SPECT/CT显像在评估缺血性心肌病患者的存活心肌中的应用价值
2023-11-01赵守松孙文杰牟兴宇陆路张蕾秦杰付巍
赵守松,孙文杰,牟兴宇,陆路,张蕾,秦杰,付巍
SPECT/CT显像在评估缺血性心肌病患者的存活心肌中的应用价值
赵守松,孙文杰,牟兴宇,陆路,张蕾,秦杰,付巍
桂林医学院附属医院核医学科,广西桂林 541001
以2-氟-18-氟-2-脱氧-D-葡萄糖(18F-fluorodeoxyglucose,18F-FDG)PET/CT心肌代谢显像为金标准,探讨锝-99m-4,9-二氮-3,3,10,10-四甲基十二烷-2,11-二酮肟(technetium-99m labeled 4,9-diaza-3,3,10,10-tetramethyldodecan-2,11- dione dioxime,99mTc-HL91)SPECT/CT乏氧显像结合锝-99m-甲氧基异丁基异腈(technetium-99m labeled sestamibi,99mTc-MIBI)SPECT/CT心肌灌注显像评估缺血性心肌病(ischemic cardiomyopathy,ICM)患者不同缺血程度及不同冠状动脉供血区存活心肌的价值。纳入66例ICM患者,于99mTc-MIBI心肌灌注显像当日行99mTc-HL91乏氧显像、次日行18F-FDG心肌代谢显像。将左心室心肌分为17个节段,分析99mTc-MIBI心肌灌注显像与99mTc-HL91乏氧显像的放射性分布情况,根据结果将ICM患者缺血心肌节段分为存活心肌节段和坏死心肌节段,并与金标准对比。采用四格表法计算99mTc-HL91乏氧显像对ICM患者不同缺血程度及不同冠状动脉供血区存活心肌的诊断效能。66例ICM患者共1122个心肌节段,99mTc-MIBI心肌灌注显像提示,正常心肌节段304个,缺血心肌节段818个。99mTc-HL91乏氧显像提示,存活心肌节段514个,坏死心肌节段304个;18F-FDG心肌代谢显像提示,存活心肌节段641个,坏死心肌节段177个。99mTc-HL91乏氧显像在轻中度缺血组、重度缺血伴梗死组间诊断的敏感度、准确率差异均有统计学意义(均<0.001),特异性差异无统计学意义(=1.000)。99mTc-HL91乏氧显像诊断敏感度、准确率在左前降支组、左回旋支组组间比较,差异均无统计学意义(分别为0.121、0.653),在左前降支组、右冠状动脉组组间(均<0.001)或左回旋支组、右冠状动脉组组间比较,差异均有明显统计学意义(均<0.001),特异性在各组间差异均无统计学意义(均为1.000)。99mTc-HL91乏氧显像结合99mTc-MIBI心肌灌注显像可判断缺血心肌的存活状态,对于存在左冠状动脉病变或重度心肌缺血伴梗死的ICM患者存活心肌的评估有较高的临床价值;对于单纯轻中度缺血或右冠状动脉病变的患者诊断价值相对较低。
乏氧显像;心肌灌注显像;心肌代谢显像;缺血性心肌病;存活心肌
冠心病是全世界人口最主要的死亡原因之一,其发病率逐年提高,已成为心力衰竭的主要病因[1-3]。而缺血性心肌病(ischemic cardiomyopathy,ICM)是冠心病的晚期阶段,指长期心肌缺血导致心肌细胞减少、坏死、纤维化,从而产生心脏功能受损,引起心脏扩大、心力衰竭、严重的心律失常等一系列表现的临床综合征,严重者可导致心肌梗死及心源性猝死等心脏不良事件。ICM患者中存在冬眠心肌、顿抑心肌和坏死心肌,前两者即为存活心肌。研究表明,有存活心肌的患者会从血运重建术中受益,可明显改善其左心室射血分数以及存活率[4-6]。存活心肌数量越多,血运重建后获益越多,尤其当存活心肌>10%时[7-8]。