心房颤动相关缺血性卒中的研究进展
2014-03-08李姝雅王伊龙王拥军
李姝雅,王伊龙,王拥军
心房颤动(atrial fibrillation,AF)是最常见的室上性心动过速,人群总体患病率为0.4%~1.0%[1-2]。一些心房颤动患者缺乏明显的、特征性的临床表现,许多患者直到出现严重并发症时才被检出心房颤动。心房颤动是缺血性卒中的一个重要的独立危险因素,约每6例卒中患者中有1例是心房颤动患者[3]。伴心房颤动的缺血性卒中患者复发率高、预后差,给社会和家庭造成沉重的负担[4-9]。合理应用抗凝治疗可降低心房颤动患者的卒中风险[10-11],过度抗凝治疗增加患者出血风险[12-13]。由于目前医疗水平的限制及循证医学资料的匮乏,对于心房颤动患者的检出和管理仍缺乏有效的、一致的意见,探索卒中合并心房颤动患者管理规范尤为重要。
1 心房颤动患者的卒中危险分层评估和新型抗凝药物的发展
抗凝治疗可以降低心房颤动患者卒中发生率,但因出血风险而限制其临床应用。鉴于抗凝的利弊,评估心房颤动患者卒中发生风险和出血风险,平衡利弊,显得极为重要。20世纪90年代初,学者们就致力于建立一个有效的心房颤动患者卒中危险评分工具(表1)[14-21],经过20年的不断发展,最新的卒中危险分层工具是CHADS2评分(Congestiveheart failure,Hypertension,Age>75 yrs,Diabetes mellitus,prior Stroke and TIA)[22]和CHA2DS2_VASc评分[Congestive heart failure,Hypertension,Age≥75(Doubled),Diabetes,Stroke(doubled),Vascular disease,Age 65~74,and Sex category(female)][23](表2)。CHADS2评分和CHA2DS2_VASc评分已在欧洲、日本、韩国等多个地区心房颤动人群中进行验证,得到其预测1年心源性卒中风险的曲线下面积(area under curve,AUC)(C值)在0.60~0.63[24-26]。2001年问世的CHADS2评分是基于专家共识产生的总分为6分的经典危险分层工具,在其产生队列中显示出良好的效度(C=0.82)。该评分因操作简单,效度良好,一经问世即在临床上广泛应用,随着临床试验的不断检验,Lip等[27]根据临床实践修订了CHADS2的危险分层标准。Gage等[28]将更改了分层方法的CHADS2评分在“心房颤动患者应用口服凝血酶抑制剂预防卒中研究”(Stroke Prevention using an ORal Thrombin Inhibitor in atrial Fibrillation,SPORTIF)中进行验证,约60%的患者被分为中危患者,指南中对于中危患者抗栓药物选择没有明确推荐,限制了CHADS2评分对抗栓药物应用的指导意义。2010年CHA2DS2_VASc评分是一种以危险因素为基础评价非瓣膜性心房颤动患者的方法,改进了心房颤动患者发生卒中的危险分层。这一评分方法将CHADS2评分得到的中危人群比例降低到原来的1/4,进一步增强了评分工具对抗凝治疗的指导意义[23]。根据上述评分标准,对于伴心房颤动的缺血性卒中患者,属于存在既往卒中病史的心房颤动患者,至少得到2分,属高危分层,需抗凝治疗。

表1 心房颤动患者卒中风险评分工具

表2 CHADS2和CHA2DS2_VASc评分
卒中等血栓栓塞性并发症是心房颤动患者致死、致残的主要原因,合理的抗凝治疗对于改善心房颤动患者生活质量和远期预后具有重要意义。虽然国内外相关指南均建议给予高危心房颤动患者血栓预防治疗,但迄今多数患者并未得到相应处理,这与口服抗凝药物的选择限制密切相关[29-30]。目前成熟的口服抗凝药物只有维生素K拮抗剂华法林。华法林应用时需根据凝血酶原国际标准化比值(international normalized ratio,INR)调整剂量,且其抗凝效果受食物影响大,出院患者自行用药风险极大。新型口服抗凝剂凝血因子Ⅹa抑制剂克服了上述困难,具备高效、安全、固定剂量、无需监测INR的特点,未来将占据口服抗凝药物的市场,为抗凝治疗带来新的时代。达比加群酯(Pradaxa)、利伐沙班(rivaroxaban)和阿哌沙班(apixaban)是目前批准上市的新型抗凝药物。这三类新型抗凝药物都经过了大型临床试验的证实,在抗凝疗效和出血风险方面不同程度地优于阿司匹林和华法林,这就意味着在心房颤动相关卒中预防中新型抗凝剂时代已经到来[22,31-35]。
2 伴心房颤动的缺血性卒中患者抗凝治疗的出血风险
