1990—2021年中国归因于饮食因素的缺血性心脏病疾病负担变化趋势及预测研究
2025-01-06吴霞张译匀姚承志赵湘铃熊文婧让蔚清

【摘要】 背景 缺血性心脏病(IHD)是导致中国居民疾病负担的第二大原因,饮食因素干预被认为是减少疾病负担有效及可行的措施。目的 分析1990—2021年中国归因于饮食因素的IHD疾病负担变化及未来变化趋势,以期为中国IHD的饮食防治提供参考。方法 提取2021年全球疾病负担(GBD 2021)数据库中1990—2021年中国、全球、不同社会人口指数(SDI)地区的归因于饮食因素的IHD疾病负担相关数据,应用Joinpoint模型计算年度变化百分比(APC)及平均年度变化百分比(AAPC),分析1990—2021年中国、全球、不同SDI地区归因于饮食因素的IHD疾病负担,中国不同性别、年龄人群归因于饮食因素的IHD疾病负担以及归因于不同类型饮食因素的IHD疾病负担。利用贝叶斯年龄时期队列(BAPC)模型预测2022—2031年中国归因于饮食因素的IHD标化死亡率、标化伤残调整寿命年(DALY)率变化趋势。结果 2021年中国归因于饮食因素的IHD标化死亡率为44.26/10万、标化DALY率为820.87/10万,与全球水平接近,高于高SDI地区,低于其余4类SDI地区。1990—2021年中国归因于饮食因素的IHD标化死亡率(AAPC=-0.17%,Plt;0.001)、标化DALY率(AAPC=-0.50%,Plt;0.001)与全球及五类SDI地区一致,均呈现下降趋势,全球下降幅度明显高于中国,高SDI地区下降速度最快。1990年与2021年中国男性归因于饮食因素的IHD疾病负担均高于女性;1990—2021年中国男性归因于饮食因素的IHD标化死亡率(AAPC=0.25%,Plt;0.001)呈上升趋势,女性标化死亡率(AAPC=-0.71%,Plt;0.001)、标化DALY率(AAPC=-1.23%,Plt;0.001)均呈下降趋势。1990与2021年中国归因于饮食因素的IHD疾病负担随着年龄增长呈上升趋势,≥70岁人群的死亡率、DALY率最高;1990—2021年50~69岁人群死亡率、DALY率呈下降趋势,而15~49岁、≥70岁人群呈上升趋势(Plt;0.001)。1990年与2021年归因于13种饮食因素的IHD标化死亡率、标化DALY率排名前两位的饮食因素均是钠摄入过量、全谷物摄入不足;1990—2021年标化死亡率、标化DALY率上升趋势较明显的是含糖饮料摄入过量、加工肉摄入过量、红肉摄入过量。BAPC模型显示,未来10年中国归因于饮食因素的IHD标化死亡率,标化DALY率均呈下降趋势。结论 1990—2021年中国归因于饮食因素的IHD标化死亡率、标化DALY率均呈下降趋势,但下降速度与高SDI地区相比差距较大,男性和老年人群负担较重,因此仍需重视IHD的饮食防控策略,加强宣传健康的膳食模式,倡导增加全谷物的摄入,减少钠盐、含糖饮料、加工肉、红肉的摄入,采取针对性措施进行有效干预以减轻其疾病负担。
【关键词】 心肌缺血;缺血性心脏病;全球疾病负担;饮食因素;趋势;预测
【中图分类号】 R 542.2 【文献标识码】 A DOI:10.12114/j.issn.1007-9572.2024.0253
Trend and Prediction of Changes in the Disease Burden of Diet-related Ischemic Heart Disease in China,1990-2021
WU Xia1,ZHANG Yiyun1,YAO Chengzhi1,ZHAO Xiangling1,XIONG Wenjing1,2,RANG Weiqing1*
1.School of Public Health,University of South China,Hengyang 421001,China
2.The First Affiliated Hospital of University of South China,Hengyang 421001,China
*Corresponding author:RANG Weiqing,Professor;E-mail:nhurwq@126.com
