Radiotherapy for hyoid bone metastasis from lung adenocarcinoma: A case report
2024-03-08JonathanHsuKambridgeHribarJosephPoen
Jonathan Hsu,Kambridge Hribar,Joseph Poen
Abstract BACKGROUND Metastasis to the hyoid bone is an exceptionally rare occurrence,with documented cases limited to breast,liver,colon,skin,lung,and prostate cancers.This report highlights an unusual case involving the metastasis of lung adenocarcinoma to the hyoid bone,accompanied by a distinctive headache.Previous documentation involved surgical resection of the hyoid mass.We present a case displaying the benefits of palliative radiotherapy.CASE SUMMARY A 72-year-old non-smoking,non-alcoholic woman,initially under investigation for a year-long elevation in absolute lymphocyte count,presented with a monthlong history of intermittent throat pain.Despite negative findings in gastroenterological and otolaryngologic examinations,a contrast-enhanced chest computed tomography scan revealed a mediastinal mass and questionable soft tissue thickening in her left anterolateral neck.Subsequent imaging and biopsies confirmed the presence of lung adenocarcinoma metastasis to the hyoid bone.The patient was treated with platinum-based chemo-immunotherapy along with pembrolizumab.Ultimately,the lung cancer was unresponsive.Our patient opted for palliative radiation therapy instead of surgical resection to address her throat pain.As a result,her throat pain was alleviated,and it also incidentally resolved her chronic headaches.This is the second documented case of lung adenocarcinoma metastasizing to the hyoid bone.CONCLUSION Palliative radiotherapy may add to the quality of life in symptomatic patients with cancer metastatic to the hyoid bone.
Key Words: Metastasis;Radiotherapy;Adenocarcinoma;Hyoid;Throat;Headache;Case report
lNTRODUCTlON
This case report accounts for the second reported instance of hyoid metastasis from lung adenocarcinoma.Metastatic tumors to the hyoid bone are rare,with sporadic instances reported in breast,liver,colon,skin,lung,and prostate cancers[1-6].We present the case of a 72-year-old female patient with stage IV terminal lung cancer presenting with throat pain attributed to a metastatic tumor on the hyoid.Choosing radiotherapy over surgery,she experienced significant relief from her throat pain.
CASE PRESENTATlON
Chief complaints
A 72-year-old white female patient presents to an otolaryngology clinic complaining of intermittent throat pain for the past month.
History of present illness
Symptoms of throat pain persisted for a month with no response to antibiotics,antihistamines,or acid reflux medications.Alongside the throat pain,she was experiencing left,lateral,posterior headaches and intermittent episodes of vertigo.
History of past illness
Patient with no history of smoking or alcohol presented with a mildly elevated absolute lymphocyte count (ALC) of 4336 in February 2020.She denied systemic symptoms of fevers,night sweats,or unintentional weight loss.
Personal and family history
The patient reported only a paternal history of prostate cancer and denied melanoma,skin and squamous cell carcinomas in her family.
Physical examination
No masses were appreciated on palpation of her neck,flexible laryngoscopy,nor esophageal endoscopy.
Laboratory examinations
Mildly elevated ALC of 4336 in February 2020.A CBC in 2021 demonstrated an increase in lymphocyte count with an ALC of 5645.Given this increase in lymphocytosis,the patient was referred to a hematologist to be worked up for follicular lymphoma.
Imaging examinations
A computed tomography (CT) scan of the chest abdomen pelvis with contrast was performed,which incidentally showed a single para mediastinal 2.8 cm mass in the upper left lung lobe and questionable soft tissue thickening in her left anterolateral neck.Flow cytometry of her peripheral blood revealed an abnormal CD10 positive B-cell population,co-expressing CD20,CD19,and CD45 with low CD23 present,which is consistent with a follicular lymphoma.A CT neck with contrast,followed by magnetic resonance imaging (MRI) of the neck with and without contrast were ordered to further evaluate the neck tissue.The CT and MRI of the neck confirmed a focal soft tissue lesion with residual calcifications measuring 1.4 cm × 1.9 cm × 1.7 cm centered on the left limb of the hyoid bone (Figure 1).MRI of the neck also revealed a suspicious thyroid nodule which required an ultrasound to be further evaluated.
