经椎弓根椎体截骨术治疗强直性脊柱炎后凸畸形术中大量出血的预测
2014-02-14郭鸿飞张永刚姚子明付君王景明杜建伟唐翔宇王岩
郭鸿飞 张永刚 姚子明 付君 王景明 杜建伟 唐翔宇 王岩
. 强直性脊柱炎 Ankylosing spondylitis .
经椎弓根椎体截骨术治疗强直性脊柱炎后凸畸形术中大量出血的预测
郭鸿飞 张永刚 姚子明 付君 王景明 杜建伟 唐翔宇 王岩
目的探讨经椎弓根椎体截骨术 ( pedicle subtraction osteotomy,PSO ) 治疗强直性脊柱炎( ankylosing spondylitis,AS ) 后凸畸形术中大量出血 ( massive blood loss,MBL ) 的预测因素。方法共收集147 例 PSO 治疗 AS 后凸畸形的病例数据。其中 106 例资料完整,分为两组:A 组 ( n=69 ) 术中出血量≥估计血容量的 30%,B 组 ( n=37 ) 术中出血量<估计血容量的 30%。比较两组患者术前数据,应用单因素分析大量出血所有可能的预测因素。应用多因素 Logitic 回归分析大量出血的独立危险因素。应用 Pearson 相关性检验分析全部 106 例大量出血的发生率与脊柱外科医生 PSO 手术积累量的关系。结果A 组患者 ( 65% ) 中,GK 角 ≥70°、固定节段数 ≥9、双节段截骨的例数比 B 组 ( 35% ) 更多。Logistic 回归分析显示固定节段数 ≥9以及双节段截骨是大量出血的独立危险因素。Pearson 相关性分析显示在一定范围内,大量出血的发生率随着脊柱外科医生 PSO 手术积累量的增加而下降,二者呈线性相关。结论PSO 手术治疗 AS 后凸畸形的患者中,大量出血的发生率为 65%。术前 GK 角 ≥70°、双节段 PSO 截骨以及固定节段数 ≥9 是大量出血的预测因素,后两者是独立预测因素。在一定范围内,随着脊柱外科医生 PSO 手术量的积累,大量出血的发生率下降。
脊柱炎,强直性;失血,手术;椎体后凸成形术;矫形外科手术;经椎弓根椎体截骨术
强直性脊柱炎 ( ankylosing spondylitis,AS ) 是一种常见的风湿免疫性疾病,可导致典型的脊柱畸形,如腰椎前凸消失、胸椎驼背畸形以及胸腰段后凸畸形[1]。疾病后期可产生严重的胸腰段后凸畸形,导致矢状面失平衡以及平视能力下降[2]。脊柱截骨术能够矫正畸形,恢复矢状面序列并改善平视能力[3-4]。然而有文献报道脊柱截骨术治疗脊柱后凸畸形可导致严重的出血[5]。大量出血 ( massive blood loss,MBL ) 增加治疗费用并可导致许多相关并发症[6-9]。2011 年,Arun 等[10]报道 1 例 AS 患者在矫正畸形的过程中损伤主动脉,发生的灾难性地出血。因此,在术前预测术中大量出血对于治疗有很大意义。
尽管有一些文献报道了脊柱内固定术中的出血情况[5,10],但是关于经椎弓根椎体截骨术 ( pedicle subtraction osteotomy,PSO ) 治疗 AS 术中大量出血预测因素的研究却很少[11]。考虑到本科室 PSO 手术大量出血的发生率比其它手术更高,以及围手术期血液管理的重要性,笔者进行本研究,在术前评估术中大量出血的预测因素,为术者、麻醉医生、输血医生提供预警。
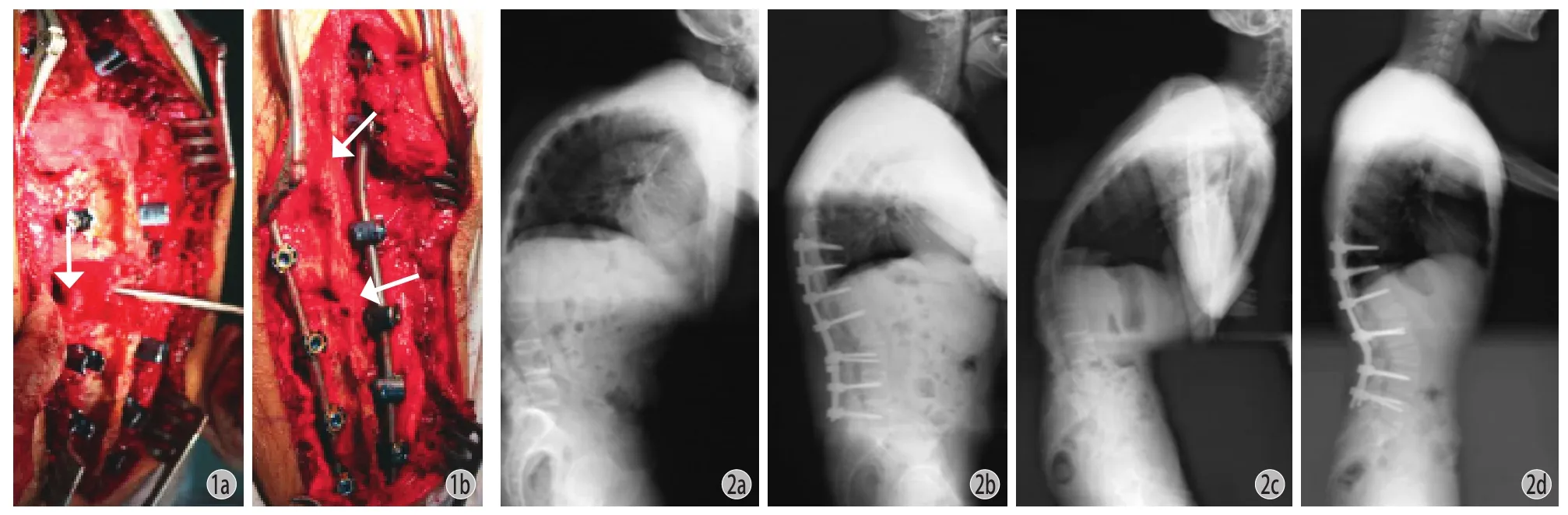
图1 术中照片 a:推入椎体后皮质前 ( 箭头所示 );b:闭合截骨处后 ( 箭头所示 )图 2 a~b:为 AS 后凸畸形患者术前术后侧位平片,于 L2行单节段 PSO 矫形术;c~d:为双节段截骨,于 L1、L3行 PSO 矫形术Fig.1 Intraoperative photographs a: Before the posterior cortex was pushed down ( arrow ); b: After the osteotomy was closed ( arrow )Fig.2 a-b: The preoperative and