【Abstract】 Background Ischemic heart disease(IHD)is the second leading cause of disease burden in the Chinese population,and dietary factors are considered as effective and feasible approaches to reduce the disease burden. Objective To analyze the trends in the disease burden of IHD attributable to dietary factors from 1990 to 2021 and future trends in China,aiming to provide a reference basis for dietary prevention and treatment of IHD in China. Methods Data related to the disease burden of IHD attributable to dietary factors in China,worldwide,and regions with varied socio-demographic index(SDI)from 1990 to 2021 were extracted from the Global Burden of Disease 2021(GBD 2021)database. Using the Joinpoint model,the annual percent change(APC)and average annual percent change(AAPC)were calculated to analyze the disease burden of IHD attributable to dietary factors in China,worldwide,and regions with varied SDI. Furthermore,the model evaluated the diet-ralated disease burden by gender and age groups in China,as well as the burden of disease attributable to specific dietary factors within the Chinese population from 1990 to 2021. Additionally,the Bayesian age-period-cohort(BAPC)model was used to predict the standardized mortality rate and the standardized disability-adjusted life year(DALY)rate of IHD attributable to dietary factors from 2022 to 2031. Results In 2021,the standardized mortality rate and standardized DALY rate of IHD attributable to dietary factors in China were 44.26/100 000 and 820.87/100 000,respectively,which were close to the global levels,but higher than those of high SDI regions and lower than the remaining four categories of SDI regions. From 1990 to 2021,the standardized mortality rate(AAPC=-0.17%,Plt;0.001)and the standardized DALY rate(AAPC=-0.50%,Plt;0.001)of IHD attributable to dietary factors in China showed a decreased trend,which were consistent with the global trend and those in the five categories of SDI regions. The global decrease was significantly higher than that in China,with the fastest decrease in the high SDI regions. Disease burden of IHD attributable to dietary factors was significantly higher in Chinese males than in females in 1990 and 2021. The standardized mortality rate(AAPC=0.25%,Plt;0.001)of IHD attributable to dietary factors in Chinese males showed an increasing trend from 1990 to 2021. The standardized mortality