Clinical features and treatment of sump syndrome following hepaticojejunostomy
2011-12-14GabrieleMarangoniAmirAliWalidFarajNigelHeatonandMohamedRela
Gabriele Marangoni, Amir Ali, Walid Faraj, Nigel Heaton and Mohamed Rela
London, UK
Clinical features and treatment of sump syndrome following hepaticojejunostomy
Gabriele Marangoni, Amir Ali, Walid Faraj, Nigel Heaton and Mohamed Rela
London, UK
(Hepatobiliary Pancreat Dis Int 2011; 10: 261-264)
biliary tract surgical procedures;biliary tract disease;septicemia
Introduction
The siphoning effect causing bile stasis, re fl ux of bilio-enteric contents into the common bile duct (CBD) and cholangitis without evidence of anastomotic stricture was originally described in choledochoduodenostomy and called "sump syndrome".[1]Sump syndrome has also been described as a rare complication of choledochojejunostomy and, more recently, hepaticojejunostomy.[2]Although not very common, it is a potentially life-threatening complication.The pathophysiology of the syndrome seems to differ whether we consider side-to-side and end-to-side choledochoduodenostomy or choledocho and hepaticojejunostomy.
Side-to-side choledochoduodenostomy was originally performed with the aim to achieve drainage of the CBD with low morbidity in high-risk patients. The segment of the CBD between the anastomosis and the ampulla of Vater acts as a reservoir of stagnant bile with concomitant formation of debris, stones and proliferation of bacteria that cause cholangitis, pancreatitis and hepatic abscesses.In end-to-side choledochoduodenostomy, enteric material re fl uxes into the biliary tree causing obstruction of the ducts and favouring the formation of stones and subsequent episodes of cholangitis.
Today, it is a standard practice to use Roux-en-Y hepaticojejunostomy as the method of biliary reconstruction due to the very low incidence of complications.[3]Ascending cholangitis is rare with this anastomosis and when it does occur the mechanism is different and could be related to a short Roux limb with re fl ux of food into the biliary tree and disturbance in intestinal motility.
We report 6 cases of sump syndrome after hepaticojejunostomy and discuss our experience in the light of the reported literature on this condition.
Methods
From 2001 to 2006, six patients (5 females and one male) with a mean age of 52 years (range 28-74), who had undergone an end-to-side hepaticojejunostomy,presented to our institution with episodes of biliary sepsis without evidence of anastomotic stricture. Biliary reconstruction was performed after laparoscopic cholecystectomy bile duct injury in 2 patients, after open cholecystectomy bile duct injury in 1, for biliary stricture after liver transplant in 1, for ischemic stricture 3 months after open cholecystectomy in 1, and as part of a pancreaticoduodenectomy procedure in 1. The fi rst episode of biliary sepsis was seen between 7 months and 36 years after hepaticojejunostomy. One patient developed a liver abscess which was later treated conservatively with drainage and appropriate antibiotic therapy. The number of signi fi cant episodes of cholangitis per patient(requiring hospitalization) ranged from one to nine. One patient required 3 months of intensive care due to biliary sepsis-induced multiple organ failure. The presence of anastomotic stricture was excluded with liver MRI/MRCP and percutaneous transhepatic cholangiogram (PTC). A scan of hepatobiliary imino diacetic acid (HIDA) was performed in 4 patients to assess hepatocyte excretion function and tracer/bile hold-up at the anastomosis.Diagnosis of sump syndrome was made with barium meal showing re fl ux of contrast into the biliary tree above the anastomosis (Fig. 1) and with PTC demonstrating blind loop or efferent loop stasis and retrograde re fl ux of contrast into the biliary tree (Fig. 2). On pre-operative imaging, three patients seemed to have a short jejunal Roux limb (less than 50 cm) and one had a distortion of the Roux loop at the level of the biliary anastomosis. The characteristics of the patients are listed in Table 1.
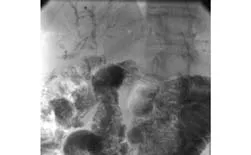
Fig. 1. Re fl ux of contrast into the bile tree on barium meal study.

Fig. 2. Stasis of contrast in the Roux loop on PTC.
Results
Five patients underwent surgery. Two underwent two operations and one was not considered amenable to surgery (Table 2).
One Tsuchida anti-re fl ux valve operation was performed with an uneventful hospital stay, but the patient continued to experience cholangitis and underwent lengthening of the Roux loop a year later.One patient had revision of a previously fashioned hepaticojejunostomy and concomitant lengthening of the Roux loop as there was a slight dilatation of the loop at the hepaticojejunostomy site. However, he subsequently needed further lengthening of the Roux loop to 100 cm 15 months after the fi rst operation due to ongoing cholangitic episodes and documented evidenceof re fl ux on barium meal. Three patients underwent lengthening of the Roux loop (70 cm) for a very short jejunal limb (20-40 cm). Of these, one had excision of a redundant blind end of the Roux loop and one had a redo end-to-side hepaticojejunostomy at the same time.