postoperative lateral radiographs respectively of an AS patient with spinal kyphosis, who underwent singlesegment PSO on L2; c-d: The preoperative and postoperative lateral radiographs respectively of an AS patient with spinal kyphosis, who underwent double-segment PSO on L1and L3
资料与方法
一、一般资料
回顾性研究 2003 年 1 月至 2014 年 1 月,我院行 PSO 矫形术的 147 例 AS 后凸畸形患者资料。其中 106 例资料完整,男 94 例,女 12 例,平均年龄( 36.3±9.3 ) ( 18~65 ) 岁。全部患者符合 1984 年修订的纽约标准[12]。患者由于严重的后凸畸形而无法平躺。全部 147 例手术均由笔者之一主刀完成。
患有高血压患者术前血压控制在 140 / 90 mm Hg以下。术前 3 个月停止除非甾体类抗炎药的其它药物治疗,吸烟者戒烟。排除行颈胸段畸形手术以及翻修手术的患者。
二、手术方法
全麻后将患者俯卧置于弓形手术台,腹部悬空。取后正中切口,骨膜下剥离显露后部结构,侧方尽可能显露至横突。按照术前计划,在将行截骨的椎体上下 2 个或 3 个节段置入椎弓根螺钉。使用刮匙去除椎体内松质骨形成空腔,仔细清除两侧皮质。随后将后皮质向下推入椎体。如果须行双节段截骨,在另一截骨节段进行相同操作。用巾钳夹住头尾两侧棘突,逐渐伸展手术台闭合截骨平面 ( 图 1 )。确认神经根无压迫后,将椎弓根螺钉锁死。手术全程由体感诱发电位 ( somatosensory evoked potential,SEP ) 及运动诱发电位 ( motor evoked potential,MEP ) 检测脊髓功能。
是否行双节段截骨取决于恢复矢状面平衡所需的矫正角度。单节段 PSO 截骨能够矫正 30°~40°,如需矫正更大角度,则行双节段 PSO 截骨[13]。在L3或附近椎体行第一处 PSO 截骨,第二处 PSO 截骨选择 T12或 L1,两处截骨节段之间至少保留一个椎体[14]。单节段和双节段 PSO 术前术后侧位平片如图 2 所示。
术中未使用凝血药,用双极电凝止住活动性出血,使用可吸收明胶海绵及骨蜡封堵软组织及骨表面渗血。术中心率控制在基础水平的 20% 以内,平均动脉压控制在 65~80 mm Hg。术中常规使用自体血回输。全部患者术中未损伤腹主动脉及其它大血管。
三、临床资料
查阅病历收集患者性别、年龄、体重、术前病程、血红蛋白、血小板计数、凝血酶原时间 ( PT )、活化部分凝血活酶时间 ( APTT )、国际标准化比值( INR )、纤维蛋白原、红细胞沉降率 ( ESR )、C 反应蛋白 ( CRP )、术前最大后凸角 ( global kyphosis,GK )、术后 GK 角、固定节段数、手术过程、手术时间、术中出血量、术后引流量以及术中输血量等资料。
术中出血量参照麻醉记录[15]。根据失血量≥估计血容量的 30% 需输血[16],将大量出血定义为术中出血量≥估计血容量的 30%,估计血容量按75 ml / kg ( 体重 ) 计算。
四、统计分析
使用 SPSS 19.0 统计学软件 ( SPSS 公司,美国 )对数据进行统计学分析。患者分入两组,A 组 ( 大量出血,术中出血量≥估计血容量的 30% ),B 组 ( 术中出血量<估计出血量的 30% )。应用 t 检验分析正态分布连续变量,应用 WilCoxon 秩和检验分析非正态分布连续变量,应用卡方检验分析分类变量。使用单因素分析筛选大量出血所有可能的预测因素。将 P 值<0.05 的变量纳入二分类 Logistic 回归分析以确定大量出血的独立预测因素。使用 Pearson 相关性检验分析全部 106 例患者大量出血发生率与手术积累量的关系。P 值<0.05 认为差异有统计学意义。
