Ethno-medicinal plants used by Bengali communities in Tripura, northeast India
2014-04-19JoydebMajumderParthaBhattacharjeeBadalDattaBasantAgarwala
Joydeb Majumder • Partha P.Bhattacharjee • Badal K.Datta • Basant K.Agarwala
Introduction
Medicinal plants are the richest bio-resource of drugs used in traditional medicinal systems, modern medicines, nutraceuticals, food supplements, folk medicines and pharmaceuticals (Hammer et al.1999).In India, medicinal plants occupy important positions in the socio-cultural, spiritual and medicinal arena of rural people (Kumar et al.2011).The centuries-old Indian Systems of Medicine (ISM) use about 400 kinds of plants in production of ayurvedic, unani, siddha, and tribal medicines.Worldwide, an estimated 20,000 plant species are considered to have medicinal importance, but about 7,500 of those species have only been well documented in the ISM and ethnobotany (Mao et al.2009).About 75% of these are sourced from tropical forests and the remaining 25% from temperate forests.Use of traditional medicine is rapidly growing worldwide (Bussmann and Glenn 2011) despite tremendous advances in synthetic drugs and modern medical science (Sandberg and Corrigan 2001; Salim et al.2008).
Tripura, a small hilly state of northeast India, is rich in floral diversity and represents the western fringe of Indo-Burma biodiversity hotspot of tropical Asia (Myers et al.2000).The 10,492 km2area of the state has closed and open forests distributed across 6,293 km2and represented by 379 species of trees, 320 of shrubs, 581 of herbs, 165 of climbers, 16 of climbing shrubs, 35 of ferns, and 45 species of epiphytes (Sen et al.2011).The geographical area of the state is 0.3% of India’s total but it harbors 13% of the known plant diversity of the country (Kshirsagar and Upadhyay 2009).According to the population census of 2002, about 83% of the state’s population of 3.7 million lives in rural areas (http//tripura.nic.in/tspcd/people.htm).Rural populations are comprised 69% of Bengali people and another 31% of tribal populations.These people are well aware of the traditional use of various plant/forest resources in their daily life (De et al.2010).Several studies have documented ethno-medicinal uses of plants and plant products by the tribal peoples of Tripura (Singh et al.1997; Majumdar and Datta 2007; Das et al.2009; Sen et al.2011), but information on the ethno-botanical knowledge of Bengali people (69% of the total population) of Tripura has not been documented.
Our objectives were to document the ethno-medicinal plants used by the people of Bengali communities, describe plant habits and parts used in medicinal preparations, and report their modes of use in the two largest administrative and forest-rich West and South districts of Tripura, northeast India.
Materials and methods
Study area
Tripura state is located in the bio-geographic zone 9B-North-East Hills at 22°56′ to 24°32′ N and 90°09′ to 92°20′ E.The state shares an 837 km long segment of the India-Bangladesh international border on the north, south, and west at the deltaic basin of Bangladesh, and on the east it shares a boundary with the states of Assam and Mizoram.The length of the state from north to south is 183.5 km and the maximum width from east to west is 112.7 km.Our study was conducted in forested and rural areas of Bengali-dominated villages in the West (23°16′ to 24°14′N and 91°09′ to 91°47′ E) and South (91°18′ to 91°59′ E and 22°56′to 23°45′E) districts of the state.Geographical areas of the two districts are 3,544 km2and 2,624 km2, respectively.
Ethnomedicinal plants survey
We surveyed during 2009 and 2010 for collection of information on plants of ethno-medicinal uses by interviewing informants living in villages adjacent to the forests (Table 1).From each village, about 10% of the total resident population was selected at random as informants who consented to share information.These included medicine-men, older men and women well versed in the identification of plants, and who regularly use and visit nearby forests to source cures for various ailments.Information was collected through interviews, group discussion, and semi-structured questionnaires in local parlance with regard to local names of medicinal plants, names of diseases for which a particular plant is used, part of the plant used, and other information.This method was repeated twice, once in winter 2009 and the second time in the rainy season of 2010.