伴心房颤动的缺血性卒中患者的抗凝治疗是一把双刃剑,在对心房颤动患者进行抗凝治疗的同时应当评估其出血风险(表3)。出血风险的研究略晚于心房颤动患者的卒中风险,最早的出血风险评分工具诞生于1998年[36],以年龄、2周内胃肠道出血、卒中史及并发症为危险因素,根据得分判断出血风险,其用C值代表的预测大出血的效度为0.78。1年后,Kuijer等[37]提出了以年龄、性别和癌症三种危险因素组成的抗凝治疗出血风险预测评分,在其验证队列中,用C值代表的评分对大出血的预测效度为0.82[95%可信区间(confidence interval,CI):0.66~0.98]。因出血风险与年龄呈正相关,Shireman等[38]提出了一个适用于年龄>65岁心房颤动患者的评分工具,其低、中、高危患者的出血率分别为0.9%、2.0%和5.4%。2006年,Gage等[39]发表了出血危险的预测量表模型:肝脏或肾脏疾病、酗酒、恶性肿瘤、高龄、血小板计数或功能降低、再次出血、高血压、贫血、基因因素、容易摔倒危险和卒中(Hepatic or renal disease,Ethanol abuse,Malignancy,Older age,Reduced platelet count or function,Re-bleeding,Hypertension,Anemia,Genetic factors,Excessive fall risk and Stroke;HEMORR2HAGES)评分工具,该评分方法较为繁琐,但心房颤动患者抗凝治疗的出血风险随着得分的增加而增高。2010年Pisters等[40]提出的另一个预测模型:高血压、肝/肾功能异常、卒中、出血史或易于出血因素、不稳定国际标准化比值、老年人、药物/酒精(Hypertension,Abnormal renal/liver function,Stroke,Bleeding history or predisposition,Labile international normalized ratio,Elderly,Drugs/alcohol,HAS-BLED)评分量表因操作简单,对单纯抗血小板治疗及非抗栓治疗组出血风险的预测能力则强于其他评分系统(C值分别为0.91和0.80),成为欧洲心脏病协会(European Society of Cardiology,ESC)心房颤动管理指南对出血风险定量分析的推荐工具(表4)。该量表总分为9分,规定HAS-BLED评分≥3分为高危人群,1~2分为中危人群,0分为低危人群,对于高危人群,在应用抗凝药物或阿司匹林时需密切注意全身出血倾向。

表3 心房颤动患者抗凝治疗出血风险评分

表4 HAS-BLED评分
HAS-BLED评分指导抗凝治疗需与心房颤动患者卒中风险评分工具合用。在心房颤动患者中同时应用CHADS2和HAS-BLED评分将会减少12%接受抗凝治疗而出血的人数。当CHADS2评分≥2时,患者存在卒中高风险,推荐抗凝治疗,若此时HAS-BLED评分大于CHADS2评分,则出血风险超过抗凝获益。对于CHADS2评分=1分的患者,HAS-BLED评分与CHADS2评分相差不超过2分时,抗凝获益大于出血风险[41]。
上述5种抗凝治疗出血风险预测工具均是在未接受抗凝治疗的研究队列中产生和验证,为进一步预测接受抗凝治疗的患者自发性脑出血风险,Fang等[42]提出了基于心房颤动抗凝和危险因素的研究(Anticoagulation and Risk Factors in Atrial Fibrillation,ATRIA)评分。该研究在基于社区的大规模心房颤动患者队列中建立了评估华法林相关出血风险评估的有效方法,在最终风险模型中识别出5个独立变量,包括贫血、肾脏疾病(肾小球滤过率<30 ml/min或接受透析)、年龄≥75岁、曾因出血住院和高血压。效度分析得到的C统计值为0.74。评分划分低危(0~3分)、中危(4分)和高危(5~10分)患者的主要出血事件发生率分别为0.8%、2.6%和5.8%。ATRIA评分产生后,Lip等[43]将HEMORR2HAGES评分,HAS-BLED评分和ATRIA评分的预测能力进行了比较。效度分析(relative operating characteristic,ROC分析)显示HAS-BLED评分预测任何临床相关出血方面最佳,但三者对出血风险均有较保守的预测能力(C值均<0.7)。在改善分析(net reclassification index,NRI)中,HASBLED评分被证实相对于HEMORR2HAGES及ATRIA评分可以分别改善10.3%和13%。使用决定曲线分析(detrended correspondence analysis,DCA)显示,HAS-BLED评分在临床相关出血事件任何界值水平方面优于ATRIA和HEMORR2HAGES评分。另外,颅内出血是抗凝治疗中最危险的并发症,只有HAS-BLED评分对颅内出血具有预测价值。因此,HAS-BLED评分可能成为指南推荐工具。Lip教授[44]评论:“HAS-BLED高评分不能被认为是停止抗凝治疗的指标,而是促使临床医师关注这类需要特别留意与随访的高危患者。HAS-BLED评分使临床医师考虑潜在的可纠正的出血风险因素,比如未控制的血压,不稳定的INR值,以及合并用药中的阿司匹林及非甾体抗炎药。”来自中国台湾[45]和西班牙[46]的数据同样证实了HAS-BLED评分的优势。目前,HAS-BLED评分是唯一国际指南推荐的抗凝治疗风险预测评分[47-49]。
3 提高卒中患者伴发心房颤动的检出率
