复杂肱骨远端骨折手术治疗的临床探讨
2014-07-05赵龙宋有鑫崔成喜张宇轩张宝琦龚平武云鹤尚瑞松陈宾
赵龙 宋有鑫 崔成喜 张宇轩 张宝琦 龚平 武云鹤 尚瑞松 陈宾
复杂肱骨远端骨折手术治疗的临床探讨
赵龙 宋有鑫 崔成喜 张宇轩 张宝琦 龚平 武云鹤 尚瑞松 陈宾
目的评价手术治疗复杂肱骨远端骨折的疗效。方法我院自2004年1月至2013年12月治疗肱骨远端骨折患者24例(AO/OTA分型为A3、B1、B2、C3型),根据不同的骨折分型采取个性化治疗,并对手术时间、术中出血量及术后肘关节功能进行评价。结果术后随访3~6个月,平均4.5个月。根据肘关节返修术后功能评价(Mayo Clinic),术后一周肘关节功能评分:良好12例,一般10例,较差2例,优良率为50.0%;术后3个月肘关节功能评分:良好15例,一般7例,较差2例,优良率为62.5%。AO/OTA分型:A3型平均手术时间(186±45.9)min,平均术中出血量(161.1±69.7)ml,平均引流量(109.4±39.2)ml;B1、B2型平均手术时间(115±42.9)min,平均术中出血量(75.8±66.5)ml;平均引流量(17.0±28.2)ml;C3型平均手术时间(206.7±37.4)min,平均术中出血量(237.8±140.4)ml,平均引流量(132.8±17.9)ml。结论合理的手术入路及内固定方式结合早期功能锻炼有利于肱骨远端骨折患者术后肘关节功能的恢复,可提高肱骨远端骨折患者的治疗效果,减少并发症。
肱骨骨折,远端;手术治疗;疗效
肱骨远端骨折是肘关节周围的一种严重损伤,约占成人骨折的2%,占肱骨骨折的50%,多见于青壮年,是临床上较难处理的骨折之一[1]。由于肱骨远端骨折类型复杂,多为粉碎性骨折且复位困难,因此术后易发生骨折再移位和关节黏连,是当今公认的创伤骨科难题之一。现总结我院2004年1月至2013年12月收治的24例肱骨远端骨折患者(AO/OTA分型为 A3、B1、B2、C3型)的临床表现、治疗方法及效果,报道如下:
资料和方法
一、一般资料
选择我院自2004年1月至2013年12月收治的24例肱骨远端骨折患者,其中,男性15例,女性9例,年龄17~73岁,平均41岁。按AO/OTA分型:A3型9例,B1、B2型6例,C3型9例。术前伤肢合并神经损伤患者2例,合并糖尿病、高血压等全身性系统疾病的患者2例。
二、手术方法
患者入院后以长臂石膏托固定,完善相关术前检查,均于入院后12~72h手术,平均1.5d。臂丛神经阻滞麻醉(22例)或全麻(2例)成功后,患者均取侧卧位,患肢置于胸前,常规消毒术区后手术。部分患者术中使用气囊止血带。
A3型肱骨远端骨折患者9例、B1、B2型骨折6例、C3型骨折7例,选择经纵行分离三头肌入路。肘部后正中切口长约15cm,依次切开皮肤、皮下组织、深筋膜,显露肱三头肌后,在肱骨远端钝性分离肱三头肌远端并向内、外侧牵开,显露骨折端。直视下解剖复位骨折,用2枚克氏针横行临时固定骨折端,注意保持肱骨干的提携角和肱骨髁的前倾角。然后以外侧单钢板或双钢板固定骨折端。术中用C臂X线机透视,确定骨折复位满意、内固定牢固后拔除临时固定骨块的克氏针,彻底冲洗切口,放置引流管,逐层缝合。
