转移,1 例死于复发和广泛转移。5 年生存率达 75.9%。术后 13 例肩关节功能均得到满意的恢复。本组 10 例II 型患者中 9 例接受了肩胛骨部分切除保留肩胛盂的术式,1 例接受了病灶刮除骨水泥填塞。术后随访 4 例死亡 ( 40%,4/10 )。9 例接受肩胛骨部分切除保留肩胛盂的患者术后 MSTS ( 93 ) 评分平均为24 分。获得了较好的功能恢复,日常生活基本不受影响。与 Mayil Vahana 等报道结果相近。
全肩胛骨切除重建术式是治疗 III 和 IV 肩胛骨肿瘤的主要手术方式。Syme 首次报道全肩胛骨切除术治疗肩胛骨恶性肿瘤,该术式的有效性已被多数学者肯定,优点是最大限度地保留了患肢的功能。Nakamura 等[10]报告 10 例肩胛骨恶性肿瘤患者肩胛骨切除的随访结果。其 5 年生存率达 50.0%,与肩胛胸壁间 1/4 肢体离断术效果相似。虽然肩关节活动严重受限,但保留了肘、腕手部的功能。重建的方式包括肱骨头悬吊、肩胛骨假体重建以及异体肩胛骨重建。Pritsch 等[11]比较了 16 例肱骨头悬吊和 16 例肩胛骨假体重建的功能和外形结果,MSTS功能评分分别为 58.5% 和 78.5%。杨强等[12]报道了5 例全肩胛骨切除重建治疗肩胛骨肿瘤,其中 1 例行肩胛骨假体置换,术后功能恢复良好 ( 77% ),相比 4 例肱骨头悬吊 ( 3 例全肩胛骨切除,1 例关节盂切除 ) 者肩关节功能评分略低 ( 65% )。本组 6 例III 型和 3 例 IV 型患者,均行全肩胛骨切除重建术,其中 4 例 III 型患者接受了全肩胛骨切除肱骨头悬吊术式;3 例 IV 型患者行限制性全肩关节置换术( 图 2,3 )。随访结果:死亡 2 例 ( 22.2%,2/9 ) 其中 1 例肝癌并肩胛骨转移于术后 6 个月死亡,1 例血管肉瘤于术后 14 个月死亡,术后功能 MSTS ( 93 )评分:4 例全肩胛骨切除肱骨头悬吊术式患者平均21 分,3 例限制性全肩关节置换术平均 24.7 分。显示限制性全肩关节置换术后功能评分略高于肱骨头悬吊术,与 Pritsch 等[11]报道结果相近,但由于本组例数较少,尚不能得出统计学差异。
随着人工假体技术发展,对于累计肩关节的肩胛骨恶性肿瘤,限制性全肩关节置换术能使患者更多获益。全肩胛骨切除或大块广泛的关节外肩胛骨切除加限制性全肩胛骨假体最大限度重建了盂肱关节和肩胛骨胸廓间的肌肉群体功能,建立了一个稳定的、无痛的肩关节,有利于肩关节的运动和上肢的稳定[2]。Wittig 等[2]报道 3 例,MSTS 功能评分 80%~90%,盂肱关节前屈和外展 25°~40°,可以旋转、后伸、外展、上抬。限制性全肩胛骨切除假体置换术是切除肩胛骨恶性肿瘤可靠的手术方案。Tang 等[13]报道了 10 例接受限制性全肩关节置换术的患者,36 个月的随访结果,显示 2 例死于原发肿瘤,1 例局部复发和远处转移。术后功能 MSTS ( 93 ) 评分:平均23.3 分。本研究中限制性全肩关节置换的术后评分与以往报道相近。

图 2 患者,女,23 岁,左肩胛骨尤文肉瘤行左肩胛骨全切限制性人工关节置换 a:术前 X 线片;b:术后 X 线片Fig.2 A 23 years women with Ewing’s Sarcoma in left Scapular received total scapulectomy with constrained scapular prosthesis a: Preoperative radiograph; b: Postoperative radiographs of replaced scapular prosthesis

图 3 术后肩关节功能评估 a:前伸;b:后伸;c:外展Fig.3 Postoperative function evaluation a: Protrusion; b: Extension; c: Abduction
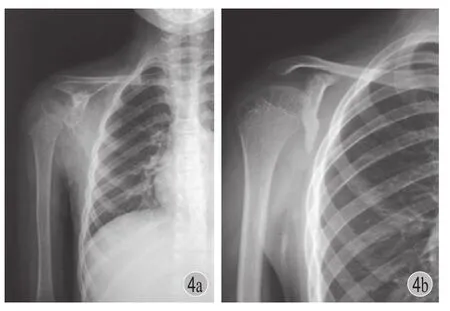
图 4 患者,男,6 岁,右肩胛骨尤文肉瘤行全肩胛骨切除灭活回植术 a:术前 X 线片;b:术后 X 线片Fig.4 A 6 years boy with Ewing’s Sarcoma in right Scapular received inactivated autogenous bone replantation surgery a: Preoperative radiograph; b: Postoperative radiographs

图 5 术后肩关节评估 a:后伸;b:外展;c:前伸Fig.5 Postoperative function evaluation a: Extension; b: Abduction; c: Protrusion