因此,准确地评估ICM患者的存活心肌对其行血运重建、改善预后有重要的意义。锝-99m-甲氧基异丁基异腈(technetium-99m labeled sestamibi,99mTc-MIBI)心肌灌注显像可以准确评估心肌是否缺血,但无法判断心肌是否存活[9]。2-氟-18-氟-2-脱氧-D-葡萄糖(18F-fludeoxyglucose,18F-FDG)PET/CT心肌代谢显像是无创性精准评估存活心肌的金标准,但其价格昂贵、半衰期短,在临床中应用较少[10]。锝-99m-4,9-二氮-3,3,10,10-四甲基十二烷-2,11-二酮肟(99mTc-4,9-diaza-3,3,10,10-tetramethyldodecan-2,11- dione dioxime,99mTc-HL91)是一种新型耐缺氧心肌显像剂,价格便宜,获取方式简单,它在缺血存活的心肌细胞中具有较高的摄取,呈“阳性”显像,但在坏死或正常组织中几乎不摄取,结合心肌灌注显像,可迅速准确地鉴别缺血存活心肌和坏死心肌[11-13]。本研究以18F-FDG心肌代谢显像为金标准,旨在分析99mTc-HL91乏氧显像结合99mTc-MIBI心肌灌注显像评估ICM患者存活心肌的应用价值。
1 资料与方法
1.1 临床资料
前瞻性选取2020年7月至2022年2月期间,在桂林医学院附属医院就诊时确诊冠心病、心功能纽约心脏病协会(New York Heart Association,NYHA)Ⅱ~Ⅳ级,并行99mTc-MIBI静息心肌灌注显像提示心脏扩大且至少满足1个心肌节段存在放射性缺损的ICM患者共66例,其中男42例(63.64%),女24例(36.36%);年龄36~74岁,平均年龄为(51.34±10.78)岁。所有患者均知晓检查情况,自愿参加后续研究并签署知情同意书,于心肌灌注显像当日行99mTc-HL91乏氧显像、次日行18F-FDG心肌代谢显像,检查前2d停服β-受体阻滞剂、血管紧张素转化酶抑制剂、血管紧张素受体拮抗剂等药物。排除标准:①不能耐受检查;②6个月内有脑血管疾病史;③严重心律失常;④先心病、瓣膜病、心肌病;⑤严重呼吸道、肝脏或肾脏疾病。本研究通过桂林医学院附属医院伦理委员会批准(伦理审批号:2021YJSLL-32)。
1.2 显像剂
①99Mo-99mTc发生器由中国原子能科学研究所同位素研究所生产,产生的99mTc核素纯度>99%。MIBI和HL91由北京欣科思达医药科技有限公司提供,将新鲜的740~925MBq99mTcO4-淋洗液注入注射用MIBI冻干瓶中,静置10min,充分溶解后煮沸15min,得到99mTc-MIBI;②将新鲜的740~925MBq99mTcO4-淋洗液注入注射用HL91冻干瓶中,静置10min,得到99mTc-HL91;③18F-FDG:由桂林医学院附属医院核医学科回旋加速器GE PETtrace 800自主生产提供,以18O-H2O为靶材料,通过核反应和亲核取代反应得到18F-FDG。以上3种显像剂检测其放化纯均>95%。
1.3 显像仪器、方法与图像处理
1.3.199mTc-MIBI SPECT/CT静息心肌灌注显像 静脉注射99mTc-MIBI 30mCi后30min进食脂餐,1.5h后行门控SPECT心肌灌注显像,采用德国西门子公司Symbia T16 SPECT/CT显像仪,探头围绕患者从右前斜位45°开始到左后斜位45°顺时针旋转180°,25s采集1帧,共32帧图像。采集矩阵为64×64,放大倍数1.33,能峰140keV,窗宽20%。采集结束后,通过计算机软件(Toolbox)对二维图像进行三维重建,最终获得左心室短轴、水平长轴、垂直长轴3个层面的心肌灌注断层图像和极坐标靶心图。