部分C3型肱骨远端骨折(2例),采用肘后经尺骨鹰嘴截骨入路或纵行分离肱三头肌入路。选择肘后S形切口,起于肱骨中下1/3,止于尺骨干,长约15cm。暴露肱三头肌内侧缘的尺神经,充分游离后牵引保护,沿肱三头肌肌腱两侧分离,远端至尺骨近端,从内侧或外侧剥离鹰嘴后侧骨面,先用摆锯在鹰嘴尖、肱三头肌肌腱附着点近端的关节外缘作V形截骨,深度为尺骨鹰嘴的3/4,然后用骨凿截至软骨下骨,撬拨截断鹰嘴,截断的鹰嘴连同肱三头肌肌腱一同翻向近端,充分暴露肱骨内、外髁及滑车部关节面。复位髁间骨折,将髁间骨折变为髁上骨折,骨折复位满意后屈曲肘关节,将骨折远端与近端复位,并用2~4枚克氏针临时固定。取2块AO解剖型锁定加压板,分别植于干骺端的外侧柱和内侧柱的骨嵴上,注意保护血运,不剥离骨表面软组织。然后垂直钢板方向植入螺钉,并保证螺钉不进入鹰嘴窝或冠状窝。或术中使用单钢板辅助克氏针固定骨折端。术中采用C臂X线机透视确定骨折复位满意、内固定牢固。移除克氏针,活动肘关节,确定固定牢靠后,将截下的鹰嘴骨块复位,打入平行的双克氏针,“8”字张力带钢丝固定,探查尺神经,放置引流管,缝合伤口。
三、术中注意事项
术中操作轻柔,注意神经、血管的保护。易疆莺等[2]认为在骨折复位过程中应注意恢复上肢提携角及肱骨髁的前倾角。对于C3型骨折术中应先恢复髁间骨折,变髁间骨折为肱骨髁上骨折,之后复位肱骨远端内外侧柱,重点是恢复肱骨滑车关节面。在手术操作时注意保护骨折块的血供及神经。
四、术后处理
术后患者常规应用抗生素3~5d。术后48~72h内拔除引流管,2周后拆线。根据骨折的分型和患者实际情况辅助上肢长石膏拖或可拆卸式肘关节支具功能位固定。术后早期即进行功能锻炼,进行上肢肌肉的等长收缩及肩、腕、各手指关节等的功能锻炼。术后一周左右鼓励患者主动进行肘关节屈伸活动,以主动活动为主、被动锻炼为辅。由于A3及C3型骨折属粉碎性骨折,因此锻炼结束后继续石膏拖或支具外固定。有文献报道:肘关节功能锻炼应逐渐增加锻炼幅度,6~8周后允许上肢适当负重[3]。有2例患者因骨折粉碎严重、内固定不牢固,术后石膏托固定3周后行肘关节功能锻炼。
结 果
24例患者均顺利完成手术,手术时间55~270min(平均143min),术中出血量为50~400ml(平均183ml),见表1。24例患者切口均I期愈合,未出现切口红肿、渗液、感染。术后随访3~6个月(平均4.5个月),骨折端可见明显骨痂形成。随访期间无内固定松动、骨化性肌炎、骨折畸形愈合、延迟愈合或不愈合的发生。按照肘关节返修术后功能评价(Mayo Clinic):术后1周:优良率为50.0%;术后3个月:优良率为62.5%,见表2。
表1 三种类型手术时间、术中出血量和术后引流量数据分析(ml,±s)
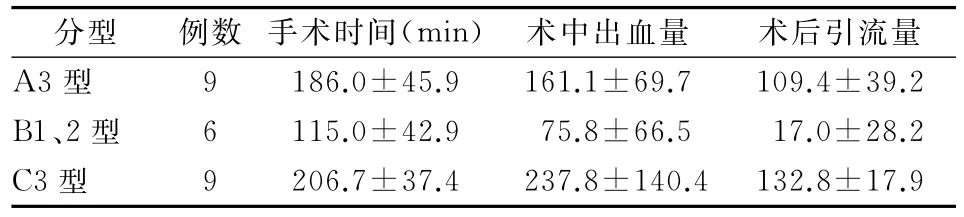
表1 三种类型手术时间、术中出血量和术后引流量数据分析(ml,±s)
分型 例数 手术时间(min) 术中出血量 术后引流量A3 型 9 186.0±45.9 161.1±69.7 109.4±39.2 B1、2 型 6 115.0±42.9 75.8±66.5 17.0±28.2 C3 型 9 206.7±37.4 237.8±140.4 132.8±17.9

表2 肘关节返修术后功能评价(Mayo Clinic)(例)
讨 论
一、肱骨远端骨折的AO/OTA分型
肱骨远端骨折目前常用的AO/OTA分型分为:A型骨折为关节外骨折;B型骨折为部分关节内骨折;C型骨折为完全关节内骨折,即髁间骨折。近年来有学者提出肱骨远端的“双柱”概念[4],即肱骨远端的冠状三角,三角中央为冠状窝及鹰嘴窝,内外髁由近端向远端延伸构成双柱。在肱骨远端冠状三角结构中,任何一边断裂都会破坏肱骨远端力学的稳定性。肱骨远端A型骨折中双柱断裂,而肱骨远端C型骨折中冠状三角三边均遭到破坏,手术重点是恢复三边的稳定性[5]。因此在肱骨远端骨折的处理中,应同时恢复肱骨远端关节面和内外侧双柱的完整性。在AO/OTA分型中C3型骨折为关节内粉碎性骨折(包括肱骨滑车及双柱均为粉碎性骨折),术中骨折复位及内固定实施都较为困难,导致肘关节功能恢复较差。Charissoux等[6]进行流行病学调查研究发现,由于中老年患者骨质疏松,肱骨远端骨折多为C型。
