Evaluation of the diagnostic value of total bile acids/platelets in HBV related liver fibrosis
2024-01-19SUNTianYiHUANGShengkaiSUNLong
SUN Tian-Yi, HUANG Sheng-kai, SUN Long
Department of Infectious Diseases, the First Affiliated Hospital of Hainan Medical University, Haikou 570102, China
Keywords:
ABSTRACT Objective: Explore the diagnostic value of total bile acids/platelets in HBV related liver fibrosis.Methods: 160 patients with chronic HBV infection admitted to the Infection Department of the First Affiliated Hospital of Hainan Medical College from February 2021 to December 2022 were selected.They were divided into two groups based on the degree of liver fibrosis detected by liver biopsy: significant liver fibrosis group and non-significant liver fibrosis group.The total bile acid/blood platelet levels and their correlation with liver fibrosis in the two groups were compared and observed, and the efficacy of other non-invasive liver fibrosis diagnostic models was evaluated.Results: (1) Compared with the non-significant liver fibrosis group, the significant liver fibrosis group showed an increase in total bile acid levels, a decrease in platelet levels, and a significant increase in total bile acid/platelet levels (P<0.05).(2) Platelets decrease with the increase of liver fibrosis degree, total bile acids increase with the increase of liver fibrosis degree, and total bile acids/platelets increase with the increase of liver fibrosis degree.(3) The area under the curve (AUC) of total bile acid/platelet, APRI, FIB-4,and elastography in diagnosing the degree of liver fibrosis were 0.69, 0.57, 0.56, and 0.68,respectively.Conclusions: The diagnostic efficacy of total bile acids/platelets in diagnosing HBV related liver fibrosis is no less than that of other liver fibrosis diagnostic methods, and it is non-invasive, simple, and convenient, which is worthy of further clinical promotion and validation.
1.Introduction
Hundreds of millions of patients are infected by hepatitis B virus every year around the world, and China is a high prevalence area for patients with hepatitis B virus infection, and the transition to cirrhosis in various chronic hepatitis B is based on the pathology of hepatic fibrosis[1].Several experts have confirmed that liver fibrosis can be diagnosed and treated at an early stage if it is detected when it has just formed, and the disease progression can be reversed in a timely and effective manner[2].Therefore, early detection of liver fibrosis in clinical practice plays a very crucial role in slowing down the progression of the disease[3].In recent years, the use of non-invasive serological indicators for the early detection of the degree of hepatic fibrosis is a hot research topic, Total bile acid (TBA), is positively correlated with the pathological degree of fibrosis in liver tissue[4-5].Platelet (PLT), has been clinically shown to independently predict the pathological degree of hepatic tissue fibrosis[6] , but the total bile acid/platelet (TBA/PLT, TRP) in diagnosing chronic HBV-infected patients has been reported less frequently and without in-depth studies.Therefore, the present study was focused on evaluating the value of TRP in the diagnosis of hepatic fibrosis in HBV-infected patients by observing its changes in different degrees of hepatic fibrosis.
2.Information and Methods
2.1 General information
160 patients with chronic HBV infection admitted to the Department of Infection of the First Affiliated Hospital of Hainan Medical College and completed liver biopsy from February 2021 to December 2022 were selected, and were divided into two groups according to the degree of hepatic fibrosis in liver histopathology[7]: 57 cases in the non-significant hepatic fibrosis group (S0-S1),with 35 cases of males and 22 cases of females, and an average age of (37.79 ± 9.44) years; Significant liver fibrosis group (S2-S4)103 cases, there were 76 males and 27 females, mean age (40.66 ±10.38) years.There was no difference in the comparison of gender and mean age between the two groups (P>0.05).This study was approved by the Ethics Committee of our hospital.