阵发性和无症状性心房颤动难以检出,因此隐源性卒中和短暂性脑缺血发作患者可能存在未诊断的心房颤动,心房颤动的检出在卒中二级预防中处于关键优先地位。我国心源性卒中的整体出院诊断率为6%~7%,这与国外报道的20%比例相距甚远[22,49],从一个侧面说明了我国心源性卒中的诊断率较低。研究证实通过新技术延长心电监测时间可提高心房颤动检出率,但其成本效益存在争议[50-54]。美国的一项研究对卒中患者心房颤动检出(Score for the Targeting of Atrial Fibrillation,STAF)评分≥5分的患者进行连续21 d心电监测,心源性卒中的诊断率提高到13%,这比当时的总体诊断率提高了6%[51]。另一研究提出,通过延长心电监测时间每多诊断一位心源性卒中患者需要耗费的成本为44 000美元[52]。对患者进行心房颤动风险评估,针对高危患者延长心电监测时间,提高心房颤动检出率,是符合成本效益的卒中二级预防内容。2010年Suissa等[55]提出了STAF评分系统,从4个方面对卒中患者进行评分,总分为8分(表5)。根据相应的受试者工作特征(receiver operating characteristic,ROC)曲线得出总得分<5分,心源性卒中的可能性<10%;如果总分≥5分,心源性卒中的可能性则可以达到90%,建议进一步延长心电监测时间。该评分识别心房颤动患者的敏感性为89%,特异性为88%。阵发性心房颤动和短阵心房颤动是提高心房颤动检出率的关键。Suissa等[56]提出,STAF评分≥5分对于阵发性心房颤动和持续性心房颤动的作用无显著性差异,两者的C值分别为0.907和0.911,其识别阵发性心房颤动的敏感性为91%,特异性为77%。德国的一项研究进一步探讨了STAF评分对于阵发性心房颤动的预测能力[57]。效度分析结果提示C值为0.84,STAF评分≥5分对于识别阵发性心房颤动的敏感性为79%,特异性为74%。继STAF评分之后,Malik等[58]提出了用于卒中患者心房颤动风险预测的LADS评分(Left atrial diameter,Age,Diagnosis of stroke or TIA,and Smoking status)(表5)。该评分总分为6分,规定≥4分为心房颤动高风险患者,其识别心房颤动患者的敏感性为85.5%,特异性为53.1%。经过LADS评分的分类,可减少47%的卒中或TIA患者接受长时间心电监测。由于LADS评分的预测能力略低于STAF评分,目前尚无对LADS评分进一步验证的相关研究。
STAF评分筛选出卒中患者中伴发心房颤动的高危人群,高危人群需延长心电监测时间进一步检出心房颤动,目前相关指南尚未对心电监测时长给予建议,研究建议对卒中患者早期实施心房颤动筛查有助于提高心房颤动的检出率,最短监测时间为4 d[59]。可插入心脏监测器这一新技术不仅较7 d的连续心电监测提高心房颤动的检出率,且对患者而言更易耐受,无不良反应,将成为提高心房颤动检出率的新方向[55,60]。
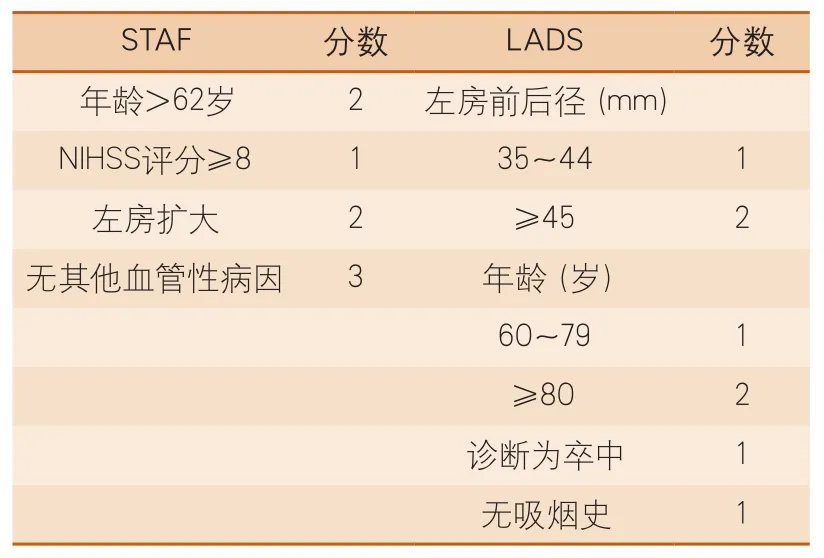
表5 STAF和LADS评分
4 伴心房颤动的缺血性卒中患者的不良预后量表
目前,尚无单纯用于伴心房颤动的缺血性卒中患者的不良预后量表。用于心房颤动患者卒中危险分层的CHADS2和CHA2DS2_VASc评分,其组成元素均为卒中复发和卒中后死亡的独立危险因素。由此推测,两种评分工具可能对于发生缺血性卒中的心房颤动患者卒中复发和不良预后方面有一定的预测价值。既往研究将CHADS2和CHA2DS2_VASc评分应用于伴非瓣膜性心房颤动的缺血性卒中患者预后结局的预测,发现这两种评分工具是不良预后和死亡的独立危险因素[61-63]。希腊的一项研究将CHA2DS2_VASc评分应用于非心房颤动患者,中、高危分层患者的5年死亡率,卒中复发率和联合心血管事件明显高于低危分层的患者[64]。
心房颤动或不伴心房颤动患者的不良预后危险因素基本一致是CHA2DS2_VASc评分可用于不伴心房颤动患者预后评价的基础。随着大型高质量队列研究的逐渐发展和完善,研究者们提出了多个不良预后风险预测模型(表6)。这些风险预测模型未将伴心房颤动的缺血性卒中排除在外,可初步作为心房颤动相关卒中的预后评估工具。

表6 缺血性卒中死亡和不良预后评估量表
iScore评分[65]是基于加拿大卒中登记的一项较早的预测模型,预测急性缺血性卒中患者30 d和1年的死亡风险。预测模型在建模队列(30 d死亡,C=0.85;1年死亡,C=0.823)、内部验证队列(30 d死亡,C=0.851;1年死亡,C=0.84)和外部验证队列(30 d死亡,C=0.79;1年死亡,C=0.782)中均得到较好的预测效度。随后,iScore评分分别用于不良预后风险预测,溶栓患者出血风险及预后转归预测,均得到理想结果[66-68]。PLAN评分[69]预测模型来源于另一个加拿大卒中登记,用于预测缺血性卒中患者出院30 d、1年的死亡率和出院时改良Rankin量表(modified Rankin Scale,mRS)评分5~6分。预测模型包括9项临床指标,操作相对简单,可以准确预测急性缺血性卒中患者30 d死亡(C=0.87),出院时死亡或严重致残(C=0.88)、1年死亡(C=0.84)。同时也可以预测出院时的良好结局(mRS 0~2)(C=0.80)。美国心脏协会在其协作医院的冠状动脉疾病单元中推行的跟着指南走(Get-with-the-Guideline)建立了在院死亡模型[70],其包括美国国立卫生研究院卒中量表(National Institutes of Health Stroke Scale,NIHSS)评分的预测模型对于院死亡的预测效度为0.85(0.84~0.86)。
