Spontaneous coronary artery rupture after lung cancer surgery: A case report and review of literature
2024-05-08YingDingRuanJianWeiHan
Ying-Ding Ruan,Jian-Wei Han
Abstract BACKGROUND Spontaneous coronary artery rupture (SCAR) is a rare and life-threatening complication after lung cancer surgery.We present a case of SCAR following left upper lobectomy,successfully managed through emergency thoracotomy and coronary artery ligation.CASE SUMMARY A 61-year-old male patient underwent left upper lobectomy and mediastinal lymph node dissection for lung cancer.The surgery was performed using singleport video-assisted thoracoscopic surgery,and there were no observed complications during the procedure.However,19 h after surgery,the patient experienced chest discomfort and subsequently developed severe symptoms,including nausea,vomiting,and a drop in blood pressure.Urgent measures were taken,leading to the diagnosis of SCAR.The patient underwent emergency thoracotomy and coronary artery ligation,successfully stopping the bleeding and stabilizing the condition.Despite postoperative complications,the patient made a successful recovery and was discharged from the hospital.CONCLUSION SCAR is a rare but life-threatening complication following lung cancer surgery.Immediate thoracotomy has been shown to be a life-saving measure,while stenting is not the preferred initial approach.
Key Words: Spontaneous coronary artery rupture;Lung cancer;Surgery;Case report
INTRODUCTION
Coronary artery rupture (CAR) has various causes,including atherosclerosis,aneurysm,trauma,infection,and vascular anomalies[1-11].Spontaneous CAR (SCAR) denotes unexplained CAR,with unclear etiology and pathology[12].Consequently,SCAR has limited literature coverage[8,13-22].Only two reports discuss coronary bleeding after pulmonary surgery[18,22].One case involved a 68-year-old man with left circumflex coronary artery bleeding on postoperative day 4,managed successfully through left thoracotomy[22].The other concerned a 58-year-old man experiencing SCAR 3 mo after surgery;emergency thoracotomy revealed a ruptured left coronary artery ramus branch,and the patient succumbed to it[18].
No reports have documented survival after SCAR within 24 h of lung cancer surgery.This study presents the first such case: A patient with significant pericardial effusion and cardiogenic shock who underwent emergent left thoracotomy,proximal left anterior descending branch ligation,and suturing.As a result,the patient successfully recovered and was discharged without complications.
CASE PRESENTATION
Chief complaints
A 61-year-old Chinese man presented to the thoracic surgery clinic with left-sided chest pain lasting 1 mo.
History of present illness
The patient has had intermittent left-sided chest pain for 1 mo.A nodule was found in the upper lobe of the left lung during the thoracic surgery clinic evaluation,suggesting a possible tumor.
History of past illness
The patient denied any surgeries or comorbidities.
Personal and family history
The patient denied any family history of malignant tumors.
Physical examination
On physical examination,the vital signs were as follows: Body temperature,36.4°C;blood pressure,135/94 mmHg;heart rate,79 beats/min;respiratory rate,20 breaths/min.The patient has no palpable lymph nodes in the neck and supraclavicular region.The chest wall appeared normal,without tenderness.The breath sounds in both lungs were clear,and the heartbeat was regular without any audible murmurs.The patient had normal limb mobility.Digital anal examination was not performed.
Laboratory examinations
Blood chemistry,cardiac enzymes,tumor markers were normal.
Imaging examinations
Computed tomography (CT) revealed a 25.4 mm × 19 mm solid nodule in the left lung apex.Electrocardiography (ECG)and 24-h Holter monitoring were normal.Echocardiography found 69.7% left ventricular ejection fraction and no other issues (Figure 1).