1.3.299mTc-HL91 SPECT/CT心肌乏氧显像 患者做完静息心肌灌注显像时,通知护士在检查床上给患者静脉推注99mTc-HL91 30mCi,嘱患者30min后吃脂餐,2h后行SPECT/CT心肌乏氧显像,显像方法及图像处理同99mTc-MIBI静息心肌灌注显像。
1.3.318F-FDG PET/CT心肌代谢显像 采用荷兰飞利浦Ingenuity TF PET/CT仪,于99mTc-MIBI静息心肌灌注后次日行心肌代谢显像。显像前患者禁食8~12h,晨起测定其空腹血糖,根据是否为糖尿病患者及血糖水平,口服葡萄糖5~40g(若血糖过高,同时皮下或静脉注射胰岛素),45~60min后测血糖,若血糖≤7.8mmol/L,则随即注射18F-FDG;若血糖>7.8mmol/L,则继续皮下或静脉注射胰岛素,直至血糖≤7.8mmol/L,方可注射18F-FDG。静脉注射18F-FDG 5mCi,1h后行门控PET/CT显像,每个心动周期采集8帧,矩阵576×576,能峰511keV,采用3D采集1个床位(10min)。
1.4 图像分析与判定标准
所有图像均由2位核医学主治以上职称医师独立分析,诊断一致时方可认为有效;诊断不一致时由2人协商达成相同诊断结果。根据美国心脏病协会(American Heart Association,AHA)指南将左心室心肌分为17节段(图1)[14]。所有心肌节段按照软件自动生成评分结合诊断医生视觉半定量分析,采用5分制评分法进行评估。0分:放射性分布正常;1分:放射性分布轻度稀疏;2分:放射性分布中度稀疏;3分:放射性分布重度稀疏;4分:放射性分布缺损。判定标准:以18F-FDG心肌代谢显像为判断存活心肌的金标准(图2),99mTc-MIBI心肌灌注显像中,有放射性分布稀疏或缺损的心肌节段,18F-FDG心肌代谢显像相应节段的显像剂摄取增加,为灌注/代谢不匹配,表明该心肌节段为存活心肌;18F-FDG心肌代谢显像相应节段的显像剂仍为稀疏或缺损,为灌注/代谢匹配,表明该心肌节段为坏死心肌。99mTc-HL91乏氧显像(图3):99mTc-MIBI心肌灌注显像中,有放射性分布稀疏或缺损的心肌节段,99mTc-HL91乏氧显像有放射性明显回填,即“阳性”显像,则判定为存活心肌;若无放射性回填,即“阴性”显像,则判定为坏死心肌。

图1 左心室心肌17节段靶心图
66例ICM患者共1122个心肌节段,2位医师分别对99mTc-HL91乏氧显像及18F-FDG心肌代谢显像图像进行双盲分析,诊断一致时方可认为有效,诊断不一致时由两位医师协商得出一致结果。
将所有缺血心肌节段按照冠状动脉供血区分为左前降支(left anterior descending artery,LAD)组332个、左回旋支(left circumflex artery,LCX)组296个、右冠状动脉(right coronary artery,RCA)组190个。
1.5 统计学方法


图2 18F-FDG心代谢显像图
注:黄色箭头,灌注/代谢不匹配,代表存活心肌节段;红色箭头,灌注/代谢匹配,代表坏死心肌节段
注:黄色箭头,99mTc-HL91乏氧显像放射性回填,代表存活心肌节段;红色箭头,99mTc-HL91乏氧显像放射性缺损,代表坏死心肌节段
2 结果
2.1 99mTc-HL91乏氧显像与18F-FDG心肌代谢显像结果
99mTc-MIBI心肌灌注显像提示正常心肌节段(0分)304个,缺血心肌节段(1~4分)818个。99mTc-HL91乏氧显像提示存活心肌节段514个,坏死心肌节段304个;18F-FDG心肌代谢显像提示存活心肌节段641个,坏死心肌节段177个,见表1。