结 果
一、术前数据
A 组 69 例 ( 65% ),B 组 37 例 ( 35% )。两组中性别、年龄、体重、病程、血红蛋白、血小板计数、PT、APTT、INR、纤维蛋白原、CRP、ESR 差异无统计学意义 ( P>0.05 )。A 组中 GK 角≥70°、双节段截骨以及固定节段数≥9 的例数比 B 组更多( P<0.05 ) ( 表 1 )。
表1 两组术前变量比较 ( n = 106,±s )Tab.1 Comparison of the preoperative variables between the 2 groups ( n=106,±s )

表1 两组术前变量比较 ( n = 106,±s )Tab.1 Comparison of the preoperative variables between the 2 groups ( n=106,±s )
变量 A 组 ( n=69 ) B 组 ( n=37 ) P 值性别男62 32 0.60女7 5年龄 ( 岁 ) 36.7± 9.2 35.5± 9.6 0.54体重 ( kg ) 61.3±13.2 64.6±13.1 0.19病程 ( 年 ) 14.0 ( 10 ~ 20 ) 11.0 ( 7~16 ) 0.22血红蛋白 ( g / L ) 136.2±18.8 128.4±22.6 0.16血小板计数 253.0 ( 218.0 ~300.0 ) 241.0 ( 184.0 ~328.0 ) 0.57 PT ( s ) 16.2 ( 15.2 ~ 16.8 ) 16.3 ( 15.5 ~ 16.7 ) 0.68 APTT ( s ) 38.5 ( 35.3 ~ 42.2 ) 38.3 ( 33.8 ~ 40.7 ) 0.29 INR 1.0 ( 0.96~ 1.1 ) 1.0 ( 0.95~ 1.1 ) 0.62纤维蛋白原 ( mg / dl ) 3.8 ( 3.4 ~ 4.5 ) 3.9 ( 3.3 ~ 4.5 ) 0.72 ESR 16.0 ( 10.0 ~ 25.0 ) 10.0 ( 6.8 ~ 21.5 ) 0.06 CRP 1.6 ( 1.0 ~ 2.6 ) 1.6 ( 0.9 ~ 2.7 ) 0.98术前 GK ( ° )≥70 48 17 0.02<70 21 20截骨节段数单节段 24 30 <0.01双节段 45 7固定节段数≥9 27 6 0.01<9 42 31
二、术中、术后数据
平均术中出血量 2072.5 ( 600~5800 ) ml。估计血容量的 30%,A 组 ( 1379.7±296.7 ) ml,B 组 ( 1454.9±293.9 ) ml,差异无统计学意义 ( P>0.05 )。术中出血量,A 组 ( 2647.7±1060.3 ) ml,B 组 ( 1000.0±273.9 ) ml ( P<0.05 )。
A 组患者手术时间更长,术中自体血回输、输新鲜冰冻血浆以及同种异体红细胞量更多 ( P<0.05 )。两组术后 GK 改变角度、GK 改变率以及术后引流量差异无统计学意义 ( P>0.05 ) ( 表 2 )。
表2 两组术中、术后结果比较 ( n = 106,±s )Tab.2 Comparison of the intraoperative and postoperative results between the 2 groups ( n=106,±s )

表2 两组术中、术后结果比较 ( n = 106,±s )Tab.2 Comparison of the intraoperative and postoperative results between the 2 groups ( n=106,±s )