本组 1 例行自体肩胛骨灭活回植术的 6 岁肩胛骨尤文肉瘤的患儿 ( 图 4 ),由于患者尚处在骨骼发育阶段肩胛骨体积较小,找不到合适的人工假体或异体骨。采用自体肩胛骨灭活回植,灭活后的肩胛盂和肩峰基本保持完整,有利于局部肌肉附力、重建,回植后肩部外形满意。现仍无瘤存活,术后功能MSTS ( 93 ) 评分:26 分 ( 图 5 )。因此,对于学龄前儿童肩胛骨恶性肿瘤的患者,自体肩胛骨灭活回植术不失为一种可供选择的方法,但是由于本组中仅 1 例,该方法的可靠性还有赖于大样本数量的研究。
二、手术注意事项
手术切除的安全边界对于肿瘤的局部控制至关重要,根治性切除或广泛切除较边缘切除或瘤内切除的复发率低,生存期延长。因此术前必须根据症状、体征、影像学资料确定肿瘤安全边界。2008 年后,我科引入计算机导航辅助外科手术系统。术前将患者的 CT、MRI 和骨扫描的 DICOM 文件导入导航系统进行图像融合,重建出肿瘤的三维模型,可明确区分肿瘤组织、水中带和正常组织。从而对肿瘤的安全边界有了更精确定位,最大限度地保留了骨量。本组10 例采用了导航技术,术中均获得良好的安全边界,术后病理检查提示切缘均未见肿瘤细胞。
肩胛骨部分切除保留肩胛盂和人工全肩胛骨,全肩关节置换可以最大限度地保留肩关节功能,在本组病例中两者疗效无显著差异;对于学龄前儿童肩胛骨的恶性肿瘤自体肩胛骨灭活后回植,不失为一种可供选择的方法。与肩胛骨全切除后不做重建相比,无论是人工假体还是自体或异体肩胛骨均可以恢复肩关节稳定性、部分功能和改善外观。
参 考 文 献
[1] Mavrogenis AF, Mastorakos DP, Triantafyllopoulos G, et al. Total scapulectomy and constrained reverse total shoulder reconstruction for a Ewing’s sarcoma. J Surg Oncol, 2009, 100(7):611-615.
[2] Wittig JC, Bickels J, Wodajo F, et al. Constrained total scapula reconstruction after resection of a high-grade sarcoma. Clin Orthop Relat Res, 2002, (397):143-155.
[3] O’Connor MI, Sim FH, Chao EY, et al. Limb salvage for neoplasms of the shoulder girdle. Intermediate reconstructive and functional results. J Bone Joint Surg Am ,1996, 78(12): 1872-1888.
[4] Wittig JC, Bickels J, Kollender Y, et al. Palliative forequarter amputation for metastatic carcinoma to the shoulder girdle region: indications, preoperative evaluation, surgical technique, and results. J Surg Oncol, 2001, 77(2):105-114.
[5] Enneking WF, Span ier SS, Goodman MA, et al. A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop Relat Res, 1980, (153):106-120.
[6] Malawer MM. Tumors of the shoulder girdle: technique of resection and description of a surgical classification. Oflhop Clin North Am, 1991, 22(1):7-35.
[7] Enneking WF, Dunham W, Gebhardt MC, et al. A system for the functional evaluation of reconstructive reocedures after surgical treatment of tumours of the musculoskeletal system. Clin Orthop Relat Res, 1993, (286):241-246.
[8] Gibbons CLMH, Bell RS, Wunder JS, et al. Function after subtotal scapulectomy for neoplasm of bone and soft tissue. J Bone Joint Surg Br, 1998, 80(1):38-42.