rate(AAPC=-0.71%,Plt;0.001)and standardized DALY rate(AAPC=-1.23%,Plt;0.001)in Chinese females both showed a decreased trend. Disease burden of IHD attributable to dietary factors showed an increased trend with age in China in 1990 and 2021,and the highest mortality and DALY rate were detected in people ≥70 years old. The mortality and DALY rate of IHD attributable to dietary factors for the residents aged 50-69 years showed a decreased trend from 1990 to 2021,while those in the 15-49 years and ≥70 years showed an increased trend(Plt;0.001). Among the 13 dietary factors attributed to the standardized mortality and standardized DALY rate of IHD in 1990 and 2021,the top were excessive sodium intake and insufficient intake of whole grains. Dietary factors attributed to the most significant increased trends in the standardized mortality and standardized DALY rate of IHD from 1990 to 2021 were excessive intake of sugar-sweetened beverages,excessive intake of processed meats,and red meat intake. The BAPC model showed that the standardized mortality rate and standardized DALY rate of IHD attributable to dietary factors in China will decline over the next 10 years. Conclusion From 1990 to 2021,the standardized mortality and standardized DALY rate of IHD attributable to dietary factors decreased in China,but the decline is slower compared to high SDI regions. Disease burden of IHD attributable to dietary factors is heavier among men and the elderly. Therefore,it is essential to focus on dietary prevention and control strategies for IHD. Efforts should be made to promote healthy dietary patterns,increase the intake of whole grains,and reduce the consumption of sodium,sugar-sweetened beverages,processed meats,and red meats. Targeted measures and effective interventions are needed to further reduce the disease burden.
【Key words】 Myocardial ischemia;Ischemic heart diseases;Global Burden of Disease;Dietary factors;Trends;Forecasting