骨折分型决定了手术方式的选择[7],因此术前评估十分重要。CT扫描及三维重建可更好反映骨折的移位情况,尤其是肱骨远端C型骨折,可指导临床医师进一步治疗,在患者手术方式的选择中发挥了重要作用。
二、肱骨远端骨折手术入路的选择
治疗肱骨远端骨折目前国内外文献报道的常用手术入路主要有:(1)肱三头肌舌形瓣入路;(2)经肱三头肌内外侧联合入路;(3)尺骨鹰嘴截骨入路。在本研究中有2例患者采用肱三头肌舌瓣入路,虽然未用鹰嘴截骨,但仍对肱三头肌的损伤较大。该术式早期可造成术后肌肉水肿,同时进行肘关节制动,不利于肘关节早期功能锻炼。远期可造成肌肉萎缩、黏连和瘢痕愈合等,而影响肘关节功能。并且该入路对肱骨远端关节面及肘前方显露较差,目前临床已较少使用,尤其是在肱骨远端C型骨折手术中。
本研究中的21例患者选择纵行劈开肱三头肌或经肱三头肌一侧入路。该术式对于除肱骨滑车外的肱骨远端骨折端暴露较为理想。该术式保留了肱三头肌的连续性,避免了肱三头肌舌形瓣入路的一些并发症。有利于早期进行肘关节功能锻炼,防止关节僵硬。同时,该术式在最大程度上减少肘关节周围肌肉及关节囊的损伤,保留了骨折块的血运,防止肘关节黏连、关节囊挛缩及骨折块缺血坏死。然而,对于复杂的肱骨远端C3型骨折具有一定的局限性,该入路不能充分暴露肱骨滑车粉碎性骨折块。
另外1例患者通过鹰嘴截骨充分暴露肱骨远端骨折端,尤其是肱骨滑车的显露。该术式避免了肱三头肌的损伤,有利于对粉碎性骨折解剖复位。与肱三头肌舌形瓣入路相比,经鹰嘴截骨入路对骨折暴露、复位更容易[8]。然而,人为的造成鹰嘴骨折,术后可能出现创伤性关节炎、异位骨化、骨不愈合等并发症,影响肘关节功能的恢复。但只要鹰嘴截骨做到解剖复位、坚强内固定、早期功能锻炼,仍能取得满意的疗效[8]。采用鹰嘴基底部“V”形截骨,可简化骨折复位及增加截骨的接触面积,有利于截骨面的骨性愈合,减少并发症。该术式保护了肱三头肌,避免其在肱骨远端的黏连,有利于术后肘关节功能恢复。鹰嘴截骨入路较其他手术入路对骨折端的暴露更充分,有利于粉碎性骨折的直视下复位和固定,并且不影响肘关节的早期功能锻炼。但不足之处是人为地造成一次骨折,不易被患者接受。
手术入路的选择明显影响术后肘关节功能恢复[9]。因此根据骨折情况选择入路方式,对于AO/OTA分型中A、B、C1及C2型骨折,肱骨滑车关节面相对完整者,可采用纵行劈开肱三头肌或肱三头肌内外侧入路。对于C3型骨折,因术中需要对肱骨滑车粉碎性关节面进行复位,以及肌肉发达、肥胖等骨折暴露困难者,应选用尺骨鹰嘴截骨入路。
王静等[8]研究发现:肱骨髁间骨折C2及C3型患者尺骨鹰嘴截骨入路内固定术后肘关节功能评分的优良率(82.32%与79.38%)均高于肱三头肌两侧入路术后肘关节功能评分的优良率(70.59%与64.71%);C1型患者两种入路术后肘关节功能评分的优良率差异无统计学意义。目前肱骨髁间骨折首选切开复位内固定术,常用入路为鹰嘴截骨入路[10]。Ahern等[11]通过动物实验证明鹰嘴截骨入路可以更好地暴露骨折端,尤其是复杂的肱骨远端骨折。
三、肱骨远端骨折内固定方式的选择
骨折治疗过程中坚强内固定是保证术后早期进行功能锻炼和获得良好疗效的前提。以往的单钢板、Y形钢板、克氏针、克氏针张力带等内固定方法疗效较差。克氏针由于稳定性差,易出现松动、退针,术后常需要较长时间的石膏外固定,影响术后早期功能锻炼。而单钢板为平面固定,不符合“双柱”概念的生物力学要求,对于粉碎性的C3型骨折远端固定有限。“Y”形钢板采用分叉角度固定,置于肘关节后方与肱骨远端的贴附差,对肱骨远端的C型骨折关节面的恢复和固定强度有限。“Y”型钢板如果放置过低有可能进入鹰嘴窝,影响肘关节伸直。