表1 99mTc-HL91乏氧显像与18F-FDG心肌代谢显像结果统计
注:“+”代表存活心肌节段,“–”代表坏死心肌节段
2.2 99mTc-HL91乏氧显像对不同缺血程度存活心肌的诊断效能
将所有缺血心肌节段按照缺血程度分为轻中度缺血组(1~2分)544个,重度缺血伴梗死组(3~4分)274个。99mTc-HL91乏氧显像在轻中度缺血组、重度缺血伴梗死组检测存活心肌的敏感度、特异性、准确率分别为77.0%、100%、79.2%和90.6%、100%、94.9%。两组组间诊断敏感度、准确率差异均有统计学意义(2分别为13.259、34.084,均<0.001),特异性差异无统计学意义(2=0,=1.000),见表2。

表2 99mTc-HL91乏氧显像对不同缺血程度存活心肌的诊断效能(%)
2.3 99mTc-HL91乏氧显像对不同冠状动脉供血区存活心肌的诊断效能
99mTc-HL91乏氧显像在LAD组、LCX组、RCA组检测存活心肌的敏感度、特异性、准确率分别为89.9%、100%、91.6%,85.2%、100%、90.5%和59.2%、100%、62.6%。敏感度、准确率在LAD组、LCX组组间比较,差异均无统计学意义(2分别为2.398、0.203,分别为0.121、0.653),在LAD组、RCA组组间(2分别为59.091、65.830,均<0.001)或LCX组、RCA组组间比较,差异均有统计学意义(2分别为30.852、55.568,均<0.001),特异性在各组间差异均无统计学意义(2均为0,均为1.000),如表3。
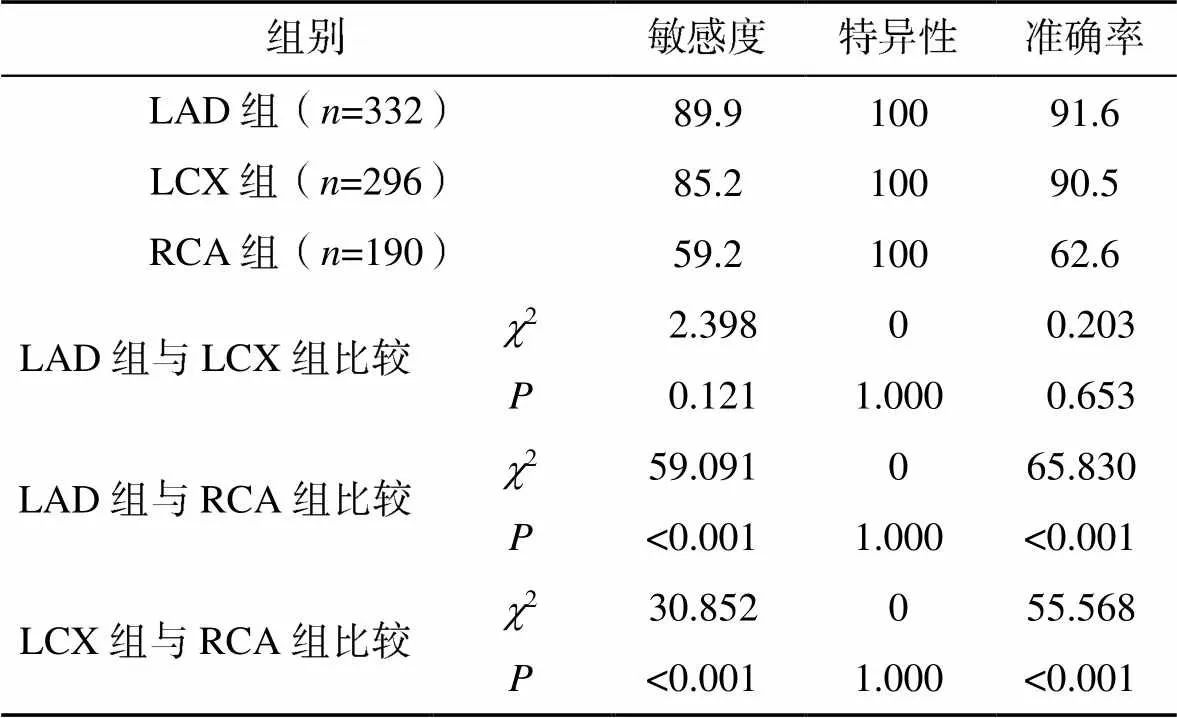
表3 99mTc-HL91乏氧显像对不同冠状动脉供血区存活心肌的诊断效能(%)
3 讨论
由冠状动脉狭窄或闭塞后慢性心肌缺血所导致的ICM属于冠心病的一种特殊类型,是全球范围内患者死亡和伤残的重要原因。且已逐渐上升为心力衰竭的主要病因[15]。ICM患者根据心肌缺血发生的速度、范围、程度以及侧支循环建立等不同,心肌细胞的损害会出现3种情况:一是坏死心肌,即不可逆的心肌损害,即使冠状动脉血流恢复,心肌也不可能再复活;二是冬眠心肌,是当慢性持续性心肌缺血时,心肌细胞通过代偿,降低耗氧量及代谢速度,以使心肌细胞保持存活状态;三是顿抑心肌,指短暂急性心肌缺血后的一过性收缩功能障碍,心肌组织和细胞尚未坏死。当冠状动脉再通血流恢复后,冬眠心肌和顿抑心肌功能可逐步恢复正常,即为存活心肌。存活心肌的存在和范围可以预测血运重建术后收缩功能恢复的可能性[16]。与单纯药物治疗相比,有存活心肌的ICM患者行血运重建治疗后存活率更高,反之这部分患者发生死亡或心脏不良事件的风险将明显提高[17-18]。因此,准确评估ICM患者缺血心肌是否存活对其治疗决策以及预后判断具有重要的临床意义。
18F-FDG PET/CT心肌代谢显像是诊断存活心肌的金标准,但由于检查费用高及设备普及率低,因此未能在临床中广泛使用。99mTc-MIBI作为国内最常用的心肌灌注显像剂,是一种脂溶性、小分子的单价阳离子,半衰期短、辐射剂量小,可通过发生器获得,制备方便,静脉注射后可通过被动弥散方式进入心肌细胞,与细胞线粒体相结合,其在心肌内的分布与心肌血流量呈正比。因此,通过其在心肌内的分布情况可准确判断有无心肌缺血。99mTc-HL91是近年来研制的一种非硝基咪唑类单光子新型乏氧组织显像剂,制备简单、价格低廉、不具有细胞毒性,进入存活细胞内后,在细胞内酶的作用下发生单原子还原,产生自由基阴离子[19]。