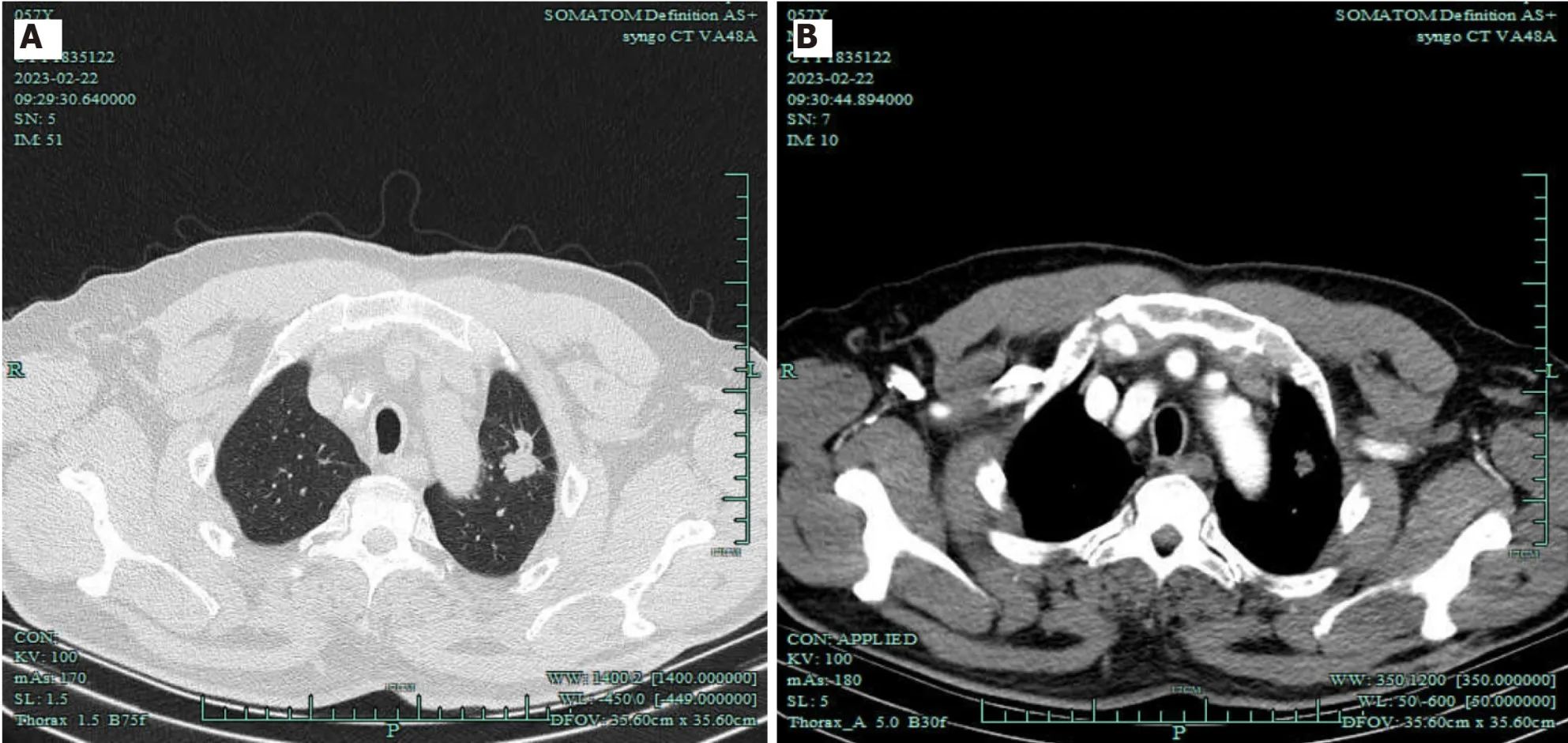
Figure 1 Imaging of pulmonary masses. A: Chest computed tomography (CT);B: Chest CT angiography revealed 50 HU.
FINAL DIAGNOSIS
Based on the patient’s medical history,the primary diagnosis was malignant lung tumor (adenocarcinoma,sT1bN0M0/IA2).Additionally,the patient was diagnosed with SCAR.
TREATMENT
On postoperative day 2,bedside echocardiography indicated no pericardial bleeding or myocardial ischemia,and coronary angiography displayed no issues (Figure 2).The patient experienced postoperative complications,including pulmonary infection,acute renal failure,and gastrointestinal infection.However,with active treatment,the patient successfully recovered and was discharged from the hospital after 10 d.
