Primary Endodermal Sinus Tumor in the Posterior Cranial Fossa:Clinical Analysis of 7 Cases
2013-11-18MingchaoFanPengSunDongliangLinYiYuWeichengYaoYugongFengandLiminTang
Ming-chao Fan,Peng Sun,Dong-liang Lin,Yi Yu,Wei-cheng Yao,Yu-gong Feng,and Li-min Tang*
1Department of Neurosurgery,2Department of Pathology,3Department of Radiology,the Affiliated Hospital of Medical College,Qingdao University,Qingdao,Shandong 266003,China
ENDODERMAL sinus tumor (EST),also known as yolk sac tumor,is a rare malignant germ cell tumor.These tumors originate mainly from the gonads,and only about 10%-20% occur in the extragonadal sites.ESTs account for only 5%-7% of intracranial germ cell tumors.Germ cell tumors comprise about 1% of all primary brain tumors in adults,and 3%-8%of all primary brain tumors in children.1The pineal or suprasellar regions are the usually locations of primary intracranial EST.2,3EST arising in the posterior cranial fossa is especially uncommon.The clinical manifestations and therapeutic strategy of this tumor in the posterior cranial fossa need to be identified.This study aimed to illustrate the clinical characteristics,management considerations and outcomes of the EST in the posterior cranial fossa.
PATIENTS AND METHODS
A systematic Medline and PubMed database search was performed (up to February 5,2013).The following key words were used to search English literatures of interest:[endodermal sinus tumor OR yolk sac tumor]AND [posterior cranial fossa OR cerebellum].One case in our hospital was described.Those cases from retrieved papers and our hospital were analyzed.The following information was recorded:age,gender,symptom,nationality,pathological features,management methods and outcomes.Both the specific tumor marker and alpha-fetoprotein (AFP) were used to identify the neoplasm.
RESULTS
Description of our case
A 4-year-old boy with an intermittent headache for 2 months was admitted to our hospital in November 2007.Ocular ataxia and defective coordination were found during physical examination on admission.Magnetic resonance imaging (MRI) routine scanning revealed a miscellaneous cystic lesion in the right cerebellar hemisphere.The signal intensity of lesions was long-T1 and long-T2.The lesion size was 32.6 mm×43.6 mm×25.5 mm.The nodules which signal intensity was slightly long-T1 and long-T2 on MRI,were found in the cyst (Fig.1).The pre-operative diagnosis was medulloblastoma.
A suboccipital craniotomy was performed.During operation,we found that the tumor was composed of both solid and cystic components with a copious blood supply.The tumor had a sharp border of demarcation with the normal parenchyma.The cut surface was kermesinus in color.The tumor was completely removed.
The specimen was processed and stained with Haematoxylin &Eosin (H&E) staining.Upon histopathological examination,the tumor mainly consisted of proliferating tubules and solid sheets of tumor cells in a loose,reticular stroma.Papillary structures that consisted of columnar cells covering the centrally situated blood vessels (Schiller-Duval body) were also found (Fig.2A).Immunohistochemical staining revealed the tumor cells were positive for AFP (Fig.2B) and AE1/AE3 (Fig.2C),leading to the final diagnosis of pure EST.
The postoperative course was uneventful.Head CT scan was performed and showed no residual tumor.One and a half months after operation,the boy underwent systemic chemotherapy with cisplatin,vincristine and bleomycin every one month.The serum AFP level was decreased from 1158.1 ng/ml to 2.3 ng/ml after the fourth circle of chemotherapy.The chemotherapy was suspended after the fifth circle.The tumor recurred in the same place at the third year after surgery.And the serum AFP level was increased to 3572.9 ng/ml.His parents rejected to surgery again,so he underwent local radiotherapy and system chemotherapy.Radiotherapy to the tumor site was initiated with a dose of 40 Gy.He died at the fifth year after surgery because of acute hydrocrania.
Characteristics of primary EST in the posterior cranial fossa

Figure 1.Cross-sectional magnetic resonance imaging routine scanning reveals an inordinate miscellaneous cystoid lesion (arrows) in the right cerebellar hemisphere.