Table 1. Patients' characteristics

Table 2. Outcome of surgery
Time from diagnosis to surgery varied from one month to 1.5 years. In one case, the patient initially refused the surgical option and in another the patient was given time to recover from a prolonged intensive care stay following a life-threatening cholangitis.
Mean hospital stay was 7.6 days (range 6-10 days).Three patients have not experienced any more septic episodes 6, 36 and 60 months after surgery. One patient,despite surgery, continued to have recurrent episodes of cholangitis with documented re fl ux into the biliary tree and is currently on rotating antibiotics, having not experienced cholangitis for a year. One patient had three cholangitis episodes in 8 years following surgery.In this case, an MRCP showed some irregularity of the intrahepatic bile ducts, possibly suggesting features of cholangiopathy without strictures or dilatation of the efferent loop, and is treated conservatively at present. Patient 5, who had undergone two biliary reconstructions following bile duct injury, was not considered for surgical treatment as originally the injury was a high Bismuth type 4 injury and the second hepaticojejunostomy required three separate duct anastomoses (right anterior, right posterior and left ducts). In this case, the next step would have consisted of a major liver resection. Because of refusing further surgery and experiencing only minor episodes of cholangitis (without hospitalization), the patient is at present under follow-up and treated conservatively with rotating antibiotics. Should the septic episodes increase in frequency and severity, surgery will be reconsidered.

Fig. 3. Holding up of tracer at the Roux loop on HIDA scan.
Discussion
Cholangitis after biliary reconstructive surgery is a relatively common complication and its incidence following Roux-en-Y hepaticojejunostomy is considered to be around 10%.[3]Sepsis is often caused by biliary stasis due to anastomosis stricture or lithiasis at the level of the anastomosis, but a number of cases occur without anatomical evidence of obstruction.
MRCP and PTC are routinely used to exclude anastomotic strictures and PTC may also show abnormal stasis of contrast in the Roux loop. HIDA scan can also be used to assess stasis, holding-up and delay of clearance in the Roux loop (Fig. 3). Finally, barium meal shows re fl ux of contrast in the biliary tree with patent anastomoses and may suggest a short Roux loop.
An adequate length of the Roux loop is important in order to prevent re fl ux of gastro-intestinal contents into the biliary tree; 50 cm is traditionally considered suf fi cient, although this is debatable and in fact other surgeons believe that 70 cm should be considered more appropriate. In our series, 4 patients had a Roux loop of 40 cm or less. However, in spite of lengthening of the Roux or revision of the hepaticojejunostomy with a loop length of 70 cm or more, three of them (patients 2, 4 and 6) continued to experience episodes of cholangitis although hospitalization was not required, and one(patient 2) presented with evidence of persistent re fl ux on barium meal. One of these patients (patient 6) had evidence of ongoing re fl ux without evidence of stricture and further lengthening of the Roux loop has controlled bile sepsis so far (6 months follow-up). Stasis of bile in an excessively long blind end of the Roux loop could be another anatomical mechanism underlying biliary sepsis, but excision of the blind end and lengthening of the loop did not resolve the problem in our patient,similar to the report by Vrochides et al.[4]
Intestinal motility disorders may play an important role. Collard and Romagnoli[5]studied bile re fl ux in a group of patients who had undergone a variety of Roux loop reconstructions and suggested that isolation of a bowel segment from the duodenum with division of one or two vascular pedicles in the mesentery disturbs intestinal motility.
Ducrotte et al[6]found that whilst the duodenal motility was normal, the motility of the limb and jejunum below the jejunojejunostomy resulted in motor abnormalities that could promote bacterial overgrowth and sepsis. Most of the abnormalities are ascribed to the presence of accessory pacemakers in the Roux loop no longer controlled by the main intestinal duodenal pacemaker.[7]
When the Roux loop seems correctly fashioned,Orlando et al[8]suggested the creation of a Tsuchida antire fl ux valve as previously described by Nakajo et al[9]in porto-enterostomy (Kasai surgery). The valve is fashioned by removing the seromuscular layers of the jejunal loop for a distance of about 2 cm and invaginating this area into the proximal jejunum. We performed a Tsuchida procedure in a patient (patient 1)who had a normal Roux loop length, without the same effectiveness in preventing cholangitis. Lengthening the Roux loop one year later to 70 cm achieved a better result and the patient is currently cholangitis-free 5 years after surgery.
In conclusion, despite its rarity, sump syndrome following hepaticojejunostomy is a clinical entity likely to be encountered in a specialist center. Patients can be quite symptomatic and occasionally present with life-threatening cholangitis. Surgical correction of an inadequately constructed Roux loop may successfully manage this complication, but cholangitis can recur despite appropriate reconstructive or antire fl ux surgery.Although it is dif fi cult to make recommendations due to the small number of cases, these episodes following surgery seem to be less frequent and less severe. In the dif fi cult cases, life-long rotating antibiotics (4 weeks cipro fl oxacin 500 mg bd alternating with 4 weeks amoxicillin 500 mg tds) and supportive treatment of the cholangitic episode are the only available measures.
Funding: None.
Ethical approval: Not needed.