洛桑卒中登记(The Acute STroke Registry and Analysis of Lausanne,ASTRAL)评分预测模型[71]主要预测不良预后风险,不良预后定义为mRS评分>2分。在建模队列中预测3个月不良预后风险的C值为0.86,在两个其他队列研究中进行外部验证,C值分别为0.937和0.771,预测效度良好。博洛尼亚研究(the Bologna Outcome Algorithm for Stroke,BOAS)模型[72]是意大利博洛尼亚市登记队列推出的用于预测9个月不良预后的模型,包括NIHSS评分、年龄、上肢永久瘫痪、吸氧和导尿5个危险因素,每个危险因素1分,总分为5分。0~1分为低危分组,2~5分为高危分组。该评分在建模队列(C=0.891,95%CI 0.848~0.934)和验证队列(C=0.845,95%CI 0.770~0.920)中均表现出良好的预测能力。美国弗明汉心脏登记研究建立了用于心脏病一级预防的(Framingham Cardiovascular Risk Score,FCRS)模型[73],将FCRS模型用于卒中二级预防出院时不良预后风险预测和出院去向预测,得到FCRS模型对于出院时mRS≥2分的比值比(odds ratio,OR)为4.9(95%CI 0.98~24.1),出院回家的OR=0.18(95%CI 0.04~0.86),FCRS模型是对缺血性卒中患者出院回家的保护性因素。
上述预测模型适用于缺血性卒中患者,缺血性卒中患者发病机制及病理生理特点异质性较强,建立针对伴心房颤动的缺血卒中患者的预测模型仍有待进一步研究。
5 伴心房颤动的缺血性卒中研究展望
美国心脏协会/美国卒中学会(American Heart Association/American Stroke Association,AHA/ASA)评选出2011年全球脑血管病最重要的十大研究进展中,与心房颤动相关的卒中占了三席,包括心房颤动的危险因素[74]、心房颤动患者的降压药物选择[75]及新型口服抗凝药物[31-36],成为2011年卒中研究领域最抢眼的热点。大约有1/5的卒中是由心房颤动所致,未被诊断的心房颤动即无症状性心房颤动很可能是原因不明卒中的病因。心房颤动所致的卒中相对严重,会导致长期的残疾或死亡。心房颤动作为心源性卒中最常见的原因,提高其检出率,指导一级预防、二级预防及预后评估对于卒中医疗质量改进及提高患者生活质量意义重大,任重而道远。
1 Feinberg WM, Blackshear JL, Laupacis A, et al.Prevalence, age, distribution and gender of patients with atrial fibrillation:analysis and implications[J].Arch Intern Med, 1995, 155:469-473.
2 Go AS, Hylek EM, Phillips KA, et a1. Prevalence of diagnosed atrial fibrillation in adults:national implications for rhythm management and stroke prevention:the Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study[J]. JAMA, 2001,295:2370-2375.
3 Hart RG, Halperin JL. Atrial fibrillation and thromboembolism:a decade of progross in stroke prevention[J]. Ann Intem Med, 1999, 131:688-695.
4 Winter Y, Wolfram C, Schaeg M, et al. Evaluation of costs and outcome in cardioembolic stroke or TIA[J].J Neurol, 2009, 256:954-963.
5 Schneck M, Lei X. Cardioembolic stroke[J/OL]. eMed Neurol, 2008.
6 Bruggenjurgen B, Rossnagel K, Roll S, et al. The impact of atrial fibrillation on the cost of stroke:The berlin acute stroke study[J]. Value Health, 2007,10:137-143. http://emedicine.medscape.com/article/1160370-overview.