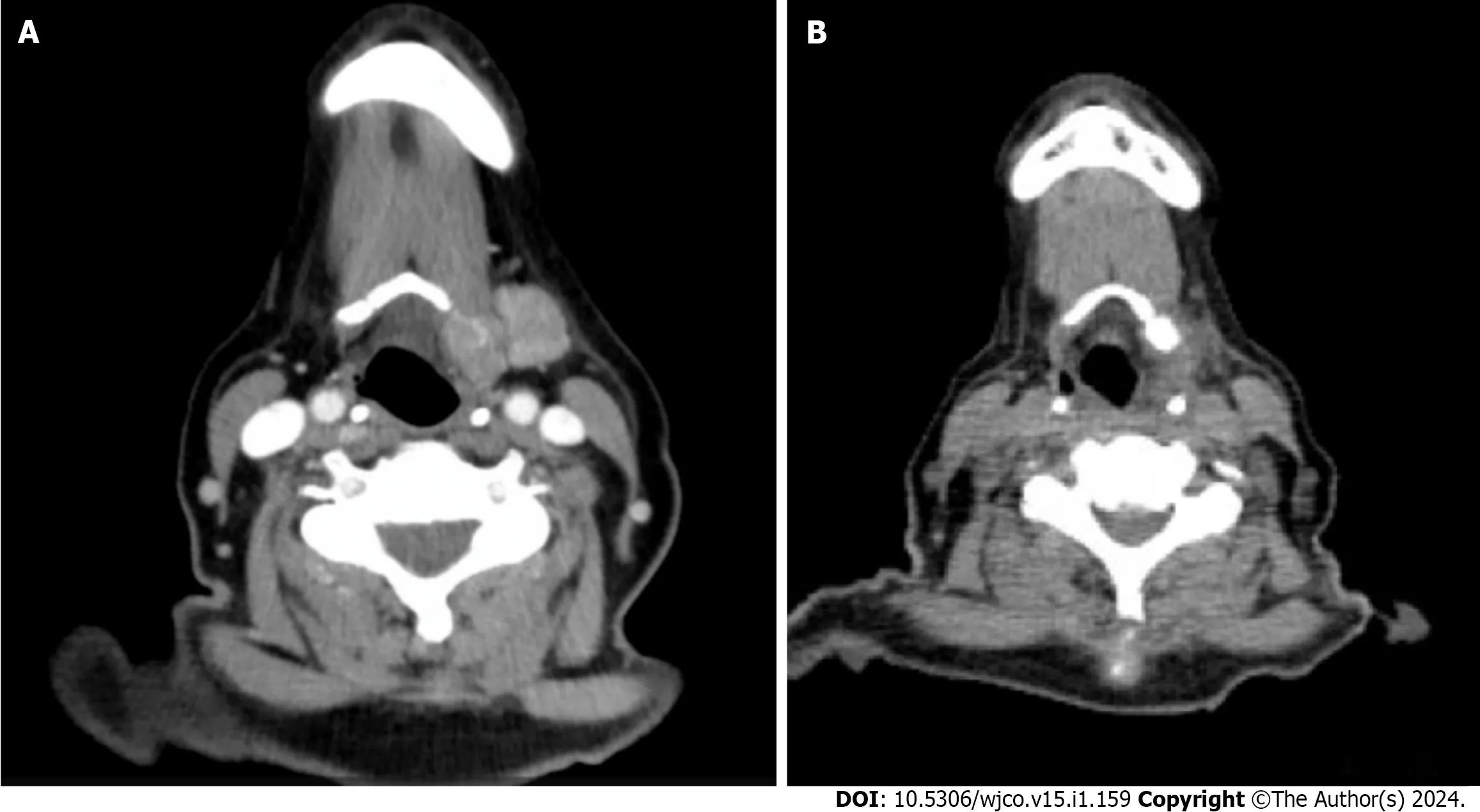
Figure 1 Computed tomography. A: Computed tomography (CT) neck w/ contrast pre-radiotherapy;B: CT neck w/contrast post radiotherapy.