[9] Mayil Vahanan N, Mohanlal P, Bose JC, et al. The functional and oncolofical results after scapulectomy for scapular tumours: 2-16-year results. Int Orthop, 2007, 31(6):83l-836.
[10] Nakamura S, Kusuzaki K, Murata H, et al. Clinical outcome of total scapulectomy in 10 patients with primary malignant bone and soft-tissue tumors. J Surg Oncol, 1999, 72(3):130-135.
[11] Pritsch T, Biekels J, Wu CC, et al. Is scapular endoprosthesis functionally superior to humeral suspension? Clin Orthop Relat Res, 2007, 456:188-195.
[12] 杨强, 李建民, 杨志平, 等. 肩胛带区骨肿瘤的保肢治疗. 中华关节外科杂志(电子版), 2010, 4(1):33-39.
[13] Tang X, Guo W, Yang R, et al. Reconstruction with constrained prosthesis after total scapulectomy. J Shoulder Elbow Surg, 2011, 20(7):1163-1169.
( 本文编辑:李贵存 )
. 肩关节外科 Shoulder surgery .
Limb salvage surgery for scapular sarcoma: a review of 19 cases
XUE Ying-sen, WANG Zhen, GUO Zheng, LI
Hong-guo, SUN Li-guo, LIU Xin-cheng, FAN Hong-bin
Department of Orthopaedic Surgery, Xi-Jing Hospital, the
fourth Military Medical University, Xi’an, Shaanxi, 710032, PRC
Corresponding author: FAN Hong-bin, Email: fanhb@fmmu.edu.cn
【Abstract】Objective To investigate functional and oncological results of different limb salvage strategies for scapular sarcoma. Methods A retrospective analysis of 25 patients diagnosed with malignant tumor of the scapula from May 2001 to May 2012 was performed. There were 17 males and 8 females and the mean age was 43 years ( range: 0.25-73 years ). Tumors include 9 metastatic tumors and 16 primary malignant tumors. Nineteen patients received limb salvage surgery ( 4 metastatic tumors, 15 primary malignant tumors ). According to Enneking surgical staging: II B 16 cases, stage III 9 cases. In 4 metastases cases of limb salvage, 2 cases received partial resection of the scapula and the scapulohumeral joint was preserved, 1 case received humeral head suspension after complete scapula resection, 1 case received constrained shoulder prosthesis after complete scapula resection. In 15 primary malignant tumors cases of scapula limb salvage, 7 cases received partial resection of the scapula and the glenoid and scapulohumeral joint were preserved, 1 case received scapula allogeneic transplantation, 1 case received lesion curettage and bone cement filling, 1 case received inactivated autologous scapula replantation, 3 cases received humeral head suspension after complete scapula resection, 2 cases received constrained shoulder prosthesis after complete scapula resection. 19 cases were followed up with the mean period of 36 months ( range: 6-60 months ). Results In 6 dead cases, 2 cases of scapula metastases in liver tumors and 1 case of scapula metastases in angiosarcoma died of primary tumors metastases and organ failure, 1 case with osteosarcoma died of lung metastases, 1 case with scapula synovial sarcoma died of local recurrence plus lung metastases, 1 case with scapula myeloma died of non primary disease. Accordingbook=535,ebook=28to MSTS ( 93 ) scored for the various types of reconstructive surgery. One case of allogeneic scapula got 18 points, 1 case of inactivated autologous replantation got 26 points, cases of scapula partial resection and glenoid preservation got 24 points on average, cases of scapula total removal and the humeral head suspension got 21 points on average, cases of constrained shoulder prosthesis after complete scapula resection got 24.7 points on average. Shoulder flexion and extension were in the range of the 90°to 20°. Outreach range was of 40° to 95°. Conclusions Partial scapulectomy with the preservation of glenoid, and total scapulectomy with constrained scapular prosthesis both can preserve the shoulder functions to the greatest degree. Inactivated autologous replantation can be regarded as an alternative for preschool children with scapula malignant tumors. Prosthesis, autologous or allogeneic scapula can restore stability, functions, and improve appearance.
【Key words】Scapula; Bone neoplasms; Sarcoma; Neoplasm metastasis; Joint prosthesis; Prosthesis
( 收稿日期:2015-04-28 )
通信作者:范宏斌,Email: fanhb@fmmu.edu.cn
DOI:10.3969/j.issn.2095-252X.2015.07.007
作者单位:710032 西安,第四军医大学西京医院骨科
中图分类号:R738.1