2.2 Inclusion and exclusion criteria
(1) Inclusion criteria: ① Meet the diagnostic criteria for chronic HBV infection in the Guidelines for the Prevention and Control of Chronic Hepatitis B (2019 edition)[8]; ② Patients who have not undergone antiviral treatment; ③ Age over 18 years old.(iv) have signed the informed consent.
(2) Exclusion criteria: ① Taking some drugs that may affect blood routine and liver function in the last six months; ② Patients with malignant tumours; ③ Patients with some other liver diseases such as combined metabolism-associated steatohepatopathy, alcoholic liver disease, autoimmune liver disease, and so on.
2.3 Methods
2.3.1 Detection of clinical indicators
Venous blood of patients was retained for clinical laboratory examination to register PLT, ALT, AST, TBA and other indicators,and these serological indicators were used to calculate the noninvasive liver fibrosis diagnostic model commonly used in the clinic,APRI = [AST (U/L) / upper limit of normal value of AST (U/L) /PLT (×109)] × 100.FIB-4 = age × AST/( PLT count × ALT (U/L).
2.3.2 Fibroscan test
Fibroscan test was completed and registered by the same experienced departmental physician in all patients before liver biopsy.
2.3.3 Liver pathology examination
The indications and contraindications for liver biopsy were strictly grasped, and after the consent of the patients and/or their families,liver biopsy puncture was performed, and the liver histopathology was read by the same pathologist.According to the degree of hepatic fibrosis in liver histopathology, they were divided into nonsignificant hepatic fibrosis group (S0-S1) and significant hepatic fibrosis group (S2-S4).
2.4 Clinical observation indexes
(1) Compare the results of serology in the two groups of subjects,including TBA, PLT, TRP; (2) Observe the changes of TBA, PLT,TRP, APRI, FIB-4, Fibroscan between different liver fibrosis stages,respectively; (3) Evaluate the four non-invasive serological indexes,namely, TRP, APRI, FIB-4, and Fibroscan, respectively, in the diagnostic efficacy in diagnosing the degree of liver fibrosis.
2.5 Statistical processing
The data were processed and analysed using SPSS 26.0 software,using (±s) to indicate continuous variables and normally distributed data, statistically verified using the t-test, and using interquartile spacing to indicate data that do not conform to the normal distribution and continuous variables, statistically verified using the non-parametric test; for the different non-invasive diagnosis of the degree of hepatic fibrosis of the serological indexes were correlated using the Spearman coefficient.Spearman’s coefficient was used for correlation analysis; the area under the ROC curve was used to compare the diagnostic value of the newly established non-invasive liver fibrosis indicators with the traditional non-invasive serological indicators that were commonly used in the past.
3.Research results
3.1 Comparison of TBA, PLT and TRP levels between the two groups of patients
The serum levels of TBA and TRP in patients in the significant liver fibrosis group were higher than those in the non-significant liver fibrosis group, and the differences were statistically significant (P<0.05), and the levels of TRP were higher than those of TBA in the significant liver fibrosis group, and the differences were statistically significant (P<0.05), and the serum levels of PLT in patients in the significant liver fibrosis group were lower than those in the nonsignificant liver fibrosis group, and the differences were statistically significance (P<0.05), as shown in Table 1.
3.2 Changes in TBA, PLT, TRP, APRI, FIB-4, Fibroscan in different liver fibrosis stages
By Spearman correlation analysis, TBA, TRP, APRI, FIB-4,and Fibroscan were all positively correlated with the pathological stage of the degree of hepatic fibrosis, and the differences were all statistically significant (P<0.05), and by Pearson correlation analysis,PLT was negatively correlated with the pathological stage of the degree of hepatic fibrosis, and the differences were all statistically significant (P<0.05), as shown in Table 2.