缺血性心脏病(ischemic heart disease,IHD)是指心肌血流量减少,导致心肌供氧和需氧不匹配为特征的疾病[1-2],是心血管疾病相关负担的主要原因[3]。世界卫生组织发布的世界卫生估计中指出,2000—2021年IHD是全球排名第一的致死病因,占世界总死亡人数的13%,是导致全球伤残调整寿命年(disability adjusted life years,DALY)损失的第二大病因[4],是全球面临的重要公共卫生问题。吸烟、饮酒、身体活动不足及不健康的饮食习惯等与IHD密切相关[5],可改变的饮食因素被认为是减少疾病负担有效及可行的手段。据全球疾病负担(Global Burden of Disease,GBD)数据库显示,2021年IHD是导致中国居民疾病负担的第二大原因,饮食因素导致中国居民IHD死亡和DALY的人群归因分值分别为41.07%和45.28%,饮食因素是中国IHD疾病负担主要的来源[6]。因此,本文通过GBD 2021数据库中国的相关数据,分析归因于饮食因素的疾病负担和变化趋势,预测未来10年的变化情况,旨在为中国IHD防治策略的制订提供参考依据。
1 资料与方法
1.1 资料来源
资料来源于GBD 2021(https://ghdx.healthdata.org/gbd-2021),包括1990—2021年全球204个国家和地区以及811个国家子地区的371种疾病及伤害的健康损失[6]、88种危险因素的归因疾病负担数据[7]。中国数据主要来自中国疾病监测系统和中国疾病预防控制中心等机构收集的死亡、癌症登记等数据。GBD 2021主要使用分层贝叶斯Meta回归建模工具DisMod-MR 2.1来估计1990—2021年的IHD的疾病负担[6],建模考虑了估计值误差,提供其95%不确定区间(95% uncertainty interval,95%UI)。本研究提取中国、全球和不同社会人口指数(socio demographic index,SDI)地区的归因于饮食因素的IHD疾病负担数据。年龄分组为15~49岁、50~69岁及≥70岁组。SDI是国家或地区发展状况的综合指标,由滞后分布的人均收入、平均受教育年限和25岁以下女性的生育率等数据综合评估得出,将204个国家或地区分为低、中低、中等、中高和高5个等级[8]。中国被划分在中等SDI地区[9]。GBD 2021根据《国际疾病分类》(ICD)第九版和第十版进行疾病分类编码,IHD疾病分类编码范围ICD-9中为410~414.9,ICD-10中为120~125.9[6]。
1.2 疾病负担指标
主要选择死亡和DALY的年龄标准化(简称标化)率为分析指标。其中DALY是一项目前评估疾病负担较为先进的综合评价指标之一,是指从发病到死亡所损失的全部健康寿命年[10],包括早死损失寿命年和伤残损失寿命年两部分。
1.3 统计学方法
使用Excel 2016对中国归因于饮食因素的IHD疾病负担指标按照不同年份、年龄、性别进行整理、绘图及统计分析。使用Joinpoint Regression Program 5.1.0软件计算中国1990—2021年归因于饮食因素的IHD标化死亡率、标化DALY率的年度变化百分比(annual percent change,APC)、平均年度变化百分比(average annual percent change,AAPC)及其95%置信区间(95% confidence interval,95%CI),检验水准α=0.05。Joinpoint模型是根据疾病的时间分布建立分段回归的方法,通过识别模型拐点将研究时间分割成不同区段,并对每个区段进行趋势拟合和优化,以描述疾病特异性的变化特征。模型公式为:
E(y|x)=β0+β1x+δ1(x-τ1)++…+δk(x-τk)+
其中x表示年份(1990—2021年);y表示归因于饮食因素的IHD标化死亡率、标化DALY率;β0、β1、δ是各个分段函数的回归系数;τ表示转折点;k代表连接点的个数,“+”表示:当 x-τk大于0时,(x-τk)+ = x-τk,若不满足条件(x-τk)+ 则被赋值为0。如果APCgt;0,表示该区段内指标上升,反之则下降;若AAPCgt;0,表示该指标逐年递增,反之则递减。如果APC或AAPC的95%CI包含0,则说明变化趋势无统计学意义。
利用R 4.2.1中BAPC包构建贝叶斯年龄时期队列(Bayesian age-period-cohort,BAPC)模型,对2022—2031年IHD归因于饮食因素的标化死亡率、标化DALY率进行预测。BAPC模型广泛用于预测不同类型的死亡率,其可以充分利用历史数据和先验信息提高参数估计准确性,得到稳健的预测结果。
2 结果
2.1 1990—2021年中国归因于饮食因素的IHD疾病负担与全球及5类SDI地区对比分析
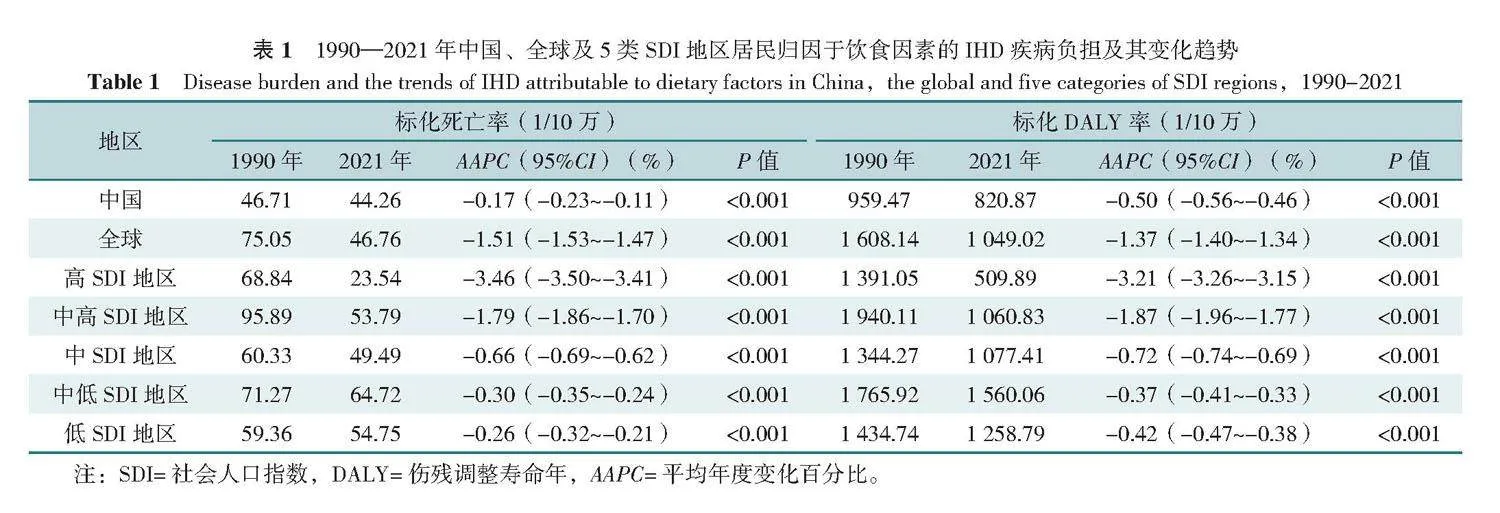
1990年中国归因于饮食因素的IHD标化死亡率和标化DALY率低于全球及5类SDI地区水平,而2021年标化死亡率、标化DALY率中国高于高SDI地区,与全球水平接近,低于其余4类SDI地区。1990—2021年中国与全球及5类SDI地区归因于饮食因素的IHD疾病负担及其变化趋势一致,标化死亡率和标化DALY率均呈现整体下降趋势,全球下降幅度明显高于中国,高SDI地区下降速度最快。标化死亡率中国下降趋势最为平缓,与低SDI地区水平接近;标化DALY率中国下降趋势高于中低、低SDI地区,见表1。