Table 1: Geo-coordinates of the study locations and sample sizes used in West District (W) and South district (S) of Tripura, northeast India
Data collected from informants of one village were cross-checked with those of other villages to assess the validity of information.Based on the interview data, a consensus index was compiled following Sajem and Gosai (2006) by calculating the percentage of informants who quoted a given specific use of a given plant taxon.Voucher specimens of different plants identified by informants as having medicinal values were collected and their herbaria prepared following the conventional method (Jain1989).These were identified by their biological names (Deb 1981, 1983−1989; Jain 1991; Kritikar and Basu 2005) and deposited in the Department of Zoology, Tripura University.Information about the process of preparation of medicines, modes of application, and doses for the treatment of disease was also recorded.
Results and discussion
Medicinal plants, plant habits and plant parts
Based on the information collected from informants, a total of 93 species of plants of 52 families and 83 genera were used by the Bengali communities as medicines in West and South districts.Some of the plant species were also used for other purposes, viz.religious (17.20%), fish poisoning (1.08%), and veterinary healthcare (6.45%).The use of above-ground plant parts was higher (85.16%) than for the below-ground plant parts (14.84%).Leaves were used more commonly as raw material for many of ethno-botanical preparations followed by fruits, roots, and stem/twig (Fig.1).

Fig.1: Use of medicinal plant parts by Bengali communities of West and South districts of Tripura
Preference for leaves in ethno-medicinal preparations was also reported by Majumdar and Datta (2007), and Sen et al.(2011) in Tripura state in other ethnic communities.For nine plant species, e.g., Centella asiatica (L.), Cissus quadrangularis L., Cuscuta reflexa Roxb., Cynodon dactylon L., Ipomea aquatica Forsk., Marsilea minuta L., Oxalis corniculata L., Polygonum hydropiper L., and Spermacoce hispida L., whole plant parts were used as medicine.The recorded ethnobotanical plant species included herbs, trees, shrubs, climbers, and bamboos (Fig.2).These plants were used to treat more than 55 different human diseases and six diseases of livestock.Treated afflictions included, among others, common cold, cough, wound, pain, skin infection, inflammation, diabetes, jaundice, heart problems, snake bite, nose bleeding, asthma, piles, and respiratory problems.Additives, including sugar (small crystals) or mishri (large crystals), salt or honey were sometimes added to the extracted juice or macerated plant parts to make them tasty or palatable.Sixty-eight plant species were used singly and 25 species were used in mixtures of various plant parts or plant-derived products for therapeutic formulations.Distribution of numbers of plant species by plant family ranged from a maximum of five in the family Asteraceae followed by four species each in Euphorbiaceae, Labiatae, Rubiaceae, and Poaceae, and 1−3 species in the remaining 47 families (Table 2).