7 Jorgensen HS, Nakayama H, Reith J, et a1. Acute stroke with atrial fibrillation. The Copenhagen Stroke Study[J]. Stroke, 1996, 27:1765-1769.
8 Marini C, De Santis F, Sacco S, et a1. Contribution of atrial fibrillation to incidence and outcome of ischemic stroke:results from a population-based study[J]. Stroke, 2005, 36:1115-1119.
9 Steger C, Pratter A, Martinek-Bregel M, et a1. Stroke patients with atrial fibrillation have a worse prognosis than patients without:data from the Austrian Stroke registry[J]. Eur Heart J, 2004, 25:1734-1740.
10 Wann LS, Curtis AB, January CT, et al. 2011 ACCF/AHA/HRS focused update on the management of patients with atrial fibrillation (updating the 2006 guideline):A report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines[J]. Circulation, 2011,123:104-123.
11 Connolly S, Pogue J, Hart RP, et al. Clopidogrel plus aspirin versus oral anticoagulation for atrial fibrillation in the atrial fibrillation clopidogrel trial with irbesartan for prevention of vascular events(active w):A randomised controlled trial[J]. Lancet,2006, 367:1903-1912.
12 Nieuwlaat R, Capucci A, Lip GY, et al. Euro Heart Survey Investigators. Antithrombotic treatment in real-life atrial fibrillation patients:a report from the Euro Heart Survey on Atrial Fibrillation[J]. Eur Heart J, 2006, 27:3018-3026.
13 Reynolds MW, Fahrbach K, Hauch O, et al. Warfarin anticoagulation and outcomes in patients with atrial fibrillation:A systematic review and meta analysis[J].Chest, 2004, 126:1938-1945.
14 [No authors listed]. Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation.Analysis of pooled data from five randomized controlled trials[J]. Arch Intern Med, 1994, 154:1449-1457.
15 Stroke Prevention in Atrial Fibrillation Investigators.Risk factors for thromboembolism during aspirin therapy in patients with atrial fibrillation:The Stroke Prevention in Atrial Fibrillation Study[J]. J Stroke Cerebrovasc Dis, 1995, 5:147-157.
16 van Latum JC, Koudstaal PJ, Venables GS, et al.Algra A for the European Atrial Fibrillation Trial(EAFT) Study Group. Predictors of major vascular events in patients with a transient ischemic attack or minor ischemic stroke with nonrheumatic atrial fibrillation[J]. Stroke, 1995, 16:801-806.