2.2 1990—2021年中国归因于饮食因素的IHD疾病负担
1990—2021年中国归因于饮食因素的IHD标化死亡率及标化DALY率由1990年的46.71/10万和959.47/10万分别下降至2021年的44.26/10万和820.87/10万,下降幅度分别为5.25%和14.45%,AAPC分别为-0.17%(95%CI=-0.23%~-0.11%)和-0.50%(95%CI=-0.56%~-0.46%),下降趋势均有统计学意义(Plt;0.05),见表1、2。
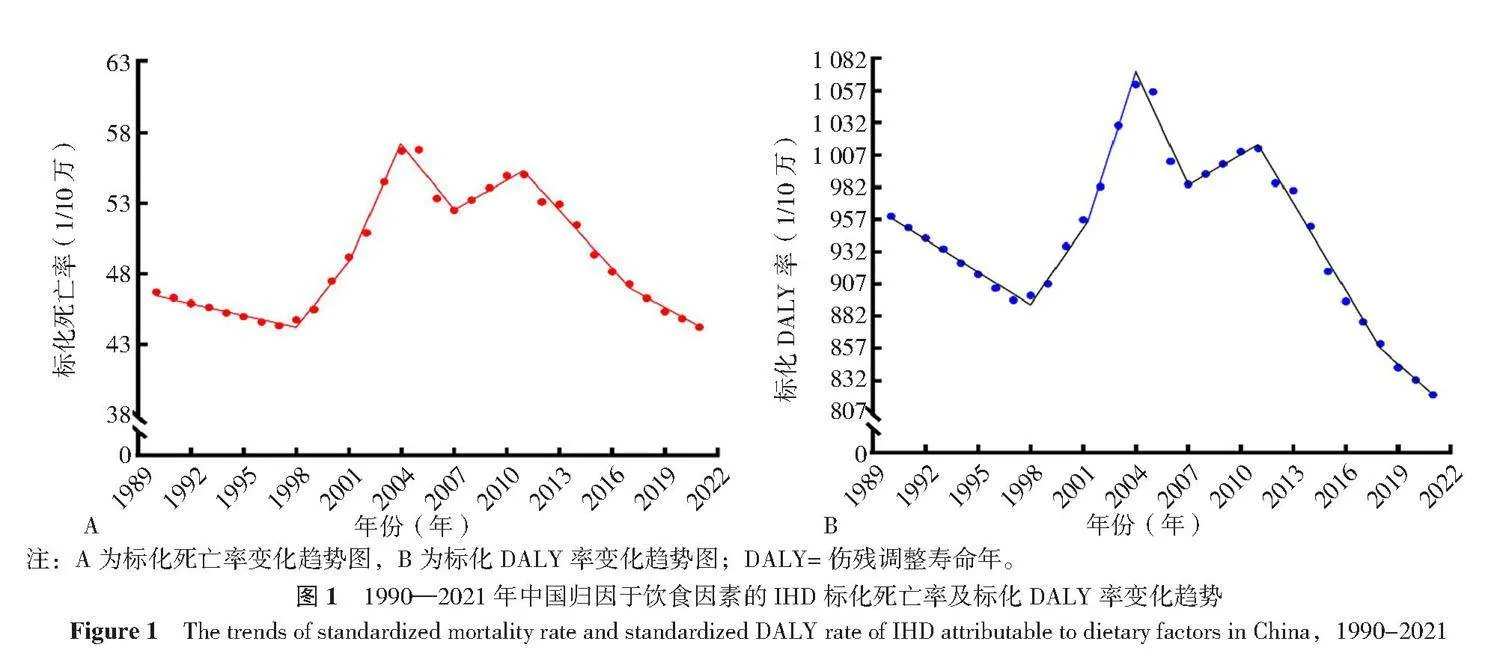
1990—2021年中国归因于饮食因素的IHD标化死亡率与标化DALY率变化趋势相似,均呈波动下降趋势;其中2001—2004年中国归因于饮食因素的IHD标化死亡率与标化DALY率增长幅度最大,APC分别为5.33%(95%CI=2.86%~5.98%)、3.85%(95%CI=1.85%~4.34%),而2011年之后均呈现下降趋势,见表2、图1。
2.3 1990—2021年中国不同性别人群归因于饮食因素的IHD疾病负担
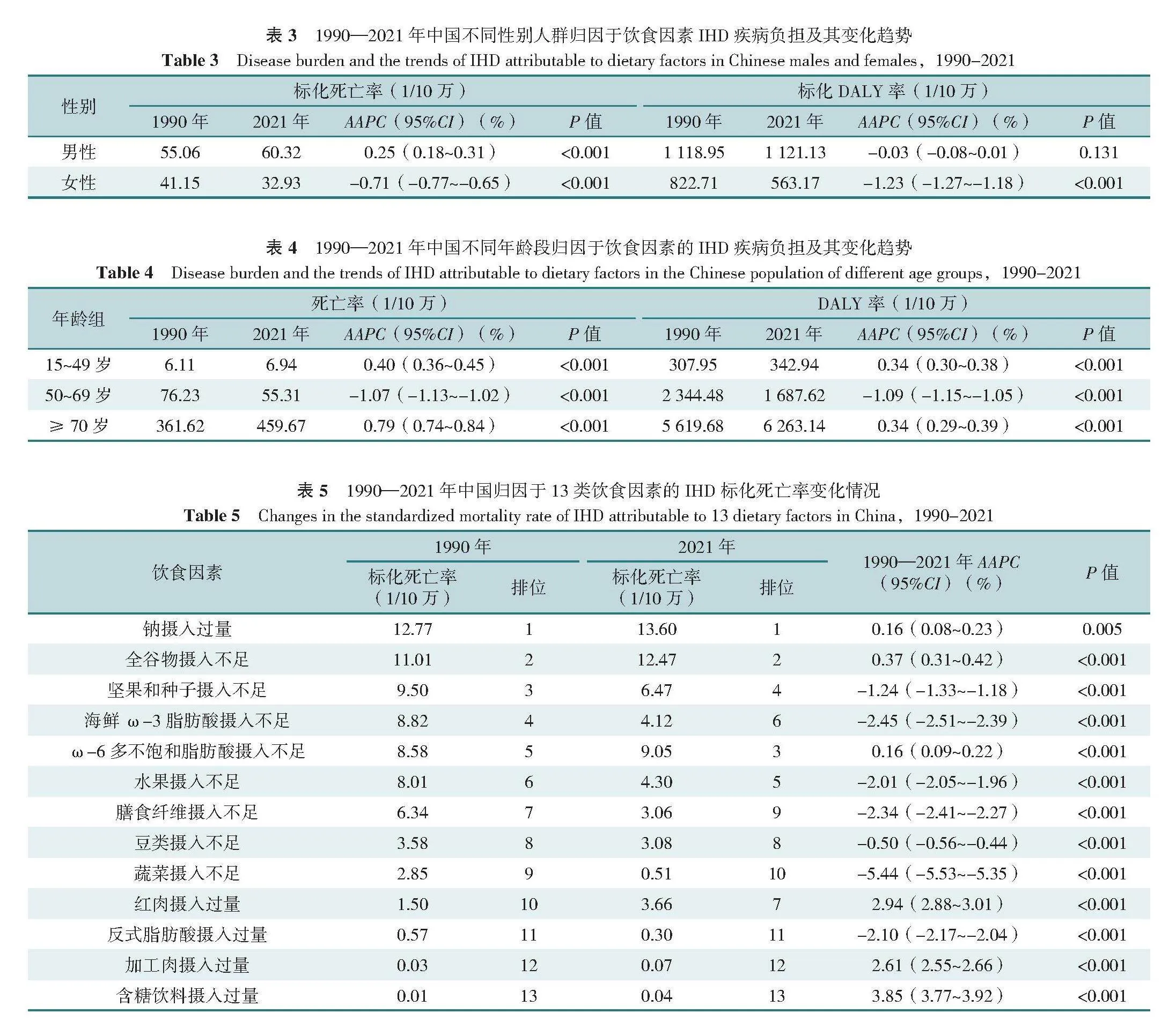
1990与2021年中国男性归因于饮食因素的IHD标化死亡率、标化DALY率均高于女性。1990—2021年中国男性归因于饮食因素的IHD标化死亡率由1990年的55.06/10万上升至2021年的60.32/10万,AAPC为0.25%(95%CI=0.18%~0.31%),上升趋势有统计学意义(Plt;0.05);男性归因于饮食因素的IHD标化DALY率趋势变化无统计学意义(Pgt;0.05)。1990—2021年中国女性归因于饮食因素的IHD标化死亡率及标化DALY率由1990年的41.15/10万和822.71/10万分别下降至2021年的32.93/10万和563.17/10万,AAPC分别为-0.71%(95%CI=-0.77%~-0.65%)和-1.23%(95%CI=-1.27%~-1.18%),下降趋势均有统计学意义(Plt;0.05),见表3。
2.4 1990—2021年中国不同年龄段归因于饮食因素的IHD疾病负担
1990与2021年中国归因于饮食因素的IHD疾病负担随着年龄增长呈上升趋势,≥70岁人群的死亡率、DALY率最高。1990—2021年中国50~69岁人群归因于饮食因素的IHD死亡率、DALY率呈下降趋势,而15~49岁、≥70岁人群呈上升趋势,趋势变化均具有统计学意义(Plt;0.05),见表4。
2.5 1990—2021年中国归因于不同类型饮食因素的IHD疾病负担
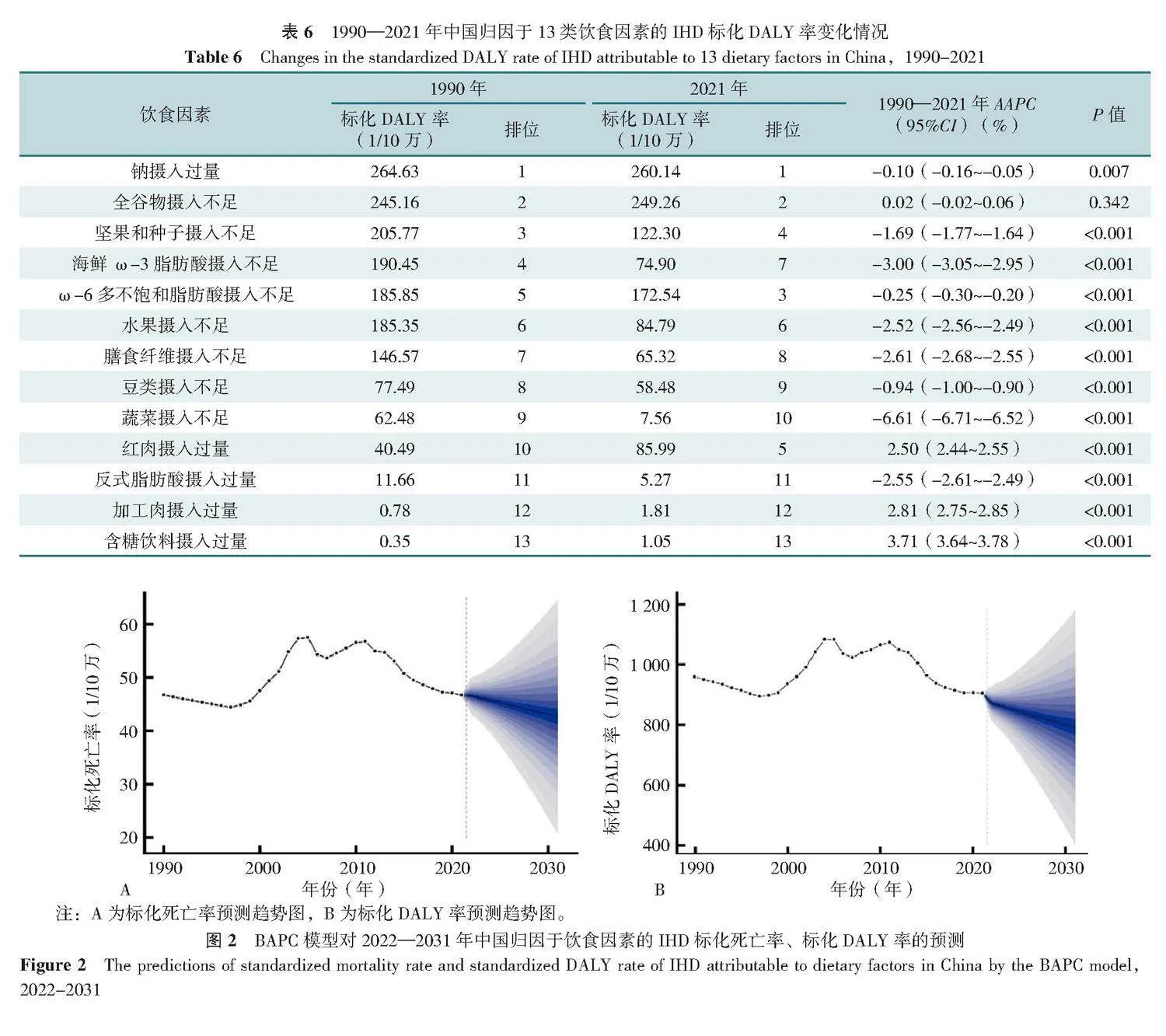
1990年与2021年13种饮食因素中导致IHD标化死亡率、标化DALY率排名前两位的饮食因素均是钠摄入过量及全谷物摄入不足;1990—2021年中国归因于ω-6多不饱和脂肪酸摄入不足的IHD标化死亡率、标化DALY率由1990年的第5位上升至2021年的第3位,坚果和种子摄入不足由第3位下降至第4位;1990—2021年中国归因于水果摄入不足的IHD标化死亡率由第6位上升至第5位,红肉摄入过量由第10位上升至第7位;1990—2021年中国归因于红肉摄入过量的IHD标化DALY率由第10位上升至第5位,见表5、6。
1990—2021年中国归因于钠摄入过量、全谷物摄入不足、ω-6多不饱和脂肪酸摄入不足、红肉摄入过量、加工肉摄入过量、含糖饮料摄入过量的IHD标化死亡率呈上升趋势(Plt;0.05);归因于坚果和种子摄入不足、海鲜ω-3脂肪酸摄入不足、水果摄入不足、膳食纤维摄入不足、豆类摄入不足、蔬菜摄入不足、反式脂肪酸摄入过量的IHD标化死亡率呈下降趋势(Plt;0.05),见表5。
1990—2021年中国归因于红肉摄入过量、加工肉摄入过量、含糖饮料摄入过量的IHD标化DALY率呈上升趋势(Plt;0.05);归因于钠摄入过量、坚果和种子摄入不足、海鲜ω-3脂肪酸摄入不足、ω-6多不饱和脂肪酸摄入不足、水果摄入不足、膳食纤维摄入不足、豆类摄入不足、蔬菜摄入不足、反式脂肪酸摄入过量的IHD标化DALY呈下降趋势(Plt;0.05),见表6。
1990—2021年中国归因于饮食因素的IHD标化死亡率、标化DALY率上升趋势较明显的是含糖饮料摄入过量、加工肉摄入过量、红肉摄入过量,见表5、6。
2.6 2022—2031年中国归因于饮食因素的IHD疾病负担预测
BAPC模型显示,未来10年中国归因于饮食因素的IHD标化死亡率,标化DALY率均呈下降趋势,标化死亡率预计在2031年下降至42.60/10万,标化DALY率下降至791.39/10万(图2)。
3 讨论