Fig.2: Use of ethno-medicinal plants by growth form
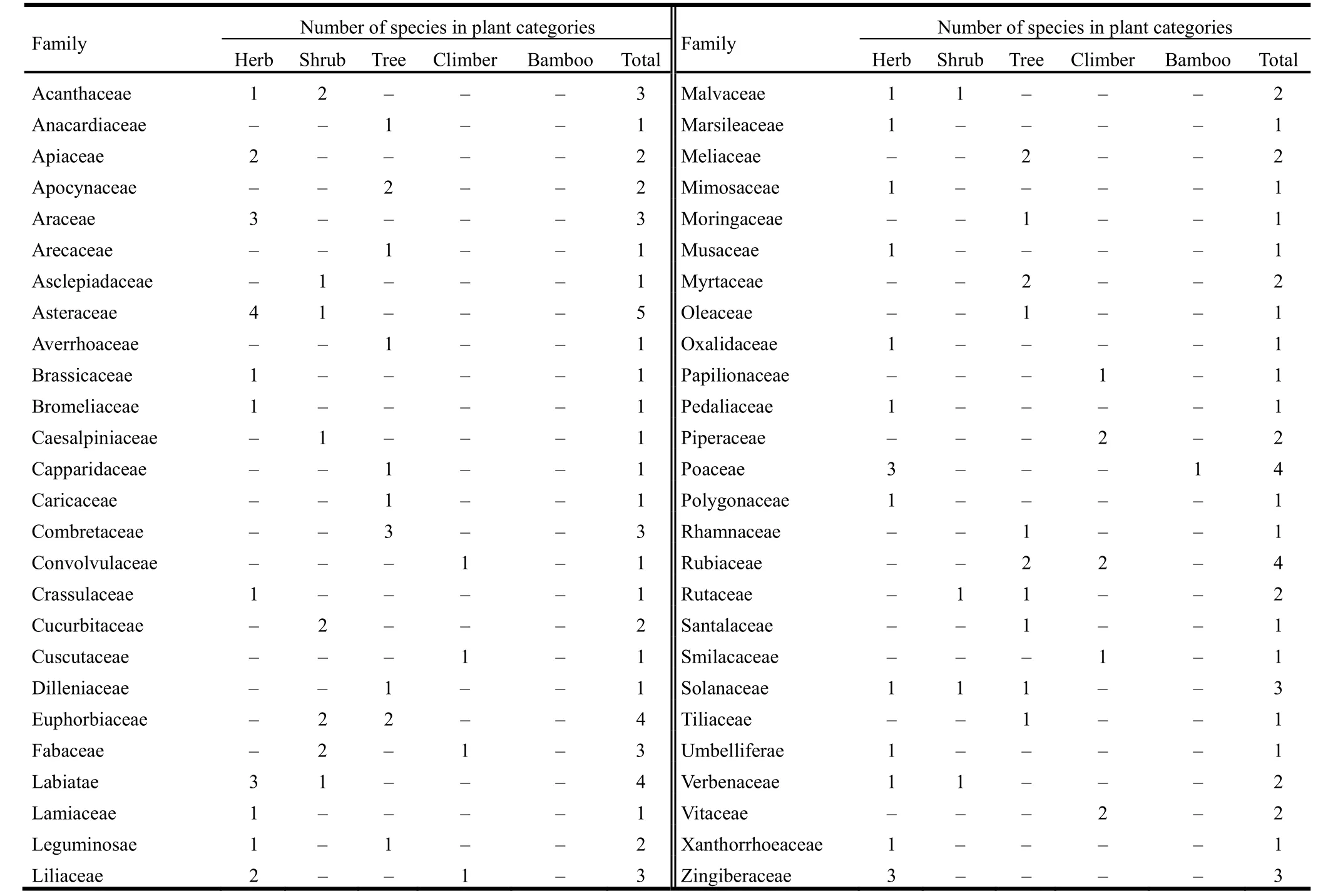
Table 2: Family-wise distribution of different categories of plant species of ethno-medicinal values recorded in the study area
Consensus value of ethnomedicinal plants use
High consensus values of medicinal plants were recorded for most of the species.The maximum value of 96% was recorded for Chromolaena odorata, and the minimum of 15% was recorded for Bambusa balcooa.The highest consensus value for C.odorata could be attributed to its common occurrence in the study area.Das and Agarwala (2011) reported that in the hot, humid environment of northeast India, C.odorata was the most common, aggressive and perennial invasive weed that occurred widely in agriculture, plantations, forests and degraded lands.The mimimum consensus value recorded for B.balcooa could be related to the rare occurrence of a white crystal product present inside the bamboo stem.Several studies have reported that the consensus value of a particular medicinal plant for specific disease treatment is dependent on the availability of plant species and the occurrence of particular diseases in a study area (Teklehaymanot and Giday 2007; Namsa et al.2011).