变量 A 组 ( n=69 ) B 组 ( n=37 ) P 值手术时间 ( h ) 6.5± 1.4 5.4± 1.3 <0.01自体红细胞 ( ml ) 1062.3±815.1 434.4±225.6 <0.01同种异体 ( ml ) 1011.4±455.5 619.4±172.5 <0.01新鲜冷冻血浆 ( ml ) 531.7±278.6 347.5±113.6 <0.01 GK 改变角度 ( ° ) 54.9± 18.6 52.1± 14.3 0.41 GK 改变率 0.71 ( 0.66~0.76 )0.77 ( 0.70~0.84 ) 0.16术后引流量 878.8±440.8 897.5±481.7 0.89
三、Logiscic 回归分析
二分类 Logistic 回归分析结果列于表 3 中,结果显示双节段截骨 ( OR 8.47,95% CI 2.95~24.28 )以及固定节段数≥9 ( OR 3.57,95% CI 1.19~10.73 )是大量出血的独立预测因素。术前 GK 角≥70°不是术中大量出血的独立预测因素 ( OR 0.97,95% CI 0.36~2.63 )。
四、Pearson 相关性检验
使用 Pearson 相关性检验分析 106 例患者大量出血发生率与脊柱外科医生 PSO 手术积累量的关系。结果显示在一定范围内,随着 PSO 手术积累量的增加,大量出血的发生率呈下降趋势 ( P<0.01,Pearson 相关系数=-0.80 ) ( 图 3 )。

表3 大量出血术前变量的二分类 Logistic 回归分析结果 ( n = 106 )Tab.3 Results of the binary Logistic regression analysis for the preoperative variables ( n=106 )
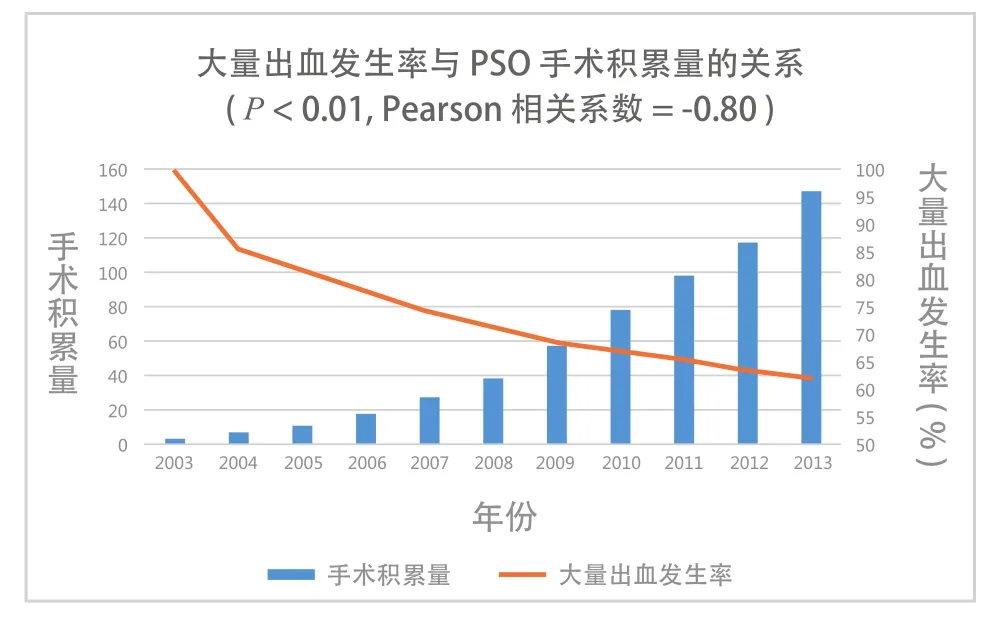
图3 应用 Pearson 相关性检验分析大量出血发生率与 PSO 手术积累量的关系Fig.3 The relationship between the incidence of MBL and the cumulative amount of PSO analyzed with the Pearson correlation test
讨 论
脊柱手术出血量受很多因素影响,确定大量出血的预测因素有一定难度[6,17-18]。对于 AS 后凸畸形患者的截骨矫形,我们仅进行一次手术。考虑到各中心拔除引流管的标准各不相同,本研究仅计患者的术中出血量而非总出血量[17-20]。为了更有效地进行血液管理,既往有研究探索脊柱内固定手术出血的预测因素[6,18]。然而,要确定患者是否确实需要输血有很大难度。而且既往的研究没有考虑到不同中心的输血适应证不同。因而需要更加客观、可行的研究探讨术中出血的预测因素。
单因素分析显示更大的 GK 角 ( ≥70° )、双节段截骨、更多的固定节段 ( ≥9 ) 是 PSO 治疗 AS 后凸畸形术中大量出血的预测因素。另外,两组患者输自体红细胞、异体红细胞、新鲜冰冻血浆量不同,说明大量出血患者更有可能需要术中输血。
应用 Logistic 回归分析可以确定独立危险因素。将单因素分析中有意义的变量纳入 Logistic 回归分析中以排除假阳性因素。结果显示双节段截骨以及更多的固定节段数 ( ≥9 ) 是大量出血的独立预测因素。Logistic 回归分析中 OR 值确定各个预测因素的相对重要性。
本研究结果显示行双节段截骨的患者术中大量出血的可能性是行单节段截骨患者的 8.47 倍。既往研究[13,21]也报道双节段截骨出血量大于单节段截骨。由于需行椎体截骨,出血往往来自于椎体本身[22]。双节段 PSO 术中截骨量更多、截骨面暴露面积更大,椎体静脉破裂导致出血量增多,有时出血甚至难以控制。
固定节段数≥9 是大量出血另一个独立预测因素。Yu 等[20]报道了固定节段数与脊柱侧凸手术出血相关。固定节段越多,脊柱暴露的就越多,需要剥离更多的肌肉,导致活动性出血,并增加软组织及椎体暴露面的渗血。本研究表明固定节段数≥9时大量出血的风险增加 3.57 倍,说明术前计划的固定节段数能够很好地预测 PSO 术中出血。