17 Wang TJ, Massaro JM, Levy D, et al. A risk score for predicting stroke or death in individuals with new-onset atrial fibrillation in the community:The Framingham heart study[J]. JAMA, 2003, 290:1049-1056.
18 National Collaborating Centre for Chronic Conditions.Atrial Fibrillation:National Clinical Guideline for Managementin Primary and Secondary Care[M].London:Royal College of Physicians, 2006.
19 Fuster V, Ryden LE, Cannom DS, et al. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation-executive summary:A report of the American College of Cardiology/American Heart Association task force on practice guidelines and the European Society of Cardiology committee for practice guidelines (writing committee to revise the 2001 guidelines for the management of patients with atrial fibrillation)[J]. Eur Heart J, 2006, 27:1979-2030.
20 Singer DE, Albers GW, Dalen JE, et al; American College of Chest Physicians. Antithrombotic therapy in atrial fibrillation:American College of Chest Physicians evidence-basedclinical practice guidelines(8th edition) [J]. Chest, 2008, 133:546S-592S.
21 Reitbrock S, Heeley E, Plumb J, et al. Chronic atrial fibrillation:incidence, prevalence and prediction of stroke using the Congestive heart failure,Hypertension, Age>75, Diabetes mellitus, and prior Stroke or transient ischemic attack (CHADS2) risk stratification scheme[J]. Am Heart J, 2008, 156:57-64.
22 Gage BF, Waterman AD, Shannon W, et al. Validation of clinical classification schemes for predicting stroke:Resultsfrom the national registry of atrial fibrillation[J]. JAMA, 2001, 285:2864-2870.
23 Lip GY, Nieuwlaat R, Pisters R, et al. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach:The Euro Heart Survey on atrial fibrillation[J]. Chest, 2010, 137:263-272.
24 Keogh C, Wallace E, Dillon C, et al. Validation of the CHADS2clinical prediction rule to predict ischaemic stroke. A systematic review and meta-analysis[J].Thromb Haemost, 2011, 106:528-538.
25 Olesen JB, Lip GY, Hansen ML, et al. Validation of risk stratification schemes for predicting stroke and thromboembolism in patients with atrial fibrillation:Nationwide cohort study[J]. BMJ, 2011,342:d124.
26 Lip GY, Frison L, Halperin JL, et al. Identifying patients at high risk for stroke despite anticoagulation:A comparison of contemporary stroke risk stratification schemes in an anticoagulated atrial fibrillation cohort[J]. Stroke, 2010, 41:2731-2738.
27 Lip GY, Lim HS. Atrial fibrillation and stroke prevention[J]. Lancet Neurol, 2007, 6:981-993.
28 Baruch L, Gage BF, Horrow J, et al. Can patients at elevated risk of stroke treated with anticoagulants be further risk stratified[J]. Stroke, 2007, 38:2459-2463.
29 Mant J, Hobbs FD, Fletcher K, et al. Warfarin versus aspirin for stroke prevention in an elderly community population with atrial fibrillation (the Birmingham Atrial Fibrillation Treatment of the Aged Study,BAFTA):A randomised controlled trial[J]. Lancet,2007, 370:493-503.
30 Fang MC, Go AS, Chang Y, et al. A new risk scheme to predict warfarin-associated hemorrhage:The ATRIA (Anticoagulation and Risk Factors in Atrial Fibrillation) study[J]. J Am Coll Cardiol, 2011, 58:395-401.
31 Eikelboom JW, Wallentin L, Connolly SJ, et al. Risk of bleeding with 2 doses of dabigatran compared with warfarin in older and younger patients with atrial fibrillation. An analysis of the Randomized Evaluation of Long-Term Anticoagulant Therapy (RE-LY)Trial[J]. Circulation, 2011, 123:2363-2372.
32 ROCKET AF Study Investigators. Rivaroxabanonce daily, oral, direct factor Xa inhibition compared with vitamin K antagonism for prevention of stroke and embolism trial in atrial fibrillation:Rationale and design of the ROCKET AF study[J]. Am Heart J,2010, 159:340-347, e341.
33 Hankey GJ, Patel MR, Stevens SR, et al. Rivaroxaban compared with warfarin in patients with atrial fibrillation and previous stroke or transient ischaemic attack:A subgroup analysis of ROCKET AF[J]. Lancet Neurol, 2012, 11:315-322.
34 Stuart JC, John E, Campbell J, et al. Apixaban in patients with atrial fibrillation[J]. N Engl J Med, 2011,364:806-817.