Due to the improbability of follicular lymphoma in the anterior mediastinum without associated lymphadenopathy,a lung biopsy was recommended.A CT-guided biopsy of the mass in the upper left lung lobe mass identified it as invasive mucinous adenocarcinoma.Figure 2 displays the biomarkers tested for the diagnosis.Positron emission tomography (PET)/CT revealed both the ipsilateral hilar node lesion and the hyoid bone lesion exhibited significantly higher metabolic activity compared to the primary lung cancer (Figure 3).Ultrasound-guided fine needle aspiration biopsy of the left hyoid mass and the right thyroid nodule resulted in a diagnosis of metastatic mucinous adenocarcinoma and papillary thyroid carcinoma respectively.Correlation of the biopsy with PET/CT confirmed that the hyoid bone tumor had metastasized from the primary lung adenocarcinoma.
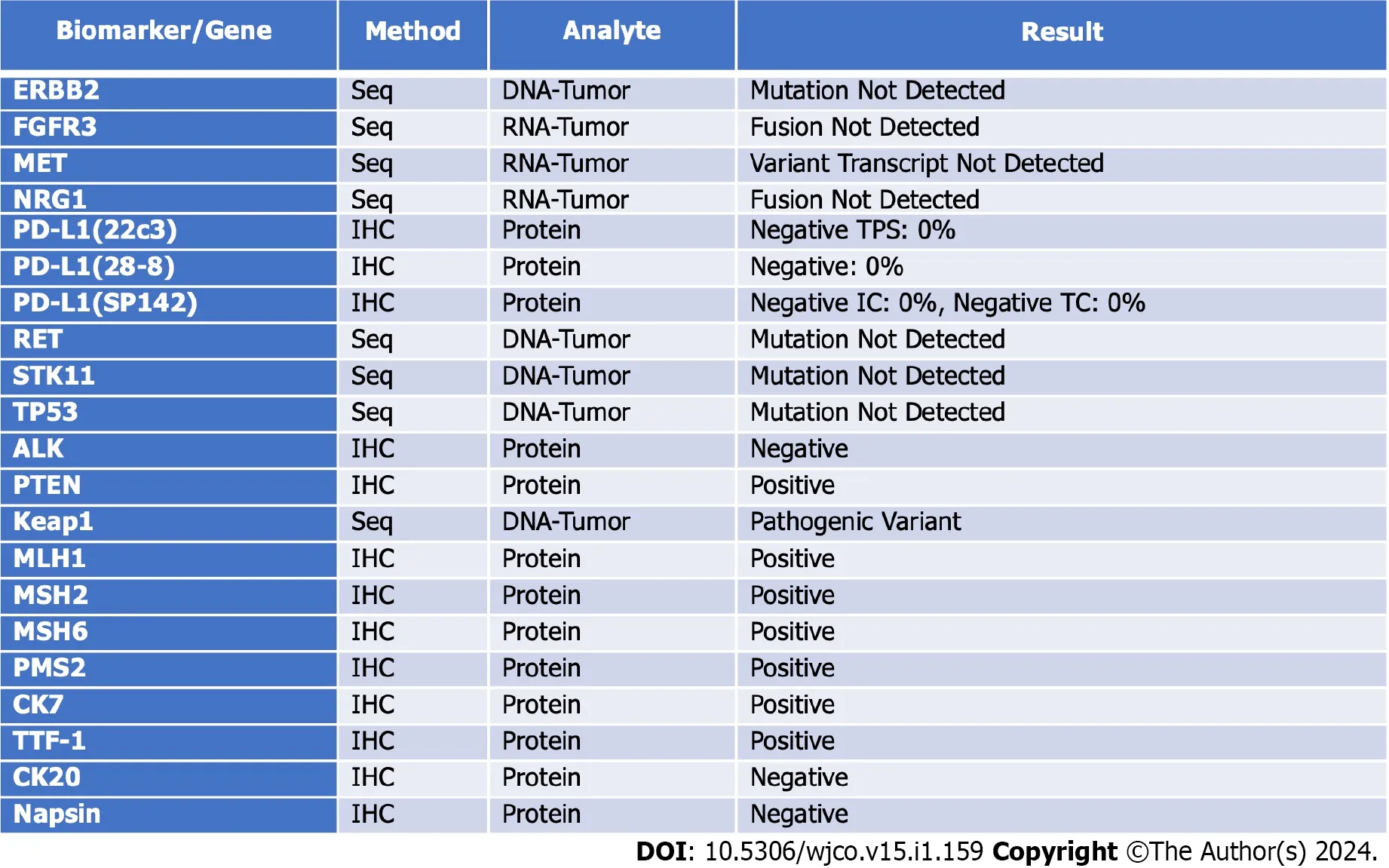
Figure 2 Lung specimen biomarker/gene table. Cancer-type relevant biomarkers and genes of the lung tumor.