尽管有学者报道术前 GK 角是脊柱侧凸患者术中大量出血的独立预测因素,但是本研究显示术前GK 角并不是 AS 患者 PSO 术中大量出血的独立预测因素[20,23]。原因可能是术前 GK 角越大,术中需要截骨、固定的节段就越多。术后 GK 改变角度以及改变率对于大量出血没有影响 ( P<0.05 )。
AS 是一种炎症性疾病,患者常表现为炎症指标异常[24],我们考虑 ESR 和 CRP 可能会是大量出血的预测因素,不过两组中这两项指标差异并无统计学意义。术前凝血功能指标也不是大量出血的预测因素。我们认为这些指标与有意义的因素相比作用比较小。
另外,随着脊柱外科医生 PSO 手术量的增加,大量出血的发生率在下降。这表明术者的经验是至关重要的。根据我们的经验,推入后皮质时出血最严重。所以行双节段 PSO 截骨时,我们更愿意先保留后皮质,并在完成第一处截骨后用无菌纱布填塞空腔,完成第二处截骨再推入两处截骨处的后皮质。熟练的手术技巧会缩短手术时间。而缩短手术时间,尤其是闭合截骨面的时间对于减少出血非常重要。 术者早期进行的 PSO 手术曾有记录 5000 ml以上的出血,近年来平均术中出血量呈下降趋势。以 2013 年为例,术者进行的单节段 PSO 术中平均出血量为 1410 ml,最少出血量为 600 ml;双节段 PSO术中平均出血量为 1923 ml,最少出血量为 650 ml。
据我们所知,这是第一个探讨 PSO 治疗 AS 后凸畸形术中大量出血预测因素的研究。我们的研究也有一些不足。首先,这是一个回顾性观察研究,存在着不可避免的、无法控制的混杂因素以及潜在的信息偏倚。一些有意义变量可能没有纳入多因素模型中。其次,我们仅分析了通信作者为主刀医生的病例。为了更准确地预测 PSO 术中大量出血,应当进行多中心随机对照研究,确定广泛适用的预测因素。
总之,PSO 治疗 AS 后凸畸形发生术中大量出血的风险很大。术前 GK 角≥70°、双节段截骨、固定节段数≥9 是大量出血的预测因素,后两者是独立预测因素。在一定范围内,大量出血的发生率随着脊柱外科医生 PSO 手术积累量的增加而下降。
[1]Braun J, Sieper J. Ankylosing spondylitis. Lancet, 2007, 369(9570):1379-1390.
[2]Chang KW, Chen YY, Lin CC, et al. Closing wedge osteotomy versus opening wedge osteotomy In ankylosing spondylitis with thoracolumbar kyphotic deformity. Spine, 2005, 30(14): 1584-1593.
[3]Mac-Thiong JM, Transfeldt EE, Mehbod AA, et al. Can C7 plumbline and gravity line predict health related quality of life in adult scoliosis? Spine, 2009, 34(15):E519-527.
[4]Glassman SD, Bridwell K, Dimar JR, et al. The impact of positive sagittal balance in adult spinal deformity. Spine, 2005, 30(18):2024-2029.
[5]Willems KF, Slot GH, Anderson PG, et al. Spinal osteotomy in patients with ankylosing spondylitis: complications during first postoperative year. Spine, 2005, 30(1):101-107.
[6]Meert KL, Kannan S, Mooney JF. Predictors of red cell transfusion in children and adolescents undergoing spinal fusion surgery. Spine, 2002, 27(19):2137-2142.
