Primary unifocal penile follicular center non-Hodgkin lymphoma:Report of a rare case and review of the literature
2024-02-25NikolaosKostakopoulos,ChristosMasaoutis,VasileiosArgyropoulos等
Dear Editor,
We present a rare case of a primary penile follicular center non-Hodgkin lymphoma and a review of the available literature on this condition.ABCL2gene transposition which was identified with fluorescentin situhybridization(FISH) molecular analysis is a unique manifestation not previously reported to the best of our knowledge.A 67-year-old man presented with a 3-month history of a small nodule on the left side of the corona of glans penis.The patient had no significant medical or family history.The patient underwent excision and biopsy of the penile lesion with a 0.5 cm macroscopic margin under local anesthesia and sedation.He was discharged on the day of surgery,and there were no postoperative complications or adverse events.The informed consent was obtained from the patient.
The histopathology report mentioned a 0.5 cm lesion of the glans penis,with a dense,vaguely nodular lymphoid infiltrate occupying the dermis,composed of small-to medium-sized cells with slightly irregular nuclear contours.There was minimal involvement of the mucosa of the glans penis and the corpus spongiosum.The lesion was mainly located at the Buck’s fascia,and the surgical margins were negative.Immunophenotyping revealed a mixed type of lymphocytes primarily consisting of B-cells,CD20 positive and expressing extensively the germinal center marker BCL6 in a nodular and diffuse manner,and less consisting of T-cells and CD3 positive.There was also a very rareBCL2gene transposition of 10% of the cellular population,which was identified with molecular analysis FISH and ruled out the diagnosis of pseudo-lymphoma.The final diagnosis was that of a primary follicle center lymphoma of the glans penis (Fig.1).Unusual features for this type of lymphoma were anatomical location and transposition ofBCL2gene.Staging with CT of the chest,abdomen,and pelvis showed no other signs of disease,and thorough skin examination revealed no other similar masses.Because of no signs of multifocal disease and normal blood tests,bone marrow examination was omitted.The patient was reexamined at 2 weeks and 4 weeks postoperatively until the surgical wound had completely healed.He also underwent a positron emission tomography (PET)/CT scan with choline 1 month after surgery with no signs of positive lymph nodes anywhere in the body.A repeat chest and abdomen CT and physical examination 6 months postoperatively revealed no recurrence or signs of metastases.
After the final pathology report was received,we performed a systematic search of the literature on PubMed/PMC and Cochrane databases using the terms: “penile” AND “lymphoma” AND “primary”.The search returned 74 results.After initial title screening,45 were excluded(articles not in English or titles not associated).The 29 remaining articles abstracts were evaluated,and 10 studies were finally included in the review.Lymphoid tumors of the urinary tract are rare entities with very few cases reported in the literature [1,2].Although most penile lymphomas present in adults,a 4-year-old boy was diagnosed with primary penile lymphoma [3].
Primary penile lymphomas most commonly present as non-healing ulcers or painless masses of the glans penis,the penile shaft,or the prepuce.Less commonly,patients present with symptoms of dysuria.Erectile dysfunction can occur if the mass affects the corpus cavernosum [1,4,5].Other cases have been reported presenting with priapism[6].Because primary penile lymphoma is a very rare entity,there is no protocol for its diagnosis and treatment.Some studies suggest an initial confirmation of the lymphoma with excisional biopsy,staging with CT of the chest and abdomen,and a thorough physical examination of superficial lymph nodes.If there are no other lesions and no signs of leukemic hemogram or bone marrow suppression,a diagnosis of primary penile lymphoma can be made,as was the case with our patient [2,5].Some suggest a PET/CT scan to exclude other sites of disease [7].In some cases,chemotherapy is administered after local excision for further eradication of the disease.Combination chemotherapy(cyclophosphamide,doxorubicin,vincristine,and prednisolone) with rituximab has been suggested to be effective in primary penile lymphomas [7-9].Follow-up should be continued for at least 2 years.Whole body scans should be considered because metastases have been reported in rare sites,such as brain and chest.Taking into consideration the available literature,we suggest a protocol for the management of primary penile lymphomas.Diagnosis should be based on history and physical examination,which should include meticulous skin and lymph node evaluations.Staging should include a CT scan of chest and abdomen,and if there is any diagnostic uncertainty,a PET/CT scan should also be performed.Treatment depends on the initial stage at diagnosis.Small tumors can be treated by local excision alone,while larger tumors can be safely treated with chemotherapy and local radiotherapy or local excision and additional chemotherapy.Radiotherapy has been used to treat a case of isolated pituitary stalk relapse [10].Pathology should include immunohistochemistry and FISH molecular analysis,which can identify rare gene transpositions.