由AO组织推荐的垂直双钢板技术和由O′Driscoll[12]推荐的平行双钢板技术可提供坚强的内固定,早期进行肘关节功能锻炼。该方法符合近年来国内外学者提出的“双柱固定”理念。此外,肱骨远端骨折恢复滑车关节面是整个肱骨远端骨折复位的关键,也是术后关节功能恢复的重要前提[5]。在恢复髁间骨折稳定性后,采用垂直或平行双钢板固定肱骨远端的内外侧柱,在解剖复位的基础上提供坚强的内固定。Kaiser等[13]采用垂直双钢板治疗22例肱骨远端骨折,垂直双钢板可提供最大的强度和抗疲劳特性,术后功能理想。Xie等[14]研究证实,内外侧双钢板固定治疗肱骨远端关节内骨折效果满意。Theivendran等[15]对16例肱骨远端骨折患者运用平行双钢板治疗,可达到较好的功能要求。Self等[16]通过生物力学试验表明,双钢板固定在肘关节活动时牢固性最佳。Schemitsch等[17]研究认为内外双接骨板法是最佳的生物力学固定模式。双钢板固定有助于重建双柱结构,固定牢固、稳定,适用于C型骨折。
近年随着手术器械及内固定器械的不断发展,肱骨远端骨折内固定方法越来越科学。由最早的重建钢板逐渐出现了解剖钢板和锁定钢板。解剖钢板利于骨折的复位,并且可为骨折复位提供一定的参考。而锁定钢板由于其内支架作用,在治疗严重粉碎性骨折及老年骨质疏松患者具有一定的优势。因此,AO双钢板固定中出现了肱骨远端解剖锁定钢板[18]。相关临床研究报道了应用肱骨远端解剖锁定钢板治疗肱骨远端骨折的满意效果[13]。由于其价格高昂,应用较为有限。对于高龄、骨质疏松严重、严重粉碎的髁间骨折患者,全肘关节置换术可作为一种有效的治疗方法[10]。切开复位内固定术和全肘关节置换术在治疗肱骨远端骨折C型骨折中远期疗效、并发症、再手术率没有统计学差异[19]。也有研究报道对于肱骨远端骨折选择过关节外固定架治疗,尤其对开放肱骨远端骨折有一定的疗效[20]。
本研究中13例采用单钢板固定,4例采用双钢板固定,7例采用双空心螺钉及克氏针固定。在早期功能锻炼中采用双钢板固定者,开始肘关节功能锻炼时间明显早于其他内固定方式,并且术后肘关节功能恢复明显优于其他方式。
四、肱骨远端骨折手术时机选择、并发症及预防
肱骨远端骨折由于骨折复杂,解剖复位困难,术后并发症多,是当今公认的创伤骨科治疗难题之一。手术时机的选择对骨折复位及肘关节功能的恢复非常重要。本文所涉及病例均于入院后12~72h手术,平均1.5d,骨折早期行切开复位内固定,软组织易分离。对于软组织张力较高的患者采用减张缝合,均获得了较好的疗效。闭合性骨折一般在伤后24~72h肿胀不显著时手术最好,术前时间过长可增加术中骨折复位的难度,使得复位不理想,影响肘关节术后功能的恢复。黄雷等[21]认为伤后超过1周再手术的患者,优良率明显下降。因此,手术时机的把握可明显降低术后并发症。
肱骨远端骨折常见的并发症有关节挛缩、黏连、创伤性关节炎、异位骨化、尺神经炎、骨折不愈合或畸形愈合等。根据骨折类型及软组织损伤程度,选择合理的手术入路、内固定方式,重建关节面才能保证关节功能的恢复,减少创伤性关节炎的发生[22]。术中操作仔细、轻柔,减小(轻或少)术中医源性损伤。术后早期进行正确的功能锻炼是肘关节功能恢复的关键[10]。本研究鼓励患者早期进行主动肘关节屈伸功能锻炼,4例垂直双钢板固定的患者术后早期进行功能锻炼,肘关节恢复良好,选择单钢板固定的5例患者术后进行功能锻炼较晚,肘关节功能恢复一般。对于单纯克氏针及螺钉固定的患者,术后辅助石膏托外固定,术后肘关节功能恢复欠佳。因此坚强内固定是肘关节早期进行功能锻炼的基础,可有效预防肘关节周围软组织黏连。有学者报道[23]术后当天即开始服用非甾体类药物,抑制炎性反应,同时能抑制间充质干细胞的迁移和增殖,阻断向成骨细胞分化,防止局限性骨化性肌炎形成。