[7]Sethna NF, Zurakowski D, Brustowicz RM, et al. Tranexamic acid reduces intraoperative blood loss in pediatric patients undergoing scoliosis surgery. Anesthesiology, 2005, 102(4): 727-732.
[8]Sachs B, Delacy D, Green J, et al. Recombinant activated factor VII in spinal surgery: a multicenter, randomized, double-blind, placebo-controlled, dose-escalation trial. Spine, 2007, 32(21): 2285-2293.
[9]Dodd RY, Notari EP 4th, Stramer SL. Current prevalence and incidence of infectious disease markers and estimated windowperiod risk in the American Red Cross blood donor population. Transfusion, 2002, 42(8):975-979.
[10]Arun R, Dabke HV, Mehdian H. Comparison of three types of lumbar osteotomy for ankylosing spondylitis: a case series and evolution of a safe technique for instrumented reduction. Eur Spine J, 2011, 20(12):2252-2260.
[11]刘兴勇, 钱邦平, 邱勇. 经椎弓根椎体截骨术治疗强直性脊柱炎胸腰椎后凸畸形术中出血情况的分析. 中国脊柱脊髓杂志, 2013, 23(8):690-693.
[12]van der Linden S, Valkenburg HA, Cats A. Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum, 1984, 27(4):361-368.
[13]Zhang HQ, Huang J, Guo CF, et al. Two-level pedicle subtraction osteotomy for severe thoracolumbar kyphotic deformity in ankylosing spondylitis. Euro Spine J, 2014, 23(1): 234-241.
[14]Song K, Zheng GQ, Zhang YG, et al. A new method for calculating the exact angle required for spinal osteotomy. Spine, 2013, 38(10):E616-620.
[15]Bose P, Regan F, Paterson-Brown S. Improving the accuracy of estimated blood loss at obstetric haemorrhage using clinical reconstructions. BJOG, 2006, 113(8):919-924.
[16]Miller RD, Eriksson LI, Fleisher LA, et al. Miller’s Anesthesia. 7th edn. Amsterdam: Churchill Living stone, 2009: 1744-1745.