本文全面分析了饮食因素对IHD疾病负担的影响,研究发现1990—2021年中国归因于饮食因素的IHD标化死亡率及标化DALY率呈下降趋势,提示中国膳食防控取得一定成果;其中标化死亡率、标化DALY率均在2001—2004年间增加幅度最大,可能与中国快速城市化和工业化,社会经济发展快[11]导致饮食结构变化有关;在2011年之后均呈现下降趋势,可能与治疗和药物水平整体改善有关,同时2011年颁布的《中国心血管病预防指南》[12]可能为中国心血管病防控发挥了重要作用。虽然中国与全球及5类SDI地区归因于饮食因素的IHD疾病负担均呈下降趋势,但相较于高SDI地区,中国下降的速度较慢,这可能因为高SDI地区有更强的经济实力和医疗资源,在医疗卫生方面的投入和技术水平相对较高,下降速度较快,同时中国与低SDI下降水平接近,这提示中国在IHD饮食防控方面仍然有较大的提升空间,需进一步重视IHD的饮食防控策略[13],未来可以借鉴高SDI地区的成功经验,进一步引进和推广先进的医疗技术和公共卫生措施,加强国际合作,共同应对IHD饮食防控的挑战。
不同性别之间存在显著差异,1990年与2021年中国归因于饮食因素的IHD疾病负担均呈现男性明显高于女性的特点,这可能与雌激素对缺血性心肌细胞具有抗氧化和抗凋亡的保护作用有关[14];另外,男性更有可能具有高脂肪、酒精摄入过多和不规律的饮食等不良饮食习惯,这会增加基线心血管疾病的患病率[15],而女性较男性更关注身体健康,容易接受健康教育从而养成良好的饮食习惯[16]。这提示应加强男性健康教育工作,以期降低不良饮食习惯所带来的IHD风险。
随着年龄的增加疾病负担呈现上升趋势,≥70岁人群死亡率与DALY率远高于15~49岁、50~69岁组。目前中国已进入中度老龄化社会,并预计于2035年前后步入重度老龄化社会[17],慢性疾病在高年龄段疾病负担更重[18],进一步提示人口老龄化对IHD疾病负担的影响。同时结果显示,中国15~49岁组归因于饮食因素的IHD疾病负担虽然较低,但32年来呈上升趋势,与既往研究结果一致[19]。青壮年较老年人的事业、家庭压力更大,患IHD后生活质量、劳动损失的影响远大于中老年患者,因此除了加强老年人饮食因素造成的IHD的预防和控制,还应增加对年轻群体的关注。
1990年及2021年钠摄入过量与全谷物摄入不足对IHD疾病负担贡献较大,并且含糖饮料摄入过量、加工肉摄入过量、红肉摄入过量造成的疾病负担32年来呈现明显上升趋势。可能原因是随着经济的发展,中国的饮食结构发生了变化,由植物性食物为主转变为以谷物和动物性食物并重的高糖、高脂肪、高蛋白的模式[20]。2000年以来,中国肉类总产量就始终占据世界各国的首位[21],中国健康与营养调查显示目前城镇和农村居民2018年畜肉平均摄入量均高于膳食指南推荐量[22]。家庭人均每日烹调用油量达43.2 g,用盐量也与推荐量差距较大,而豆类及奶类、蔬菜水果的消费量仍然偏低[23]。越来越多的证据表明饮食习惯对健康有影响,一项队列研究显示与很少摄入含糖饮料的人相比,每天摄入≥2份含糖饮料者患心血管疾病的风险比为1.21[24]。本研究结果显示,中国含糖饮料摄入过量导致IHD的疾病负担排位最低,但其上升最快,未来应引起重视。红肉摄入过量将会增加IHD及癌症的负担[25],加工肉由于其含有防腐剂、添加剂对心脏健康的危害较大[26],低盐饮食患心血管疾病的风险将会降低[27]。因此,未来应加强宣传健康的膳食模式,倡导增加全谷物的摄入,减少钠盐、含糖饮料、加工肉、红肉的摄入,养成健康的饮食习惯、减少由饮食因素造成的疾病负担。
BAPC模型显示未来10年归因于饮食因素的IHD标化死亡率、标化DALY率呈下降趋势,提示中国最新的健康和营养相关政策《健康中国行动计划(2019—2030)》中促进均衡饮食的目标可能持续取得成效[28]。但预测结果下降幅度仍然不明显,仍需继续加强综合性的防控措施,以实现更好的IHD饮食控制效果。
综上所述,本文通过研究中国居民归因于饮食因素的IHD疾病负担变化趋势及预测为解决饮食相关IHD疾病负担提供了可能以及可行的政策选择。饮食因素作为IHD长期、复杂且广泛的影响因素,在人口老龄化加重的形势下,加强健康膳食选择的健康教育,根据不同人群采取针对IHD高危影响因素的干预措施具有重要意义。中国归因于饮食因素的IHD标化死亡率、标化DALY率均呈下降趋势,但下降速度与高SDI地区相比差距较大,且不同的性别和年龄之间存在差异,因此仍需重视IHD的饮食防控策略,加强健康膳食模式的宣传,如减少钠盐的摄入、增加全谷物的摄入,应重点管理男性及老年人群,提高中国居民健康素养以减轻其带来的疾病负担。本研究存在局限性,首先未考虑饮食因素与其他因素存在的相互作用;其次未对中国各个省市、地区、城乡间归因于饮食因素的IHD疾病负担差异进行比较分析。
作者贡献:吴霞负责文章构思、撰写和修改;吴霞、张译匀负责资料的收集、整理以及图表的绘制;姚承志、赵湘玲负责分析与讨论、数据校对;熊文婧、让蔚清负责研究设计、数据核准及全文修订。