Contributors: RM proposed the study. MG wrote the fi rst draft and analyzed data. AA and FW collected data and performed literature search. HN and RM revised the manuscript. All authors contributed to the design and interpretation of the study and to further drafts.RM is the guarantor.
Competing interest: No bene fi ts in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
1 Jones SA. The prevention and treatment of recurrent bile duct stones by transduodenal sphincteroplasty. World J Surg 1978;2:473-485.
2 Morrissey PE, Burns GA, Cohn SM. Sump syndrome complicating Roux-en-Y hepaticojejunostomy: case report and review of the literature. Surgery 1996;119:403-405.
3 Bismuth H, Franco D, Corlette MB, Hepp J. Long term results of Roux-en-Y hepaticojejunostomy. Surg Gynecol Obstet 1978;146:161-167.
4 Vrochides D, Fischer SA, Soares G, Morrissey PE. Successful treatment of recurrent cholangitis complicating liver transplantation by Roux-en-Y limb lengthening. Transpl Infect Dis 2007;9:327-331.
5 Collard JM, Romagnoli R. Roux-en-Y jejunal loop and bile re fl ux. Am J Surg 2000;179:298-303.
6 Ducrotte P, Peillon C, Guillemot F, Testart J, Denis P. Could recurrent cholangitis after Roux-en-Y hepaticojejunostomy be explained by motor intestinal anomalies? A manometric study. Am J Gastroenterol 1991;86:1255-1258.
7 Karlstrom LH, Soper NJ, Kelly KA, Phillips SF. Ectopic jejunal pacemakers and enterogastric re fl ux after Roux gastrectomy:effect of intestinal pacing. Surgery 1989;106:486-495.
8 Orlando G, Blairvacq JS, Otte JB, Goffette P, Ciccarelli O, Sempoux C, et al. Successful treatment of recurrent cholangitis after adult liver transplantation with a Tsuchida antire fl ux valve. Transplantation 2004;77:1307-1308.
9 Nakajo T, Hashizume K, Saeki M, Tsuchida Y. Intussusceptiontype antire fl ux valve in the Roux-en-Y loop to prevent ascending cholangitis after hepatic portojejunostomy. J Pediatr Surg 1990;25:311-314.
BACKGROUND: Cholangitis after Roux-en-Y hepaticojejunostomy is usually caused by anastomotic stricture. A small number of cases present without evidence of obstruction and are ascribed to re fl ux of gastro-intestinal content into the biliary tree above the anastomosis (sump syndrome). Despite prophylactic rotating antibiotic therapy, the cholangitic episode may be severe and life-threatening.
METHODS: From 2001 to 2006, six patients who had undergone an end-to-side hepaticojejunostomy presented to our institution with recurrent episodes of biliary sepsis. Anastomotic stricture was excluded by liver MRI/MRCP and percutaneous transhepatic cholangiogram (PTC). Barium meal showed re fl ux of contrast into the biliary tree in all patients. Three patients had a short jejunal Roux limb (less than 50 cm) on pre-operative imaging.
RESULTS: Five patients underwent surgery and two of them had two operations. One patient had a Tsuchida antire fl ux valve and subsequently underwent lengthening of the Roux loop. Three patients had lengthening of the Roux loop; one underwent re-do hepaticojejunostomy and one had concomitant revision of the hepaticojejunostomy and lengthening of the Roux loop. The latter underwent further lengthening of the Roux loop. Three patients are cholangitisfree 6, 36 and 60 months after surgery; two still experience mild episodes of cholangitis.
CONCLUSIONS: An adequate length of the Roux loop is important to prevent re fl ux. However, Roux loop lengthening to 70 cm or more does not always resolve the problem and cholangitis, although generally less frequent and severe,may recur despite appropriate reconstructive or antire fl ux surgery. In these cases, life-long rotating antibiotics is the only available measure.
Author Af fi liations: King's College London School of Medicine at King's College Hospital, Institute of Liver Studies, Denmark Hill, Camberwell,London SE5 9RS, UK (Marangoni G, Ali A, Faraj W, Heaton N and Rela M)
Gabriele Marangoni, MD FRCSEd (Gen Surg),Institute of Liver Studies, King's College Hospital, Denmark Hill, SE5 9RS,London, United Kingdom (Tel: +442032993672; Fax: +442032993575;Email: gabrielemarangoni@virgilio.it)
© 2011, Hepatobiliary Pancreat Dis Int. All rights reserved.
December 16, 2010
Accepted after revision February 8, 2011
杂志排行
Hepatobiliary & Pancreatic Diseases International的其它文章
- Dose requirement and complications of diluted and undiluted propofol for deep sedation in endoscopic retrograde cholangiopancreatography
- Current surgical management of pancreatic endocrine tumor liver metastases
- Borderline resectable pancreatic tumors: Is there a need for further re fi nement of this stage?
- Liver transplantation for hepatocellular carcinoma:an update
- Predictive value and main determinants of abnormal features of intraoperative cholangiography during cholecystectomy
- Emergency re-routing of anterior sector venous outflow for right lobe living donor liver transplantation including the middle hepatic vein