当氧丰富时,自由基阴离子又能被迅速氧化成原化合物并扩散到细胞外;而在乏氧且存活的心肌细胞内,可进一步还原成氮的化合物形式,产物与细胞内组分结合,滞留于细胞内而显像。正常心肌摄取少,坏死心肌不摄取,能提供心肌组织缺氧但存活的直接证据,从而识别缺血但存活的心肌[20-21]。但若其单独显像无法获得整个左心室的轮廓,不能区分正常心肌与坏死心肌(均不显影)。虽然缺血存活心肌呈“热区”显影,但不能判断心肌缺血的部位、程度与面积。本研究通过2种显像结合,优势互补,可有效区分缺血存活心肌和坏死心肌。此外,本研究将心肌灌注显像与心肌代谢显像结合,避免了单纯心肌代谢显像不能区分正常心肌(代谢评分0分)与缺血存活心肌(包含代谢评分0分这种情况)的局限性,可精准识别正常心肌、缺血存活心肌和坏死心肌。
既往研究是通过长时间随访来探讨99mTc-HL91对冠心病患者存活心肌的评价,而本研究分两日法行99mTc-HL91乏氧显像与18F-FDG心肌代谢显像,可实时进行两者对比研究,避免了随时间延长患者心肌结构、活性可能会发生变化,从而导致结果的准确性不佳[22]。本研究结果显示,99mTc-HL91乏氧显像检测存活心肌的特异性为100%,这与既往研究报道相一致[22-23]。本研究有127个心肌节段在99mTc-HL91显像上呈假阴性,原因可能是:①该心肌节段为顿抑心肌,因为心肌顿抑时心肌的氧含量可能是正常的,对99mTc-HL91摄取不敏感[21, 24];②该心肌节段处于长期慢性缺血或陈旧性心肌梗死阶段,心肌修复已完成,氧离子自由基已被清除,不利于99mTc-HL91积聚;③该心肌节段坏死心肌和存活心肌混合存在,体积较小,SPECT/CT分辨率低而不能准确探测。随着心肌缺血程度加重,敏感度、准确率均提高,重度缺血伴梗死组与轻中度缺血组相比有显著差异,因为99mTc-HL91只有在氧含量明显减低时,才能长时间滞留于心肌。而缺血程度较轻时,心肌乏氧相对较轻,对99mTc-HL91摄取不敏感。与LAD组及LCX组相比,RCA组敏感度、准确率较低,原因可能是尽管肝脏对于99mTc-HL91的摄取量较低,但其仍然是主要代谢途径。本研究在注射99mTc-HL91 30min后服脂餐促进肝脏代谢,仍发现所有患者心肌下壁节段均受到肝脏放射性浓聚影响,其他各壁不受影响,而在进行后处理图像时,常规“抠除”了肝脏浓聚处,从而可能导致在图像结果判读时低估了存活的心肌下壁节段。
本研究目前仍存在一些局限:①99mTc-HL91乏氧显像与18F-FDG代谢显像均以半定量法判断心肌活性进行对比研究,缺乏定量指标,可能存在误差;②本研究采用99mTc-MIBI与99mTc-HL91或18F-FDG联合显像,均假设两者之间无相互作用,暂无试验验证;③本研究为单中心研究,样本量较少。
综上所述,99mTc-HL91乏氧显像可识别缺氧但存活的心肌,结合99mTc-MIBI心肌灌注显像可以有效区分缺血存活心肌和坏死心肌,对于存在左冠状动脉病变或缺血程度较重的ICM患者的存活心肌的评估有较高的临床指导价值;对于缺血程度较轻的患者诊断价值一般;而对于单纯右冠状动脉病变的患者意义不大。同时为暂未配备PET/CT的科室提供了评估心肌活性的新方法,优化了医疗资源,值得推广和应用。
[1] RALAPANAWA U, SIVAKANESAN R. Epidemiology and the magnitude of coronary artery disease and acute coronary syndrome: a narrative review[J]. J Epidemiol Glob Health, 2021, 11(2): 169–177.