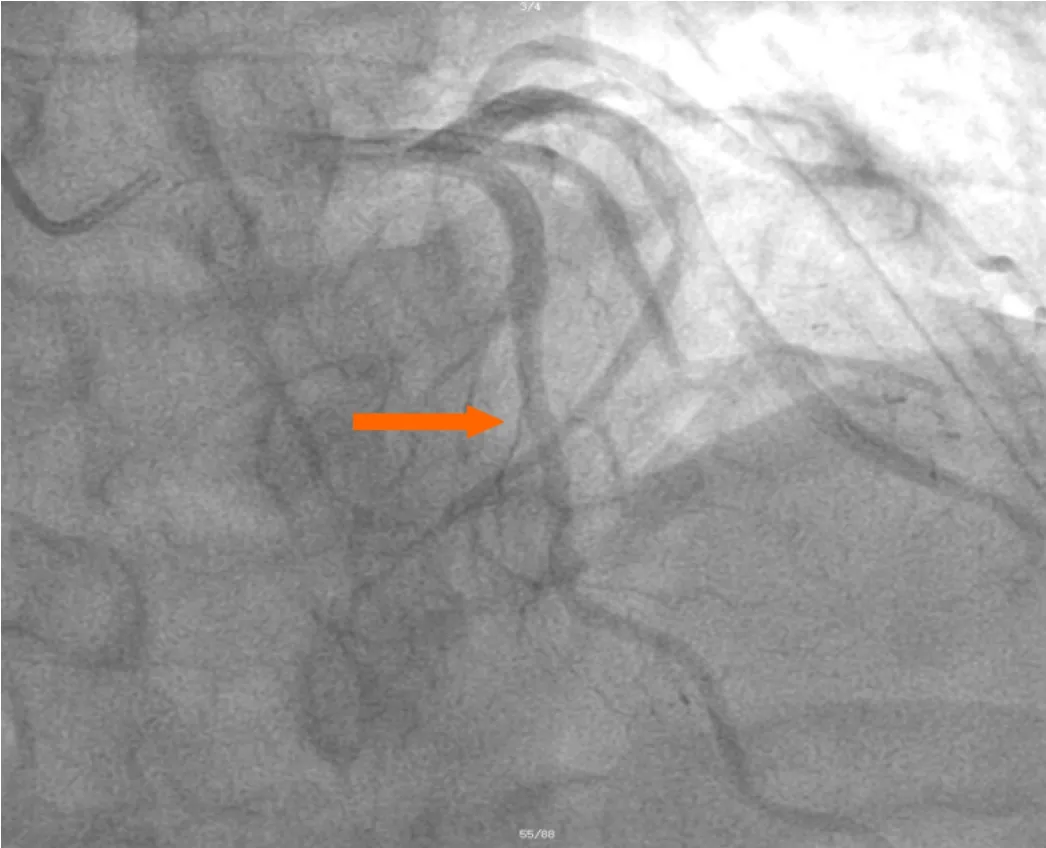
Figure 2 Partial views of coronary angiography were performed after hemostasis completion,and no abnormalities were observed in the coronary arteries (arrow).
OUTCOME AND FOLLOW-UP
The patient is still alive and in good health.
DISCUSSION
SCAR is a rare life-threatening condition that involves rupture of a normal coronary artery[13].Symptoms vary based on rupture site;some patients quickly deteriorate due to cardiac tamponade and shock,leading to sudden death[1,13-14].SCAR occurring within 24 h of video-assisted thoracoscopic left upper lobectomy,followed by successful rescue,is rarer.Our patient recovered and resumed a normal life (Figure 3 and Video).