3.3 Evaluation of the efficacy of TRP in the diagnosis of HBV-related liver fibrosis
The specificity of the four non-invasive liver fibrosis diagnostic indices, TRP, APRI, FIB-4, and Fibroscan, in diagnosing the degree of liver fibrosis was 82.7%, 56.7%, 49.6%, and 63.8%, respectively,and the sensitivity was 51.5%, 60.6%, 63.6%, and 75.8%,respectively.The area under the curve (AUC) was 0.692, 0.579,0.569, 0.687, respectively, and it can be seen that among them, the efficacy of TRP in diagnosing the degree of hepatic fibrosis was slightly higher than that of the other diagnostic indicators of noninvasive hepatic fibrosis, as shown in Table 3 and Figure 1.

Tab 1 Comparison of TBA, PLT and TRP between the two groups of patients
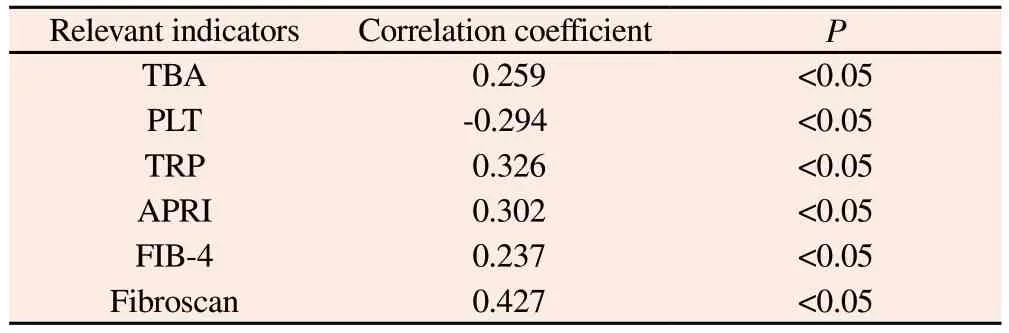
Tab 2 Correlation analysis between TBA, PLT, TRP, APRI, FIB-4, Fibroscan and degree of liver fibrosis
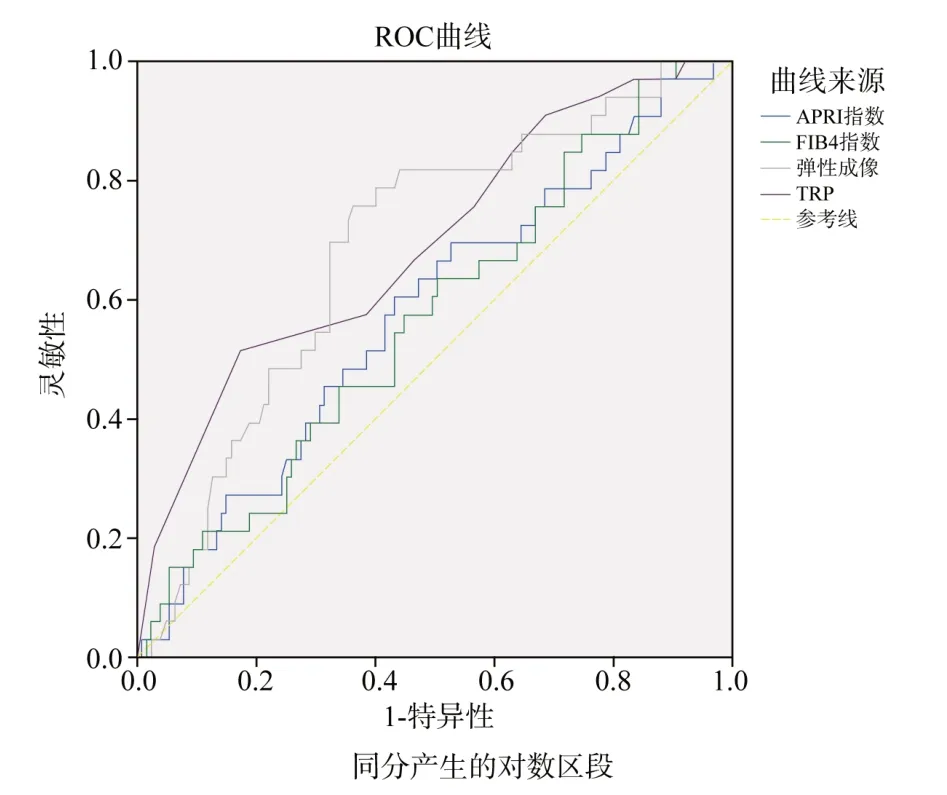
Fig 1 Diagnostic value of TRP, APRI, FIB-4 and Fibroscan for the degree of liver fibrosis
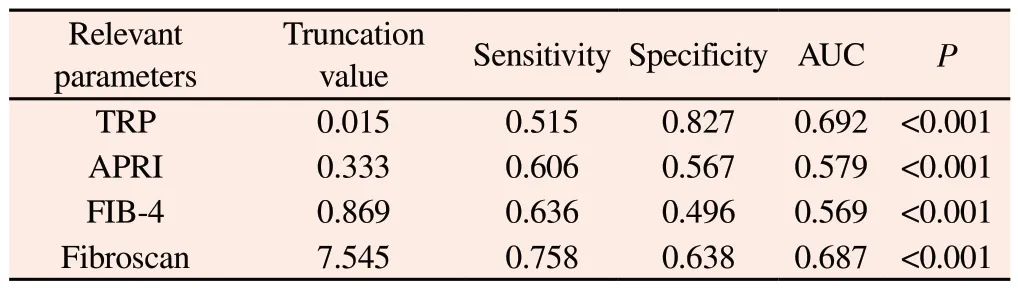
Tab 3 Evaluation of the efficacy of TRP in the diagnosis of HBV-related liver fibrosis
4.Discussion
In patients with chronic HBV infection, the early onset of symptoms is relatively insidious and not easy to be detected clinically.With the continuous stimulation of liver tissues by the virus, extracellular matrix, the continuous formation of hepatic fibrils and their continuous degradation, and the imbalance of the ratio between them, hepatic fibrosis can be formed, and finally,further development of cirrhosis, or even hepatocellular carcinoma can occur[9] , and the degree of progression of the disease depends on the balance between fibrinolysis and fibrogenesis.The