Validation of ethnomedicinal plant use with reported pharmacological properties
Of the 93 plant species recorded in this study for medicinal use, pharmacological properties for 75 plant species have been documented (Georgewill and Georgewill 2009; Rachana et al.2011; Lambole 2010; Jayanthi and Dhar 2011; Joseph and Justin 2010; Shang et al.2010).Many of these medicinal plants are also used by other ethnic people of Tripura to cure similar kind of diseases (Majumdar and Datta 2007; Das et al.2009; Sen et al.2011).Pharmacological properties of the remaining 18 plant species are yet to be documented.
Conclusion
Tripura is rich in medicinal plants and these are widely used by local people in traditional therapies.Most of these people (68% including tribals) live below the poverty line (BPL) (http//tripura.nic.in/tspcd/people.htm).Ethno-botanical information on medicinal plants and their uses by indigenous cultures is useful not only for the conservation of traditional knowledge and biodiversity but also to promote community health care, and to conserve potential sources of compounds for use in development and manufacture of modern drugs.It is, therefore, important that indigenous knowledge of plants used in traditional health care is safeguarded and protected.Changes in cultural practices due to modernization and globalization pose direct and indirect threats to this heritage, most of which is not properly documented.Approximately 80% of medicinal plants are currently collected from the wild.Adequate ethno-botanical studies and conservation strategies are required to preserve the valuable but vulnerable indigenous knowledge of medicinal plants used by Bengali communities and by other ethnic communities of the state of Tripura.
Acknowledgements
Authors are indebted to Koushik Majumdar, Department of Botany, Tripura University for identification of some of the plant species.Authors are thankful to the villagers of West district and South district for sharing information with us during the field survey and to the Head, Departments of Botany and Zoology, respectively, for extending working facilities.
Bussmann RW, Glenn A.2011.Fighting pain, traditional Peruvian remedies for the treatment of Asthma, Rheumatism, Arthrities and sore bones.Indian Journal of Traditional Knowledge, 10: 397–412.
Das HB, Majumdar K, Datta BK, Ray D.2009.Ethnobotanical uses of some plants by Tripuri and Reang tribes of Tripura.Natural Product Radiance, 8: 172−180.
Das J, Agarwala BK.2011.Changes in leaf chemicals in different phenological stages of Chromolaena odorata L.(King and Robinson) from Tripura.Vegetos, 24: 38−40.
De B, Debbarma T, Sen S, Chakraborty R.2010.Tribal life in the environment and biodiversity of Tripura, India.Current World Environment, 5: 59−66.Deb DB.1981.The Flora of Tripura state.Volume I.New Delhi: Today and Tomorrow’s Printers and Publishers.
Deb DB.1983−1989.The Flora of Tripura state.Volume II.New Delhi: Today and Tomorrow’s Printers and Publishers.
Georgewill QA, Georgewill UO.2009.Evaluation of the anti-inflammatory activity of extract of Abrus precatorious.Eastern Journal of Medicine, 14: 23−25.
Hammer KA, Carson CF, Riley TV.1999.Antimicrobial activity of essential oils and other plant extracts.Journal Applied Microbiology, 86: 985−990.
Jain SK.1989.Methods and Approach in Ethnobotany.Lucknow: National Botanical Research Institute.
Jain SK.1991.Dictionary of Indian Folk Medicine and Ethnobotany.New Delhi, India: Deep Publication.
Jayanthi MK, Dhar M.2011.Anti-inflammatory effects of Allium sativum (galic) in experimental rats.Biomolecules, 31: 84–89.
Jin SG, Chuen LC, Koo MWL.2004.Inhibitory effects of Centella asiatica water extract and asiaticoside on inducible nitric oxide synthase during gastric ulcer healing in rats.Planta Medica, 70: 1150–1154.
Joseph B, Justin RS.2010.Pharmacognostic and phytochemical properties of Aloe vera Linn – an overview.International Journal of Pharmaceutical Sciences Review and Research, 4: 106–110.
Kritikar KR, Basu BD.2005.Indian Medicinal Plants.Derhadun, India: International Book Distributors.
Kshirsagar R, Upadhyay S.2009.Free radical scavenging activity screening of medicinal plants from Tripura, Northeast India.Natural Product Radiance, 8: 117–122.