35 Granger CB, Alexander JH, Mcmurray JJ, et al.Apixaban versus warfarin in patients with atrial fibrillation[J]. N Engl J Med, 2011, 365:981-992.
36 Beyth RJ, Qui m LM, Landefeld CS. Prospective evaluation of an index for predicting the risk of major bleeding in outpatients treated with warfarin[J]. Am J Med, 1998, 105:91-99.
37 Kuijer PM, Hutten BA, Prins MH, et a1. Prediction of the risk of bleeding during anticoagulant treatment for venous thromboembolism[J]. Arch Intern Med, 1999,159:457-460.
38 Shireman TI, Mahnken JD, Howard PA, et al.Development of a contemporary bleeding risk model for elderly warfarin recipients[J]. Chest, 2006,130:1390-1396.
39 Gage BF, Yan Y, Milligan PE, et a1. Clinical classification schemes for predicting hemorrhage:results from the National Registry of Atrial Fibrillation (NRAF)[J]. Am Heart J, 2006,151:713-719.
40 Pisters R, Lane DA, Nieuwlaat R, et al. A novel userfriendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation:The Euro Heart Survey[J]. Chest, 2010, 138:1093-1100.
41 Romero-Ortuno R, O'Shea D. Aspirin versus warfarin in atrial fibrillation:Decision analysis may help patients' choice[J]. Age Ageing, 2012, 41:250-254.
42 Fang MC, Go AS, Chang Y, et al. A new risk scheme to predict warfarin-associated hemorrhage:The ATRIA(Anticoagulation and Risk Factors in Atrial Fibrillation)study[J]. J Am Coll Cardiol, 2011, 58:395-401.
43 Apostolakis S, Lane DA, Guo Y, et al. Performance of the hemorrhages, atria, and HAS-BLED bleeding riskprediction scores in patients with atrial fibrillation undergoing anticoagulation:The AMADEUS(evaluating the use of sr34006 compared to warfarin or acenocoumarol in patients with atrial fibrillation)study[J]. J Am Coll Cardiol, 2012, 60:861-867.
44 Lip GY. Stroke and bleeding risk assessment in atrial fibrillation:When, how, and why?[J]. Eur Heart J,2013, 34:1041-1049.
45 Lip GY, Lin HJ, Hsu HC, et al. Comparative assessment of the HAS-BLED score with other published bleeding risk scoring schemes, for intracranial haemorrhage risk in a non-atrial fibrillation population:The Chin-Shan community cohort study[J]. Int J Cardiol, 2013, 168:1832-1836.
46 Roldan V, Marin F, Fernandez H, et al. Predictive value of the HAS-BLED and atria bleeding scores for the risk of serious bleeding in a "realworld" population with atrial fibrillation receiving anticoagulant therapy[J]. Chest, 2013, 143:179-184.
47 Camm AJ, Kirchhof P, Lip GY, et a1. Guidelines for the management of atrial fibrillation:the task force for the management of atrial fibrillation of the European Society of Cardiology (ESC)[J]. Eur Heart J, 2010,31:2369-2429.
48 Cairns JA, Cormolly S, MeMurtry S, et a1.Canadian Cardiovascular Society atrial fibrillation guidelines 2010:prevention of stroke and systemic thromboembolism in atrial fibrillation and flutter[J].Can J Cardiol, 2011, 27:74-90.
49 Paciaroni M, Agnelli G, Micheli S, et al. Efficacy and safety of anticoagulant treatment in acute cardioembolic stroke:A meta-analysis of randomized controlled trials[J]. Stroke, 2007, 38:423-430.
50 Taya AH, Tian M, Kelly KM, et al. Atrial fibrillation detected by mobile cardiac outpatient telemetry in cryptogenic TIA or stroke[J]. Neurology, 2008,71:1696-1701.
51 Douen AG, Pageau N, Medic S. Serial electrocardiographic assessments significantly improve detection of atrial fibrillation 2.6-fold in patients with acute stroke[J]. Stroke, 2008, 39:480-482.
52 Kamel H, Hegde M, Johnson DR, et al. Costeffectiveness of outpatient cardiac monitoring to detect atrial fibrillation after ischemic stroke[J].Stroke, 2010, 41:1514-1520.
53 Stahrenberg R, Weber-Kruger M, Seegers J, et al.Enhanced detection of paroxysmal atrial fibrillation by early and prolonged continuous holter monitoring in patients with cerebral ischemia presenting in sinus rhythm[J]. Stroke, 2010, 41:2884-2888.
54 Cotter PE, Martin PJ, Ring L, et al. Incidence of atrial fibrillation detected by implantable loop recorders in unexplained stroke[J]. Neurology, 2013, 80:1546-1550.