extent of disease progression depends on the balance between fibrolysis and fibrogenesis, and liver fibrosis occurs in the context of chronic inflammation and subsequent microcirculatory disturbances,including microthrombosis, so it is crucial to know the extent of hepatic fibre progression in patients with chronic hepatitis B virus infection in a timely manner[10-12] , and early detection and early antiviral treatment can prevent further disease progression.
Currently, the gold standard in clinical practice is the liver puncture biopsy technique, but it is prone to sampling errors and subjective judgement by the observer in the sampling process, poor patient compliance in the testing process, and sometimes up to 3% of patients undergoing the procedure may experience serious complications, including death in 0.03% of patients, which is an invasive procedure that may cause many potential complications in patients.This is an invasive technique with many potential complications[13-15] , so it is important to choose an accurate noninvasive test to diagnose and stage the degree of hepatic fibrosis.Fibroscan is a non-invasive diagnostic technique that is commonly used in clinical practice, but the use of this technique requires special instruments and lacks the two-dimensional grey scale imaging B-mode and real-time liver hardness imaging, making the measurement results inaccurate and difficult to measure.make measurements inaccurate and difficult to measure in patients with obesity, ascites or intercostal stenosis.In addition clinical trials have investigated the use of a new non-invasive serological index for the early diagnosis of liver fibrosis in patients with chronic HBV infection[16-18].