Kumar A, Ilavarasan R, Jayachandran T, Deecaraman M, Aravindan P, Padmanabhan N, Krishan MRV.2008.Anti-diabetic activity of Syzygium cumini and its isolated compound against streptozotocin-induced diabetic rats.Journal of Medicinal Plant Research, 2: 246–249.
Kumar M, Sheikh MA, Bussmann RW.2011.Ethnomedicinal and ecological status of plants in Garhwal Himalaya, India.Journal of Ethnobiology and Ethnomedicine, 7: 32.
Lambole VB, Murti K, Kumar U, Bhatt SP, Gajera V.2010.Hytopharmacological properties of Aegle marmelos as a potential medicinal tree, an overview.International Journal of Pharmaceutical Sciences Review and Research, 5: 67−72.
Majumdar K, Datta BK.2007.A study on ethnomedicinal uses of plants among the folklore herbalist and Tripuri medical practitioner, part 2.Natural Product Radiance, 6: 66−73.
Mao AA, Hynniewta TM, Sanjappa M.2009.Plant wealth of Northeast India with reference to ethnobotany.Indian Journal of Traditional Knowledge, 8: 96−103.
Myers N, Mittermeier RA, Mittermeier CG, da Fonseca Gustavo AB, Kent J.2000.Biodiversity hotspots for conservation priorities.Nature, 403: 853–858.
Namsa ND, Mandal M, Tangjang S, Mandal SC.2011.Ethnobotany of the Mompa ethnic group at Arunachal Pradesh, India.Journal of Ethnobiology and Ethnomedicine, 7: 31.
Rachana Basu S, Pant M, Kumar MP, Saluja S.2011.Review & Future Perspectives of Using Vasicine, and Related Compounds.Indo Global Journal of Pharmaceutical Sciences, 11: 85−98.
Singh HB, Hynniewta TM, Bora PJ.1997.Ethnomedico botanical studies in Tripura, India.Ethnobotany, 9: 56−58.
Sajem A, Gosai K.2006.Traditional use of medicinal plants by the Jaintia tribes in North Cachar Hills district of Assam, northeast India.Journal of Ethnobiology and ethnomedicine, 2: 33.
Salim AA, Chin YW, Kinghorn AD.2008.Drug discovery from plants.In: K.G.Ramawat, J.M.Merillon (eds), Bioactive molecules and medicinal plants.Berlin: Springer, pp.1−18.
Sandberg F, Corrigan D.2001.Natural remedies, their origins and uses.New York: Taylor & Francis, 1−4.
Sen S, Chakraborty R, De B, Devanna N.2011.An ethnobotanical survey of medicinal plants used by ethnic people in West and South district of Tripura, India.Journal of Forestry Research, 22: 417−426.
Shang JH, Cai XH, Zhao YL, Feng T, Luo XD.2010.Pharmacological evaluation of Alstonia scholaris, anti-tussive, antiasthmatic and expectorant activities.Journal of Ethnopharmacology, 129: 293−298.
Teklehaymanot T, Giday M.2007.Ethnobotanical study of medicinal plants used by people in Zegie Peninsula, Northwestern Ethiopia.Journal of Ethnobiology and Ethnomedicine, 3: 12.
杂志排行

Journal of Forestry Research的其它文章
- Biodiversity of endophytic fungi from seven herbaceous medicinal plants of Malnad region, Western Ghats, southern India
- Litter production, decomposition and nutrient mineralization dynamics of Ochlandra setigera: A rare bamboo species of Nilgiri Biosphere Reserve, India
- Temporal changes in nitrogen acquisition of Japanese black pine (Pinus thunbergii) associated with black locust (Robinia pseudoacacia)
- Plant diversity at Chilapatta Reserve Forest of Terai Duars in subhumid tropical foothills of Indian Eastern Himalayas
- Floristic composition and management of cropland agroforest in southwestern Bangladesh
- The changing landscape of mangroves in Bangladesh compared to four other countries in tropical regions