There were only seven cases of primary ESTs located in the posterior cranial fossa,including six cases searched from the PubMed2-7and one case from our hospital (Table 1).Six were boy and one patient’s gender was not available from the report.Ages ranged from 1 to 5 (mean 3.14)years.The most common symptoms and signs at presentation were headache and vomiting,followed by ataxia,cranial nerve dysfunction and deteriorated mental status.The duration of clinical history ranged from 3 days to 2 months (mean 1.3 months).The mean size of tumor of this series was 4.4 cm.The locations of these neoplasms were different.ESTs of four cases originated from the cerebellar hemisphere,two cases from the cerebellar vermis,and only one case from the pontocerebellar angle.Only one case was reported in Italy.There were four cases in Japan.Six of seven cases came from East Asia.All patients underwent craniotomy.The masses were totally removed in six cases and partially resected in one case.Systemic chemotherapy was performed for all seven patients.Only two patients underwent radiotherapy when the tumors relapsed.Histological examination showed Schiller-Duval bodies in all seven neoplasms.All seven tumors were AFP positive.AE1/AE3 was detected in two cases.The AFP level in serum was sky-high before therapy and depressed quickly after patients underwent chemotherapy.The mean follow-up period was 24.4 months (range 5-52 months).Four tumors recurred after removed totally.Three cases died including one whose tumor was partially removed.
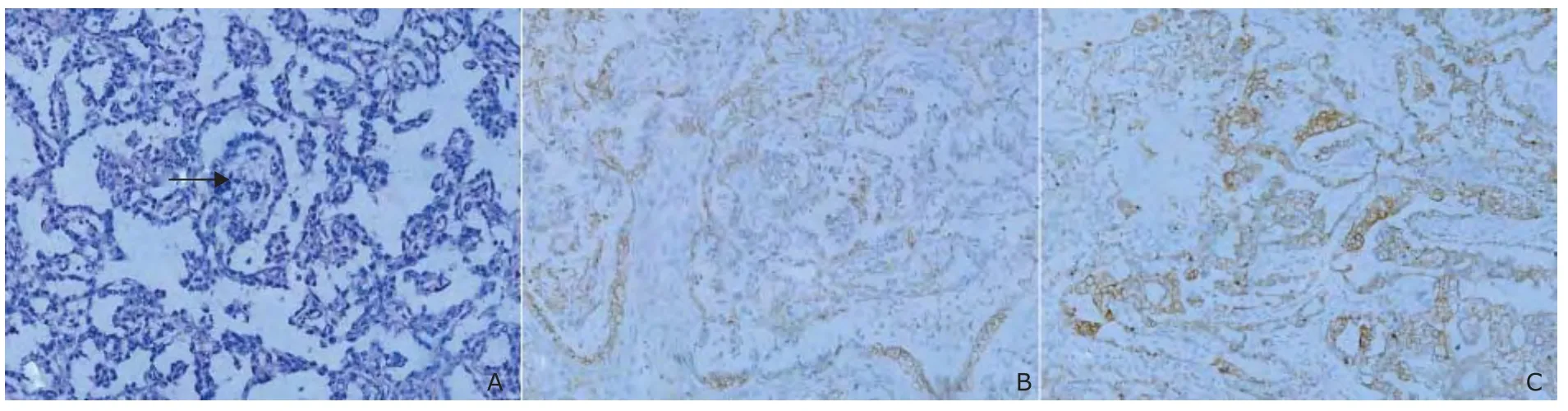
Figure 2.Histological and immunohistochemical pictures.×200

Table 1.Characteristics of seven patients having primary endodermal sinus tumor in the posterior cranial fossa
DISCUSSION
EST is a rare malignant germ cell tumor.Most of them originate from the gonads like ovary and testis.Less than 20% arise in the extragonadal sites,including the sacrococcygeal region,cervix,vulva,mediastinum,liver,omentum,face,retroperitoneum,prostate,and so on.3,6-8The central nervous system is the infrequent primary site of ESTs.Of the various central nervous system sites,EST is found to most frequently occur in the pineal or suprasellar regions,and often be combined with components of other germ cell tumors.The literatures on this neoplasm in the central nervous system are based on isolated case reports.EST rarely occurs in the posterior fossa.There were only 7 cases of the ESTs in the posterior cranial fossa.The sex preponderance was conspicuous,and almost all patients were boys.These boys were very young;the oldest one was only 5 years old.