我们主张患者术后早期进行上肢肌肉主动收缩及肩、腕、各手指关节功能锻炼。指导患者循序渐进地进行肘关节功能锻炼,主动活动结合被动活动,同时锻炼前臂旋转功能,使功能锻炼合理有效[21]。对于术后肘关节屈伸功能不佳者,也可配合外固定架松解肘关节。因此,早期合理的功能锻炼可有效防止肘关节术后并发症的发生,促进骨折愈合及肘关节功能的恢复。
综上所述,对于肱骨远端骨折利用影像学资料进行骨折分型,早期选择合适的手术方式治疗。在满意的骨折复位和坚强的内固定前提下,术后早期进行功能锻炼,对肘关节功能恢复具有重要意义。
[1] 芦浩.姜保国,付中国,等.肱骨近端骨折合并肱骨髁间骨折一例[J].中华肩肘外科电子杂志,2013,1(1):48-49.
[2] 易疆莺,李浩,邹远云,等.复杂肱骨远端骨折的双钢板内固定治疗[J].华西医学,2010(12):2249-2251.
[3] Pollock JW,Athwal GS,Steinmann SP.Surgical exposures for distal humerus fractures:a review[J].Clin Anat,2008,21(8):757-768.
[4] Ring D,Jupiter JB.Fractures of the distal humerus[J].Orthop Clin North Am,2000,31(1):103-113.
[5] 范存义,姜佩珠,蔡培华,等.双柱理论在骨质疏松性C型肱骨远端骨折治疗中的应用[J].中华创伤骨科杂志,2007,9(3):221-224.
[6] Charissoux JL, Vergnenegre G, Pelissier M, et al.Epidemiology of distal humerus fractures in the elderly[J].Orthop Traumatol Surg Res,2013,99(7):765-769.
[7] Bégué T.Articular fractures of the distal humerus[J].Orthop Traumatol Surg Res,2014,100(1Suppl):S55-S63.
[8] 王静,姜保国,张培训.尺骨鹰嘴截骨与肱三头肌两侧入路内固定治疗肱骨髁间骨折的疗效比较[J].中华骨科杂志,2009,29(3):235-240.
[9] 姜保国,张殿英,付中国.切开复位内固定治疗肱骨髁间骨折的疗效分析[J].中华创伤杂志,2007,23(2):97-99.
[10] 罗伟,姜保国.肱骨髁间骨折的治疗进展[J].中华外科杂志,2009,47(12):903-905.
[11] Ahern BJ,Richardson DW.Distal humeral Salter Harris(Type II)fracture repair by an ulnar osteotomy approach in a horse[J].Vet Surg,2010,39(6):729-732.
[12] O′Driscoll SW.Optimizing stability in distal humeral fracture fixation[J].J Shoulder Elbow Surg,2005,14(1):186S-194S.
[13] Kaiser T,Brunner A,Hohendorff B,et al.Treatment of supra-and intra-articular fractures of the distal humerus with the LCP Distal Humerus Plate:a 2-year follow-up[J].J Shoulder Elbow Surg,2011,20(2):206-212.