[17]Lenoir B, Merckx P, Paugam-Burtz C, et al. Individual probability of allogeneic erythrocyte transfusion in elective spine surgery: the predictive model of transfusion in spine surgery. Anesthesiology, 2009, 110(5):1050-1060.
[18]Nuttall GA, Horlocker TT, Santrach PJ, et al. Predictors of blood transfusions in spinal instrumentation and fusion surgery. Spine, 2000, 25(5):596-601.
[19]Zheng F, Cammisa FP Jr, Sandhu HS, et al. Factors predicting hospital stay, operative time, blood loss, and transfusion in patients undergoing revision posterior lumbar spine decompression, fusion, and segmental instrumentation. Spine, 2002, 27(8):818-824.
[20]Yu X, Xiao H, Wang R, et al. Prediction of massive blood loss in scoliosis surgery from preoperative variables. Spine, 2013, 38(4):350-355.
[21]宋若先, 张永刚, 张雪松, 等. 跳跃式经椎弓根椎体截骨术矫治强直性脊柱炎重度后凸畸形的疗效. 中华医学杂志, 2012, 92(21):1476-1480.
[22]Wang Y, Zhang Y, Mao K, et al. Transpedicular bivertebrae wedge osteotomy and discectomy in lumbar spine for severe ankylosing spondylitis. J Spinal Disord Tech, 2010, 23(3): 186-191.
[23]Hassan N, Halanski M, Wincek J, et al. Blood management in pediatric spinal deformity surgery: review of a 2-year experience. Transfusion, 2011, 51(10):2133-2141.
[24]Bond D. Ankylosing spondylitis: diagnosis and management. Nurs Stand, 2013, 28(16-18):52-59.
( 本文编辑:王永刚 )
Predictors of massive blood loss in pedicle subtraction osteotomy for ankylosing spondylitis kyphosis
GUO Hong-fei, ZHANG Yong-gang, YAO Zi-ming, FU Jun, WANG Jing-ming, DU Jian-wei, TANG Xiang-yu, WANG Yan. Department of Orthopedics, Chinese PLA General Hospital, Beijing, 100853, PRC
ObjectiveTo investigate the predictors of massive blood loss ( MBL ) in pedicle subtraction osteotomy ( PSO ) in the treatment of spinal kyphosis caused by ankylosing spondylitis ( AS ).MethodsA total of 147 patients with spinal kyphosis caused by AS underwent PSO, whose clinical data were collected. Among them, the data of 106 patients were complete, who were divided into 2 groups. In group A ( n=69 ) the intraoperative blood loss was more than or equal to 30% of the estimated blood volume, and in group B ( n=37 ) the intraoperative blood loss was less than 30% of the estimated blood volume. The preoperative data were compared between the 2 groups, and univariate analysis was undertaken to distinguish all the possible predictors of MBL. And a binary logistic regression analysis was used to determine the independent risk factors of MBL. The relationship between the incidence of MBL in all the 106 cases and the cumulative amount of PSO by spine surgeons was analyzed with the Pearson correlation test.ResultsThere were more cases of double-segment osteotomy in group A ( 65% ) than in group B ( 35% ), with the global kyphosis ( GK ) ≥70° and the number of fxation segments ≥9. Logistic regression analysis showed that more than or equal to 9 fxation segments and double-segment osteotomy were independent risk factors for MBL. The Pearson correlation test showed that the incidence of MBL was decreased with the increase of the cumulative amount of PSO by spine surgeons in a certain range and a linear correlation was found between them.ConclusionsWhen PSO is performed in the treatment of spinal kyphosis caused by AS, the incidence of MBL is 65%. The predictors of MBL included the preoperative Cobb’s angle ≥70°, double-segment PSO and number of fxation segments ≥9, and the last 2 predictors are independent. In a certain range, with the increase of the cumulative amount of PSO by spine surgeons, the incidence of MBL will be decreased.
Spondylitis, ankylosing; Blood loss, surgical; Kyphoplasty; Orthopedic procedures; Pedicle subtraction osteotomy
10.3969/j.issn.2095-252X.2014.10.007
R681.5, R682.3
100853 北京,解放军总医院骨科
张永刚,Email: zhangyg301@hotmail.com
2014-07-17 )