55 Suissa L, Bertora D, Lachaud S, et al. Score for the Targeting of Atrial Fibrillation (STAF):a new approach to the detection of atrial fibrillation in the secondary prevention of ischemic stroke[J]. Stroke,2009, 40:2866-2868.
56 Suissa L, Mahagne MH, Lachaud S. Score for the targeting of atrial fibrillation:A new approach to diagnosing paroxysmal atrial fibrillation[J].Cerebrovasc Dis, 2011, 31:442-447.
57 Horstmann S, Rizos T, Guntner J, et al. Does the STAF score help detect paroxysmal atrial fibrillation in acute stroke patients?[J]. Eur J Neurol, 2013, 20:147-152.
58 Malik S, Hicks WJ, Schultz L, et al. Development of a scoring system for atrial fibrillation in acute stroke and transient ischemic attack patients:The LADS scoring system[J]. J Neurol Sci, 2011, 301:27-30.
59 Suissa L, Lachaud S, Mahagne MH. Optimal timing and duration of continuous electrocardiographic monitoring for detecting atrial fibrillation in stroke patients[J]. J Stroke Cerebrovasc Dis, 2013, 22:991-995.
60 Ritter MA, Kochhauser S, Duning T, et al. Occult atrial fibrillation in cryptogenic stroke:Detection by 7-day electrocardiogram versus implantable cardiac monitors[J]. Stroke, 2013, 44:e135.
61 Hong HJ, Kim YD, Cha MJ, et al. Early neurological outcomes according to CHADS2score in stroke patients with non-valvular atrial fibrillation[J]. Eur J Neurol, 2012, 19:284-290.
62 Sato S, Yazawa Y, Itabashi R,et al. Pre-admission CHADS2score is related to severity and outcome of stroke[J]. J Neurol Sci, 2011, 307:149-152.
63 Giralt-Steinhauer E, Cuadrado-Godia E, Ois A, et al. CHA2DS2_VASc score and prognosis in ischemic strokes with atrial fibrillation[J]. J Neurol, 2012,259:745-751.
64 Ntaios G, Lip GY, Makaritsis K, et al. CHADS2,CHA2DS2_VASc, and long-term stroke outcome in patients without atrial fibrillation[J]. Neurology, 2013,80:1009-1017.
65 Saposnik G, Kapral MK, Liu Y, et al. iScore:A risk score to predict death early after hospitalization for an acute ischemic stroke[J]. Circulation, 2011, 123:739-749.
66 Saposnik G, Raptis S, Kapral MK, et al. The iScore predicts poor functional outcomes early after hospitalization for an acute ischemic stroke[J]. Stroke,2011, 42:3421-3428.
67 Saposnik G, Demchuk A, Tu JV, et al. The iScore predicts efficacy and risk of bleeding in the national institute of neurological disorders and stroke tissue plasminogen activator stroke trial[J]. J Stroke Cerebrovasc Dis, 2012, 22:876-882.
68 Saposnik G, Fang J, Kapral MK, et al. The iScore predicts effectiveness of thrombolytic therapy for acute ischemic stroke[J]. Stroke, 2012, 43:1315-1322.69 O'Donnell MJ, Fang J, D'Uva C, et al. The PLAN score:A bedside prediction rule for death and severe disability following acute ischemic stroke[J]. Arch Intern Med, 2012, 172:1548-1556.
70 Smith EE, Shobha N, Dai D, et al. Risk score for in-hospital ischemic stroke mortality derived and validated within the get with the guidelines-stroke program[J]. Circulation, 2010, 122:1496-1504.
71 Ntaios G, Faouzi M, Ferrari J, et al. An integer-based score to predict functional outcome in acute ischemic stroke:The ASTRAL score[J]. Neurology, 2012,78:1916-1922.
72 Muscari A, Puddu GM, Santoro N, et al. A simple scoring system for outcome prediction of ischemic stroke[J]. Acta Neurol Scand, 2011, 124:334-342.
73 Ovbiagele B, Liebeskind DS, Kim D, et al. Prognostic value of Framingham cardiovascular risk score in hospitalized stroke patients[J]. J Stroke Cerebrovasc Dis, 2011, 20:222-226.
74 Huxley RR, Lopez FL, Folsom AR, et al. Absolute and attributable risks of atrial fibrillation in relation to optimal and borderline risk factors:The Atherosclerosis Risk In Communities (ARIC) study[J].Circulation, 2011, 123:1501-1508.
75 Yusuf S, Healey JS, Pogue J, et al. Irbesartan in patients with atrial fibrillation[J]. N Engl J Med, 2011,364:928-938.
【点睛】
本文介绍了心房颤动患者卒中风险、出血风险、预后等方面预测模型和评分系统的发展和现状。