The liver is the most important metabolic organ in the human body, TBA is one of the main components of bile, all of which is secreted by the liver, and most of which is absorbed through the ileum, enters the liver through the portal vein, and then re-excretes into the intestines through the bile ducts, and a small portion of which will be directly discharged out of the body through the urine or faeces.When the liver is damaged by various damaging factors,which impedes the normal metabolism, the bile will stagnate in the liver, and serum levels of TBA will increase.When the normal metabolic function of the liver is impeded due to damage caused by various injury factors, bile will be stagnant in the liver and the serum bile acid level will increase.According to a study, TBA can be used as a predictive factor to differentiate early liver fibrosis from advanced liver fibrosis.This study also found that TBA increased significantly with the degree of hepatic fibrosis, so bile acids may be considered as an indicator of the degree of hepatic fibrosis[19].In the present study, it was found that serum levels of TBA increased with increasing degree of hepatic fibrosis and the differences were statistically significant, suggesting a close correlation between TBA and the degree of hepatic fibrosis.
PLT is produced by megakaryocytes in the bone marrow and thrombocytopenia is also one of the most common haematological problems in patients with chronic hepatitis B virus infection[20-22].Under normal conditions, the liver can produce PLT-generating hormone, which can bind to the megakaryocyte receptor in the bone marrow to promote the proliferation and division of megakaryocytes in the body, thus producing more PLT for use by the organism;when the liver undergoes severe fibrosis, the amount of PLTgenerating hormone produced by the liver decreases, resulting in reduced production of PLT, and the activation of mononuclear phagocytosis, resulting in a decrease in the production of PLT and activation of mononuclear phagocytes.When severe fibrosis occurs in the liver, the amount of PLT-generating hormone produced in the liver decreases, leading to a decrease in PLT production and activation of the mononuclear phagocyte system in the body, which leads to a massive destruction of PLT in the spleen and a decrease in the number of platelets.Many studies have shown that PLT is an important predictor of the degree of liver fibrosis.The results of the present study also suggest that as the degree of hepatic fibrosis increases, the level of PLT in the serum decreases, and there is a negative correlation with the pathological stage of the degree of hepatic fibrosis, and the differences are statistically significant(P<0.05), suggesting that there is a close correlation between PLT and the degree of hepatic fibrosis.
Previous studies have used TBA or PLT alone to detect the degree of liver fibrosis in different stages, but no study has combined the two together to detect the degree of liver fibrosis.In this study,160 patients with CHB were studied to observe the changes of TRP in different degrees of hepatic fibrosis, to evaluate its value in the diagnosis of hepatic fibrosis in HBV-infected patients, and to assess its diagnostic efficacy by APRI, FIB-4, and Fibroscan.The diagnostic efficacy is slightly higher than that of APRI, FIB-4 and Fibroscan, and has the advantages of simplicity, visualisation and relatively high patient compliance, which is expected to be promoted and applied in future clinical work.
Due to the small clinical sample size, it has not yet been possible to establish the optimal threshold of TRP for the diagnosis of HBV-associated liver fibrosis, and it is hoped that multi-centre,randomized controlled studies will be conducted in future work to provide more high-quality clinical research evidence and further research will be carried out to explore the intrinsic mechanisms.
Authors’ Contribution
Tianyi Sun: conceived and designed the article, compiled the data,and wrote the paper; Long Sun: was responsible for quality control and proofreading of the article, and was responsible for the article as a whole; and Shengkai Huang: collected the data.
The authors of this article all declare no conflict of interest.
杂志排行
Journal of Hainan Medical College的其它文章
- Antibiotic resistance analysis and coping strategies of helicobacter pylori
- Discover the key genes for glomerular inflammation in patients with type II diabetic nephropathy based on bioinformatics and network pharmacology
- Evaluation of the diagnostic efficacy of noninvasive diagnosis in patients with chronic viral hepatitis B complicated with nonalcoholic fatty liver disease and significant liver fibrosis
- Meta analysis and data mining of the method of yishenhuoxue in the treatment of nonproliferative diabetic retinopathy
- Analysis of E2F3 gene variants, expression and clinical significance in melanoma based on multiple databases
- Epidemiological characteristics of hyperuricemia in metabolic syndrome and its different components in the physical examination population