[14] Xie X,Qin H,Shen L,et al.Open reduction and bicolumnar internal fixation of intra-articular distal humerus fractures through a combined medial and lateral approach[J],2013.[in print]
[15] Theivendran K, Duggan PJ, Deshmukh SC.Surgical treatment of complex distal humeral fractures:functional outcome after internal fixation using precontoured anatomic plates[J].J Shoulder Elbow Surg,2010,19(4):524-532.
[16] Self J,Viegas SF,Buford WL,et al.A comparison of double-plate fixation methods for complex distal humerus fractures[J].J Shoulder Elbow Surg,1995,4(1Pt 1):10-16.
[17] Schemitsch EH,Tencer AF,Henley MB.Biomechanical evaluation of methods of internal fixation of the distal humerus[J].J Orthop Trauma,1994,8(6):468-475.
[18] 杨明辉,李庭,蒋协远.肱骨髁间骨折的内固定选择[J].中华关节外科杂志:电子版,2011,5(3):364-368.
[19] Wang Y,Zhuo Q,Tang P,et al.Surgical interventions for treating distal humeral fractures in adults[Z],2013:CD009890.
[20] Lewandowski L,Tintle SM,Daniel C,et al.Circular external fixation for treatment of distal humerus fractures:case report[J].J Hand Surg Am,2013,38(6):1155-1160.
[21] 黄雷,张波,王满宜,等.肱骨髁间骨折的手术治疗[J].中华骨科杂志,2001,21(3):158-162.
[22] Throckmorton TW,Zarkadas PC,Steinmann SP.Distal humerus fractures[J].Hand Clin,2007,23(4):457-469.
[23] 王慧勇,陈本钰,王希鹏.31例肱骨远端关节内骨折患者的手术治疗效果分析[J].中国当代医药,2011,4(8):158.
Clinical evaluation of operative treatment of complicated distal humerus fractures
Zhao Long,Song Youxin,Cui Chengxi,Zhang Yuxuan,Zhang Baoqi,Gong Ping,Wu Yunhe,Shang Ruisong,Chen Bin.Sixth Department of Orthopaedics,Affiliated Hospital of Chengde Medical College,Chengde 067000,China
BackgroundDistal humeral fracture is a severe damage around the elbow joint,and is often seen in young adults.It accounts for 2%of all adult fractures and about 50%of all humerus fractures.It′s one of the fractures that is difficult to deal with.The types of distal humeral fracture are divergent.Distal humerus fractures are often comminuted which make operative reduction difficult.Secondary loss of reduction and elbow ankylosis are common postoperative complications.All these difficulties make the distal humerus fracture one of the unresolved problems in fracture treatment.This study is to evaluate the clinical outcome of complex distal humeral fractures treated by operation.Methods(1)General data:twenty-four cases of operative treated distal humerus fractures in author′s hospital from January 2004to December 2013were included in this study.There were 15 males and 9females,aging from 17to 73,averaged 41.AO/OTA Classification:A3:9cases;B1,B2:6cases;C3:9cases.Two cases were combined with nerve injury.Two cases had histories of high blood pressure and diabetes.(2)Operative method:The patient was placed in the supine position,and the elbow to be operated on was positioned at 90°of abduction and supported on a lucent operating table.A pneumatic tourniquet was placed as proximally as possible on the arm.With the elbow flexed at about 60°,the first incision was made about 7cm proximal to the tip of the medial epicondyle.In the initial cases,the ulnar nerve was isolated,released from the ulnar nerve groove,and protected carefully.In later cases,the nerve was only exposed.The medial and anteromedial side of the distal humerus was exposed through the opening between the brachial muscle and the medial intermuscularseptum.The common origin of the flexor muscles was partially dissected and reflected distally,leaving a 5-mm strut to be re-sutured in situ at completion of surgery.The anterior capsule was incised.The articular surface of the trochlea was then exposed.A second incision was begun approximately 8 cm proximal to the lateral epicondyle.The space between the triceps posteriorly,the origins of the extensor carpi radialis longus and the brachioradialis anteriorly,and the anterior side of the distal articular surface were exposed.The space between the anconeus and the extensor carpi ulnaris was opened,and the most distal articular surface of the capitulum and the lateral part of the trochlea was exposed.The elbow was then flexed about 80°,and the biceps and brachial–bronchial muscles were retracted anteriorly.Any hematoma among the fragments was debrided,and the number and displacement of articular fragments were identified.The main medial articular fragment,usually associated with the metaphyseal fragment,was first reduced to the medial column and temporally fixed with K-wires.Definitive fixation with a reconstruction plate (usually 6holes)could be completed if the metaphyseal fragment was anatomically reduced.Displaced small articular fragments were reduced