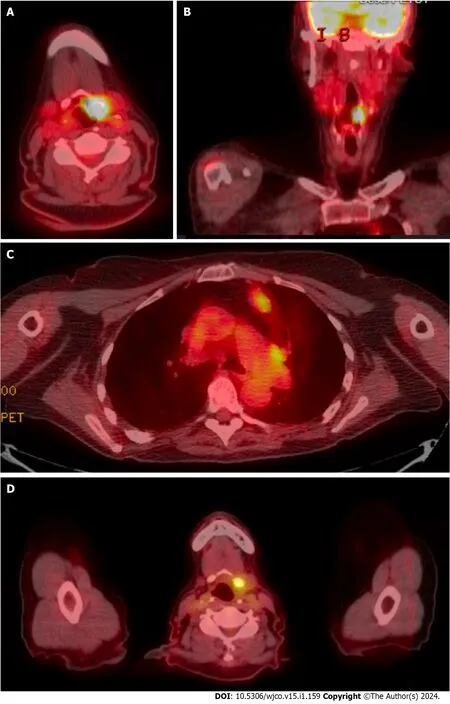
Figure 3 Positron emission tomography/computed tomography imaging. A and B: Positron emission tomography/computed tomography (PET/CT) imaging indicating hyoid bone tumor;C: PET/CT imaging indicating lung tumors;D: Hyoid region post radiotherapy.
FlNAL DlAGNOSlS
Metastatic lung adenocarcinoma of invasive mucinous type to the ipsilateral hilar node and hyoid bone.The patient was diagnosed as papillary thyroid carcinoma and follicular lymphoma.
TREATMENT
The patient,now diagnosed with metastatic lung adenocarcinoma to the ipsilateral hilar node and hyoid bone,was presented to a tumor board.The tumor board recommended against a lobectomy due to the higher recurrence risk with stage III lung cancer.Dissection of the hilar lymph node was not recommended as the node was situated in the aortopulmonary zone.Since the lung adenocarcinoma lacked targetable mutations and did not express PDL1,the patient was treated with a platinum-based chemo-immunotherapy along with pembrolizumab based on the outcomes of a clinical trial in 2018[7].The patient was also referred to head and neck surgery for consideration of resecting the metastatic cancer that engulfed the hyoid bone.However,she elected not to proceed with the procedure due to her concerns about the potential debilitating risks to swallowing and speech function.
Chemotherapy for metastatic lung cancer was initiated with Pemetrexed,Carboplatin,and Pembrolizumab for three cycles before a PET/CT scan was repeated.Despite undergoing chemotherapy,the patient continued to experience leftsided neck pain so 2 mg of dexamethasone OD was prescribed for managing her pain.PET/CT skull base to mid-thigh was repeated and after comparison to the previous PET/CT,the left upper lobe mass appeared to be stable to slightly increased in size,decreased SUV max in the ipsilateral left supra hilar node,and stable to minimally increased SUV max in the left hilar lesion which appeared grossly similar in extent to prior with some increased sclerosis of the engulfed left hyoid.These results indicated that the lung cancer was unresponsive to chemotherapy.