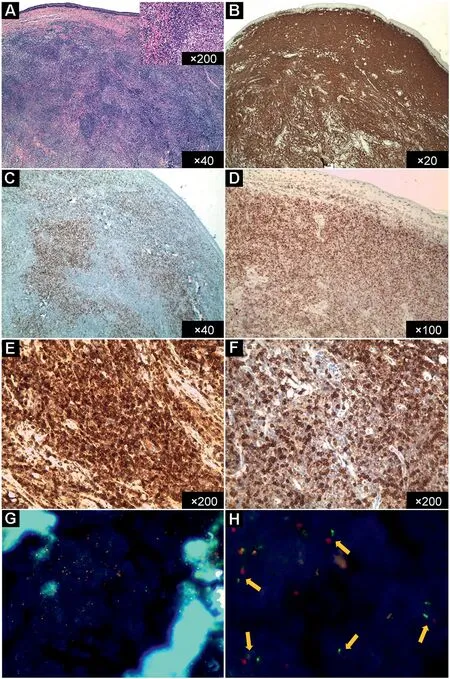
Figure 1 The results of the hematoxylin and eosin stain,immunohistochemistry,and FISH.(A)The hematoxylin and eosin stain results: a dense,vaguely nodular lymphoid infiltrate occupying the dermis,composed of small-to-medium sized cells with slightly irregular nuclear contours;(B-F) Immunohistochemistry results:extensively expressed B-cell marker(CD20)in lymphatic infiltration(B),the expression of the germinal center marker(BCL6)in a nodular and diffuse manner(C and D),and the implied expression of BCL2(E)on the B-cells when juxtaposed to CD3 immunostaining(F);(G and H)The results of FISH:fluorescent results with the break-apart probes for the BCL2 gene,consistent with BCL2 rearrangements(G),and magnified FISH of multiple split signals (yellow arrows),consistent with BCL2 rearrangements(H).FISH,fluorescent in situ hybridization.
Follow-up should continue for at least 2 years,preferably more than 5 years,and include regular physical examination and either CT or MRI scans.A PET/CT scan can also be performed at some point during follow-up to exclude any recurrence.
In conclusion,primary cutaneous penile lymphomas are rare entities and there are no standard protocols for their diagnosis and treatment.Furthermore,our case had a very rareBCL2gene transposition.Presentation of this case and review of the literature showed that B-cell penile lymphomas share many clinical features,and common pathways are suggested to facilitate management of these tumors.
Author contributions
Study concept and design: Nikolaos Kostakopoulos,Athanasios Kostakopoulos.
Data acquisition: Nikolaos Kostakopoulos,Christos Masaoutis,Varvara Pantelaion.
Data analysis: Nikolaos Kostakopoulos,Vasileios Argyropoulos,Panagiotis Theodoropoulos.
Drafting of manuscript: Nikolaos Kostakopoulos,Christos Masaoutis,Panagiotis Kouroupakis.
Critical revision of the manuscript: Athanasios Kostakopoulos,Vasileios Argyropoulos.
Conflicts of interest
The authors declare no conflict of interest.
杂志排行

Asian Journal of Urology的其它文章
- Transurethral resection of bladder tumor:A systematic review of simulator-based training courses and curricula
- Etiology and management of urethral calculi:A systematic review of contemporary series
- Oncologic outcomes with and without amniotic membranes in robotic-assisted radical prostatectomy: A propensity score matched analysis
- Single nucleotide polymorphism within chromosome 8q24 is associated with prostate cancer development in Saudi Arabia
- The risk of prostate cancer on incidental finding of an avid prostate uptake on 2-deoxy-2-[ 18F]fluoro-D-glucose positron emission tomography/computed tomography for non-prostate cancer-related pathology:A single centre retrospective study
- Prevention of thromboembolic events after radical prostatectomy in patients with hereditary thrombophilia due to a factor V Leiden mutation by multidisciplinary coagulation management