本文无利益冲突。
吴霞https://orcid.org/0009-0000-9611-3736
让蔚清https://orcid.org/0009-0000-3567-7634
参考文献
JENSEN R V,HJORTBAK M V,BØTKER H E. Ischemic heart disease:an update[J]. Semin Nucl Med,2020,50(3):
195-207. DOI:10.1053/j.semnuclmed.2020.02.007.
FU X L,WANG J,JIANG S,et al. Mortality trend analysis of ischemic heart disease in China between 2010 and 2019:a joinpoint analysis[J]. BMC Public Health,2023,23(1):644. DOI:10.1186/s12889-023-15549-3.
MOROVATDAR N,AVAN A,AZARPAZHOOH M R,et al. Secular trends of ischaemic heart disease,stroke,and dementia in high-income countries from 1990 to 2017:the Global Burden of Disease Study 2017[J]. Neurol Sci,2022,43(1):255-264. DOI:10.1007/s10072-021-05259-2.
World Health Organization. Global Health Estimates:Life expectancy and leading causes of death and disability[EB/OL]. [2024-08-07]. https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates.
中国心血管病预防指南写作组,中华心血管病杂志编辑委员会. 中国心血管病预防指南(2017)[J]. 中华心血管病杂志,2018,46(1):10-25. DOI:10.3760/cma.j.issn.0253-3758.
2018.01.004.
GBD Diseases and Injuries Collaborators. Global incidence,prevalence,years lived with disability(YLDs),disability-adjusted life-years(DALYs),and healthy life expectancy(HALE)for 371 diseases and injuries in 204 countries and territories and 811 subnational locations,1990-2021:a systematic analysis for the Global Burden of Disease Study 2021[J]. Lancet,2024,403(10440):2133-2161. DOI:10.1016/S0140-6736(24)00757-8.
GBD Risk Factors Collaborators. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations,1990-2021:a systematic analysis for the Global Burden of Disease Study 2021[J]. Lancet,2024,403(10440):2162-2203. DOI:10.1016/S0140-6736(24)00933-4.
宇传华,白建军. 社会人口指数(SDI)的概念及其应用[J]. 公共卫生与预防医学,2020,31(1):5-10. DOI:10.3969/j.issn.1006-2483.2020.01.002.
GBD Healthcare Access and Quality Collaborators. Measuring performance on the Healthcare Access and Quality Index for 195 countries and territories and selected subnational locations:a systematic analysis from the Global Burden of Disease Study 2016[J]. Lancet,2018,391(10136):2236-2271. DOI:10.1016/S0140-6736(18)30994-2.