With disease persistent in the hyoid region and significant pain,the oncologist suggested the patient discontinue carboplatin and introduce palliative radiation for the hyoid metastatic disease.The patient chose to pursue radiotherapy.Prior to each treatment,a cone beam CT scan was obtained on the linear accelerator for targeting precision down to about 1 mm.Three hundred cGy was delivered in each treatment fraction and a total of 3600 cGy was given in 12 treatments over 2-1/2 wk.
OUTCOME AND FOLLOW-UP
The patient responded well to the treatment,completely remediating the patient’s complaint of throat pain and it also resolved the patient’s headaches.A repeated PET/CT showed a decrease of SUV max of 16.6 to 5.4 in the hyoid region.
Post palliative radiotherapy treatment,the patient remained asymptomatic for a year until succumbing to the advancing lung cancer.
DlSCUSSlON
Lung cancer is the leading cause of cancer death and the second most diagnosed cancer in the world[8].Approximately 13.2% of non-small cell lung cancer metastasizes to bone[9],which are most commonly found on the spine,chest,and pelvis[10].The hyoid bone is an unusual site for secondary tumors.This is the second reported case of lung adenocarcinoma metastasizing to the hyoid bone.
The previously documented patient elected for surgical resection of the hyoid bone[1].Our patient opted out of surgery,due to its significant risks which could negatively impact her quality of life.The hyoid bone is positioned in the anterior midline of the neck and situated axially between the mandible and thyroid cartilage[11].It plays a considerable role in phonation,conserving airway integrity,swallowing,and mastication;therefore,surgical resection of this bone potentially will result in the debilitation of these physiologic functions.
The benefits of palliative radiotherapy for bone cancer pain are well documented[12].The radiotherapy of 300 cGy with each treatment,totaling 3600 cGy over 2-1/2 wk was well tolerated by the patient,and successfully mitigated the patient’s throat pain and headaches.
The relief of headaches was an unexpected positive outcome.One potential theory could be analogous to the Stylocarotid syndrome.Patients with irregular stylohyoid complex either from an elongation of the styloid process,ossification of the stylohyoid ligament,or elongation of the hyoid bone sometimes experience neurological symptoms like headaches and vertigo.This clinical presentation of neck pain,headache,otalgia,and vertigo is due to ischemia,compression of the internal and/or external carotid arteries[11,13,14].
In conclusion,palliative radiotherapy may increase the quality of life for symptomatic patients with metastatic cancer to the hyoid bone.
CONCLUSlON
Palliative radiotherapy may add to the quality of life in symptomatic patients with cancer metastatic to the hyoid bone.
FOOTNOTES
Author contributions:Hsu J contributed to data collection and manuscript writing;Hribar K and Poen J both provided patient data,conceptualization,and supervision;and all authors have read and approved the final manuscript.
lnformed consent statement:Informed written consent was obtained from the patients for the publication of this report and any accompanying images.
Conflict-of-interest statement:The authors declare that they have no conflict of interest.
CARE Checklist (2016) statement:The authors have read the CARE Checklist (2016),and the manuscript was prepared and revised according to the CARE Checklist (2016).
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:United States
ORClD number:Jonathan Hsu 0009-0009-6054-8733.
S-Editor:Chen YL
L-Editor:A
P-Editor:Zhang XD
杂志排行
World Journal of Clinical Oncology的其它文章
- Prognostic factors of breast cancer brain metastasis
- What are the changes in the hotspots and frontiers of microRNAs in hepatocellular carcinoma over the past decade?
- Fatty acid binding protein 5 is a novel therapeutic target for hepatocellular carcinoma
- Gene signatures to therapeutics: Assessing the potential of ivermectin against t(4;14) multiple myeloma
- Predicting colorectal cancer prognosis based on long noncoding RNAs of disulfidptosis genes
- ldentification of the key genes and mechanisms associated with transcatheter arterial chemoembolisation refractoriness in hepatocellular carcinoma