The histogenesis of extragonadal EST still remains controversial.One hypothesis is that these tumors arise from primordial germ cells that have migrated improperly during embryonic development.9And another hypothesis is that these tumors arise from undifferentiated pluripotent embryomic or extraembryonic cells that have escaped the influence of primary developmental factors.3,4Both of them are unable to give enough evidence to support their opinion or refute the other side,so its nosopoietic mechanism is still unknown.
The diagnosis of EST is a challenge.The symptoms of EST are nonspecific,variably according to its location and extent of involvement.Circumscribed neuro-function absence and headache are the usual presenting symptom of intracranial EST.Histopathologic and immunohistochemical examination are the final methods to make a definite diagnosis of the EST.Schiller-Duval body is the specific structure of EST.The Schiller-Duval bodies were found in all 7 cases.The presence of the Schiller-Duval body is essential for EST in the posterior cranial fossa.On immunohistochemistry,EST is positive for AFP and AE1/AE3.AFP is originally discovered in embryonic hepatic tissue cells.The level of AFP in serum has been shown increase in the presence of EST elements.7High levels of AFP (>25 ng/ml) might be associated with EST.The serum level of AFP could as an index to assessing the response to therapy and detecting recurrence.In previous and our cases,the lesion was misdiagnosed as medulloblastoma,because the level of AFP was not checked before operation.The change of serum AFP level was well correlated with the tumor’s severity.
Generally,the poor prognosis of extragonadal intracranial EST is due to still no effective management methods.It is necessary to resection of the posterior cranial fossa EST,notwithstanding it could be removed totally or not.Surgical resection could restore the cerebrospinal fluid circulation and avoid the acute cerebral hernia.The effect of radiotherapy on intracranial EST is still debated.Radiotherapy is not the first choice for primary intracranial EST.Only 2 cases were treated by radiotherapy when the tumors relapsed.Chemotherapy is considered to be a useful therapy in controlling the tumor and prolonging survival.3-5The serum level of AFP of all 7 cases was decreased quickly after chemotherapy.A combination of operation and chemotherapy may be the effective management.
1.Macvanski M,Ristić-Balos D,Vasić B,et al.Intracranial yolk sac tumor in an adult patient:MRI,diffusion-weighted imaging and 1H MR spectroscopy features.Vojnosanit Pregl 2012;69:277-80.
2.Fujiwara T,Honjo Y,Nagao S,et al.Primary cerebellar yolk sac tumor:Case report.Surg Neurol 1994;42:121-4.
3.Cheon HC,Jung S,Moon KS,et al.Primary endodermal sinus tumor of the cerebellar hemisphere:A case report with review of the literature.J Neurooncol 2006;77:173-6.
4.Endo S,Kobayashi H,Terasaka S,et al.Primary intracranial yolk sac tumor in the posterior fossa:Case report of a child with Down syndrome.Clin Neurol Neurosurg 2013;115:811-3.
5.Nakase H,Ohnishi H,Touho H,et al.Cerebellar primary germ-cell in a young boy.Brain Dev 1994;16:396-8.
6.Lazzareschi I,Furfare IF,Coccia P,et al.Extragonadal yolk sac tumor outside of the midline of the body:A case report of a child with a yolk sac tumor of the pontocerebellar angle.Tumori 2009;95:840-2.
7.Tsukamoto H,Matsushima T,Shono S,et al.Primary yolk sac tumor of the cerebellar vermis:Case report.Surg Neurol 1992;38:50-6.
8.Geminiani ML,Panetta A,Pajetta V,et al.Endodermal sinus tumor of the omentum:Case report.Tumori 2005;91:563-6.
9.Mishra A,El-Naggar AK,DeMonte F,et al.Endodermal sinus tumor of the paranasal sinuses.Head Neck 2008;30:539-43.
杂志排行

Chinese Medical Sciences Journal的其它文章
- What Moved into the Lung? An Unusual Case of Foreign Body Migration
- Recurrent Seizures Manifestations in a Case of Congenital Hypoparathyroidism:a Case Report
- Mechanical Stimulus Inhibits the Growth of a Bone Tissue Model Cultured In Vitro△
- CORRECTION
- Coronary Artery Perforation Complicated With Acute Aortic Valve Regurgitation During Percutaneous Coronary Intervention:Report of Two Cases
- Reconstruction of the Medial Patellofemoral Ligament Using Hamstring Tendon Graft With Different Methods: a Biomechanical Study