to the main lateral fragment and fixed with 0.8K-wires.The main lateral articular fragment was then reduced medially to the medial articular fragment and proximally to the lateral column and maintained temporarily with K-wires.The reduction in the articular surfaces was then checked under direct vision and using a C-arm.Any step or gap between the lateral and the medial articular fragment was abolished by abduction or adduction of the elbow and compression with forceps while keeping the medial fragment in situ.Simultaneous adjustment of the lateral column was also performed.If the articular fracture was anatomically reduced,a 1.25-mm guide wire was then inserted into the trochlea from the lateral condyle,passed through the fracture and then to the medial condyle,parallel with the distal articular surface and located in the bone between the olecranal fossa and the articular surface as confirmed by C-arm.A 4.0-mm cannulated screw was then inserted along the guide wire.As described above,the medial column could be definitely fixed with a plate if anatomical reduction was achieved.In most cases,the plate was positioned on the anteromedial side of the distal humerus.The distal end of the plate should not extend beyond the medial epicondyle and should be fixed to the bone with 2-3screws according to the location of the fracture line.The best option was to insert the most distal two screws into the medial trochlea.If the fracture line was too low to be fixed with a plate,a tension band wire or screw fixation was used.The reconstruction plate for fixing the lateral column was carefully contoured,allowing the proximal end to be placed on the anterolateral side,and the distal end with the two most distal holes placed on the lateral side of the distal humerus.At least two screws were used to fix the plate to the lateral articular fragment,with one long screw implanted from lateral to medial side and parallel to the articular surface.Inserting the most proximal screws of the lateral and medial plates at the same level should be avoided.The reduction in the articular surface and the length of the screws were checked by C-arm.No excessive movement of the fracture fragments under the motion of the elbow was confirmed under direct vision.The dissected common origin of the flexor muscles was repaired.(3)Tips and tricks during operation:the nerves and blood vessels should be carefully protected during operation.Yi Jiangying et al reported that the anteversion of distal humerus and carrying angle of upper limb should be well reconstructed.For type C3,the first thing is to reduce intercondylar fragments,changing intercondylar fracture to supracondylar fracture,then restore the lateral column of distal humerus,in the end is to focus on the recovery of the trochlea articular surface.(4)Postoperative treatment:Antibiotics were routinely used in 3-5d.The drainage tube was removed in 48-72h.The stitches would be removed after two weeks.Plaster cast or hinged splint was properly applied to protect the elbow according to the classification of the fracture and the actual situation of patients.Early functional exercise was conducted.After a week or so,patients would be encouraged to do elbow flexion and extension.Rehabilitation protocol should be individualized according to fracture type and patients status.The intensity of rehabilitation also should be increased gradually.Proper upper limb weight bearing was allowed after 6-8weeks.ResultsAll 24patients were successfully operated.Operation time variedfrom 55to 270minutes,and averaged in 143min.Blood loss was ranged from 50to 400ml,and averaged in 183ml.All 24patients achieved Stage I healing.No swelling,effusion,or infection was observed.Postoperative follow-up was 3-6months(averaged 4.5months).Callus formation was observed in fracture end.No internal fixation loosening,myositis ossifications,malunion,delayed union or nonunion was observed in follow-ups.The outcome was evaluated according to Mayo Clinic Elbow Score.Good and excellent rate was 62.5%at 3months postoperatively.ConclusionsClassifying the distal humeral fractures using the imaging data is important for choosing appropriate surgery method.The satisfied reduction,rigid internal fixation and early exercise are critical for the functional recovery of the elbow.
Humerus fractures,distal;Surgical treatment;Curative effect
Chen Bin,Email:drchenbin@vip.sina.com
2014-07-06)
(本文编辑:李静)
10.3877/cma.j.issn.2095-5790.2014.03.007
067000 承德医学院附属医院骨外六科
陈宾,Email:drchenbin@vip.sina.com
赵龙,宋有鑫,崔成喜,等.复杂肱骨远端骨折手术治疗的临床探讨[J/CD].中华肩肘外科电子杂志,2014,2(3):168-173.