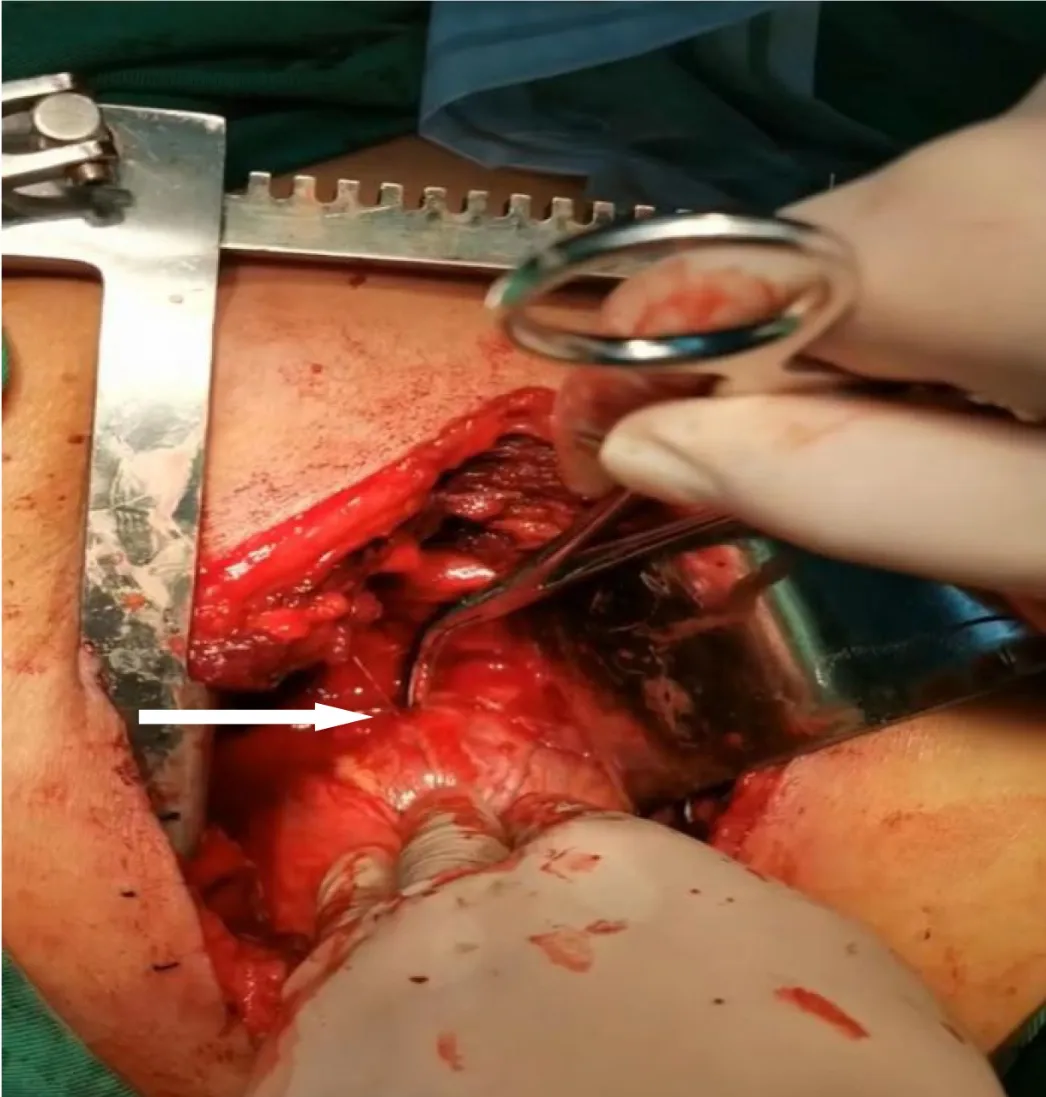
Figure 3 View of the operative field. After opening,we revealed a bleeding point in the left anterior descending coronary artery (arrow).
Cardiac tamponade after lung resection has been documented.Causes include: (1) Residual pulmonary veins retracting into pericardial space,causing intrapericardial hemorrhage[23];(2) division of aberrant bronchial arteries during surgery,retracting proximal ends into pericardium,causing tamponade[24];and (3) injury to the ascending aorta during right upper mediastinal lymph node dissection,possibly causing pericardial bleeding[25].Based on the clinical presentation and relevant examination results,we primarily attributed it to SCAR for the following reasons.Firstly,there was no evidence of coronary heart disease or a family history of the condition in the preoperative examination and medical history.During surgery,we observed no pericardial defects caused by sharp instruments,electrocautery burns,erosion,or local infection.Additionally,postoperative coronary angiography revealed no abnormalities,ruling out the possibility of hemorrhage caused by ruptured atherosclerotic coronary arteries.Since no underlying causes were identified,we consider the CAR to be spontaneous.
Prior research on coronary artery bleeding shows that pressure between the sternum and spine can rapidly raise coronary artery wall pressure.Excessive pressure beyond arterial compliance might trigger rupture[26].In this case,symptoms like nausea,vomiting,chest discomfort,and hypotension arose 19 h after surgery.Hence,we theorize that the abrupt intrathoracic pressure surge from nausea and vomiting possibly caused SCAR.
Typical SCAR clinical features mimic acute coronary syndrome,aortic dissection,or cardiac tamponade[15,27].Symptoms vary by rupture site.Left or distal right CAR leads to intrapericardial bleeding,causing tamponade and shock with hypotension,tachycardia,anxiety,altered consciousness,or sudden death.Proximal right CAR often results in subepicardial hematoma but not pericardial bleeding[15,28].