TICHENOR M,SRIDHAR D. Metric partnerships:global burden of disease estimates within the World Bank,the World Health Organisation and the Institute for Health Metrics and Evaluation[J]. Wellcome Open Res,2020,4:35. DOI:10.12688/wellcomeopenres.15011.2.
吴瑞君,薛琪薪,罗志华. 我国人口迁移和城镇化格局的转折性变化:2000—2020年[J]. 上海行政学院学报,2022,
23(1):74-86. DOI:10.3969/j.issn.1009-3176.2022.01.007.
中华医学会心血管病学分会,中华心血管病杂志编辑委员会. 中国心血管病预防指南[J]. 中华心血管病杂志,2011,
39(1):3-22. DOI:10.3760/cma.j.issn.0253-3758.2011.01.002.
杨继,张垚,马腾,等. 1990—2019年中国心血管疾病流行现状、疾病负担及发病预测分析[J]. 中国全科医学,2024,27(2):233-244. DOI:10.12114/j.issn.1007-9572.2023.0470.
DONG C J,BU X,LIU J,et al. Cardiovascular disease burden attributable to dietary risk factors from 1990 to 2019:a systematic analysis of the Global Burden of Disease Study[J]. Nutr Metab Cardiovasc Dis,2022,32(4):897-907. DOI:10.1016/j.numecd.2021.11.012.
GBD Causes of Death Collaborators. Global,regional,and national age-sex specific mortality for 264 causes of death,1980-2016:a systematic analysis for the Global Burden of Disease Study 2016[J]. Lancet,2017,390(10100):1151-1210. DOI:10.1016/S0140-6736(17)32152-9.
WANG C R,WANG C P,LIU M,et al. Temporal and spatial trends of ischemic heart disease burden in Chinese and subgroup populations from 1990 to 2016:socio-economical data from the 2016 Global Burden of Disease Study[J]. BMC Cardiovasc Disord,2020,20(1):243. DOI:10.1186/s12872-020-01530-0.
陆杰华,林嘉琪. 重度老龄化社会的人口特征、风险识别与战略应对[J]. 中国特色社会主义研究,2023(1):59-68.
PENG K G,YU H L. Characteristic analysis of clinical coronary heart disease and coronary artery disease concerning young and middle-aged male patients[J]. World J Clin Cases,2021,
9(25):7358-7364. DOI:10.12998/wjcc.v9.i25.7358.
SAFIRI S,KARAMZAD N,SINGH K,et al. Burden of ischemic heart disease and its attributable risk factors in 204 countries and territories,1990-2019[J]. Eur J Prev Cardiol,2022,29(2):420-431. DOI:10.1093/eurjpc/zwab213.
王雪,祁华清. 新时代中国居民食物消费结构变化与中国食物安全[J]. 农村经济与科技,2021,32(1):104-107. DOI:10.3969/j.issn.1007-7103.2021.01.044.
李凡. 中国畜禽肉类生产的时空演变及影响因素[D]. 兰州:兰州大学,2022.
逯晓娣,房玥晖,连怡遥,等. 2030年中国成年居民畜肉摄入量预测[J]. 中国食物与营养,2022,28(3):81-85. DOI:10.3969/j.issn.1006-9577.2022.03.016.
中国居民营养与慢性病状况报告(2020年)[J]. 营养学报,2020,42(6):521.
PACHECO L S,TOBIAS D K,LI Y P,et al. Sugar-sweetened or artificially-sweetened beverage consumption,physical activity,and risk of cardiovascular disease in adults:a prospective cohort study[J]. Am J Clin Nutr,2024,119(3):669-681. DOI:10.1016/j.ajcnut.2024.01.001.
LIU D,SHI Q Y,CHENG G P,et al. Worldwide burden attributable to diet high in red meat from 1990 to 2019[J]. Arch Med Sci,2023,19(1):1-15. DOI:10.5114/aoms/156017.
DE MEDEIROS G C B S,MESQUITA G X B,LIMA S C V C,et al. Associations of the consumption of unprocessed red meat and processed meat with the incidence of cardiovascular disease and mortality,and the dose-response relationship:a systematic review and meta-analysis of cohort studies[J]. Crit Rev Food Sci Nutr,2023,63(27):8443-8456. DOI:10.1080/10408398.2022.2058461.
MA H,WANG X,LI X,et al. Adding salt to foods and risk of cardiovascular disease[J]. J Am Coll Cardiol,2022,80(23):2157-2167. DOI:10.1016/j.jacc.2022.09.039.
GAO C,XU J,LIU Y,et al. Nutrition policy and healthy China 2030 building[J]. Eur J Clin Nutr,2021,75(2):238-246. DOI:10.1038/s41430-020-00765-6.
(收稿日期:2024-07-20;修回日期:2024-08-18)
(本文编辑:康艳辉)
基金项目:2019年度湖南省芙蓉教学名师专项基金(201RFS001)
引用本文:吴霞,张译匀,姚承志,等. 1990—2021年中国归因于饮食因素的缺血性心脏病疾病负担变化趋势及预测研究[J]. 中国全科医学,2025,28(3):305-312. DOI:10.12114/j.issn.1007-9572.2024.0253.[www.chinagp.net]
WU X,ZHANG Y Y,YAO C Z,et al. Trend and prediction of changes in the disease burden of diet-related ischemic heart disease in China,1990-2021[J]. Chinese General Practice,2025,28(3):305-312.
© Editorial Office of Chinese General Practice. This is an open access article under the CC BY-NC-ND 4.0 license.