In this case,the patient primarily experienced acute chest pain and hypotension,which align with the acute clinical presentation of SCAR.Therefore,SCAR should be considered as a differential diagnosis for post-pulmonary resection pericardial tamponade.
Common diagnostic methods for CAR include chest X-ray,ECG,echocardiography,and cardiac enzyme profiles.Some cases exhibit abnormal ECG and positive cardiac biomarkers,but most have significant pericardial effusion[19].Transthoracic echocardiography (TTE) and CT angiography (CTA) are key in diagnosing SCAR.TTE confirms pericardial tamponade post-pericardiocentesis,while CTA excludes aortic dissection and other cardiovascular ruptures[3,15,18].Rapid SCAR progression and similarity to acute coronary syndrome can lead to overlooked or delayed diagnosis.Selective coronary angiography provides definitive diagnosis,but unstable patients cannot undergo the procedure.Thus,SCAR is often diagnosed during surgery.
Treating SCAR involves factors like bleeding site,severity,patient age and condition,and medical response plan.If angiography pinpoints rupture,stent implantation or coil embolization can manage bleeding[1,3,17,29].However,as most SCAR patients have tamponade and shock,angiography might not work.Timely identificationviaTTE and chest CTA is crucial for rapid surgical intervention.
For emergency surgery,selecting the right incision matters.Urgent thoracotomy needs a left anterolateral approach;stable cases use midline sternotomy.Treatments include ligation,suturing,patch repair,and revascularization.Distal artery ruptures can be ligated,causing minor heart damage.Proximal ruptures may lead to extensive infarction and heart failure,so distal revascularization is vital[30].
If the bleeding artery is not found,pericardium or patches can cover,reinforced by medical glue[2,3,19].Despite the grave outlook of SCAR,many recover wellviaemergency surgery or intervention[3].Based on Ellis’ classification[31],this SCAR could be type III,linked to 63% tamponade incidence,requiring thoracotomy,with 19% mortality.Limited data exists on coronary bleeding treatment;some cases used cardiopulmonary bypass (CPB) and cardiac arrest[1,15,19].Successful surgery removing hematoma,resolving symptoms,absence of severe plaques or artery stenosis permits safe on-beating-heart repair,avoiding the drawbacks of CPB.
Our patient had bedside echocardiography,confirming rising pericardial effusion.Emergency left anterolateral thoracotomy within 2 h revealed the bleeding site,preventing tamponade,and saving the patient’s life.
Although the patient was discharged safely and recovered his health,to date,there is a lack of large-scale research data regarding the treatment of SCAR.Therefore,it is important to determine the most appropriate medical intervention measures definitively.
CONCLUSION
Although SCRA is rare,it is vital for thoracic surgeons to watch for acute chest pain after lung resection.Monitoring vital signs,timely observation,and comprehensive examination aid rapid,accurate decisions.SCAR should be among postresection differential diagnosis.If SCAR arises after surgery,immediate thoracotomy boosts survival,and stenting is not preferred initially.
FOOTNOTES
Author contributions:Ruan YD contributed to manuscript writing and editing,and data collection and analysis;Han JW contributed to conceptualization and supervision;all authors have read and approved the final manuscript.
Informed consent statement:Informed written consent was obtained from the patient for publication of this report and any accompanying images.
Conflict-of-interest statement:All authors declare that they have no conflict of interest to disclose.
CARE Checklist (2016) statement:The authors have read the CARE Checklist (2016),and the manuscript was prepared and revised according to the CARE Checklist (2016).
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Ying-Ding Ruan 0009-0007-6772-2410;Jian-Wei Han 0000-0003-0540-7689.
S-Editor:Liu JH
L-Editor:A
P-Editor:Zhao S
杂志排行
World Journal of Cardiology的其它文章
- Facing ethical concerns in the age of precise gene therapy: Outlook on inherited arrhythmias
- Development and validation of a nomogram model for predicting the risk of pre-hospital delay in patients with acute myocardial infarction
- Seeing beneath the surface: Harnessing point-of-care ultrasound for internal jugular vein evaluation
- Risk of permanent pacemaker implantation following transcatheter aortic valve replacement: Which factors are most relevant?
- Cardiac rehabilitation after cardiac surgery: An important underutilized treatment strategy
- Inflammation as a cause of acute myocardial infarction in patients with myeloproliferative neoplasm