[2] LIANG F, WANG Y. Coronary heart disease and atrial fibrillation: a vicious cycle[J]. Am J Physiol Heart Circ Physiol, 2021, 320(1): H1–H12.
[3] PAGLIARO B R, CANNATA F, STEFANINI G G, et al. Myocardial ischemia and coronary disease in heart failure[J]. Heart Fail Rev, 2020, 25(1): 53–65.
[4] NAMDAR M, RAGER O, PRIAMO J, et al. Prognostic value of revascularising viable myocardium in elderly patients with stable coronary artery disease and left ventricular dysfunction: a PET/CT study[J]. Int J Cardiovasc Imaging, 2018, 34(10): 1673–1678.
[5] PANZA J A, CHRZANOWSKI L, BONOW R O. Myocardial viability assessment before surgical revascularization in ischemic cardiomyopathy: jacc review topic of the week[J]. J Am Coll Cardiol, 2021, 78(10): 1068–1077.
[6] TSAO C W, ADAY A W, ALMARZOOQ Z I, et al. Heart disease and stroke statistics-2022 update: a report from the American Heart Association[J]. Circulation, 2022, 145(8): e153–e639.
[7] 崔雅丽, 刘海燕, 秦锐锐, 等. 核素心肌显像对急性心肌梗死患者PTCA后左心室收缩功能变化的评估价值[J].国际放射医学核医学杂志, 2020, 44(3): 137–142.
[8] LING L F, MARWICK T H, FLORES D R, et al. Identification of therapeutic benefit from revascularization in patients with left ventricular systolic dysfunction: inducible ischemia versus hibernating myocardium[J]. Circ Cardiovasc Imaging, 2013, 6(3): 363–372.
[9] FALLAHI B, HAGHIGHATAFSHAR M, FARHOUDI F, et al. Comparative evaluation of the diagnostic accuracy of99mTc-sestamibi gated SPECT using five different sets of image acquisitions at stress and rest phases for the diagnosis of coronary artery disease[J]. Am J Nucl Med Mol Imaging, 2013, 4(1): 10–16.
[10] MURTHY V L, BATEMAN T M, BEANLANDS R S, et al. Clinical quantification of myocardial blood flow using PET: joint position paper of the SNMMI cardiovascular council and the ASNC[J]. J Nucl Med, 2018, 59(2): 273–293.
[11] 李艳郧, 刘刚, 吴立兵, 等. 用99Tm-HL91评价鼠心肌缺血模型[J]. 中华核医学杂志, 2006, 26(5): 280–281.
[12] 朱卓豪, 牟兴宇, 卢彦祺, 等.99mTc-TF心肌灌注显像联合99Tcm-HL91乏氧显像评价SMI患者的存活心肌[J]. 标记免疫分析与临床, 2019, 26(11): 1822–1826.
[13] 蒋泽文, 卢彦祺, 牟兴宇, 等.99mTc-TF联合99mTc-HL91心肌显像评估隐匿型冠心病患者预后价值[J]. 标记免疫分析与临床, 2019, 26(9): 1518–1523.
[14] CERQUEIRA M D, WEISSMAN N J, DILSIZIAN V, et al. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association[J]. Circulation, 2002, 105(4): 539–542.
[15] PERERA D, CLAYTON T, PETRIE M C, et al. Percutaneous revascularization for ischemic ventricular dysfunction: rationale and design of the REVIVED- BCIS2 trial: percutaneous coronary intervention for ischemic cardiomyopathy[J]. JACC Heart Fail, 2018, 6(6): 517–526.
[16] PARIKH K, CHOY-SHAN A, GHESANI M, et al. Multimodality imaging of myocardial viability[J]. Curr Cardiol Rep, 2021, 23(1): 5.
[17] GARATTI A, CASTELVECCHIO S, CANZIANI A, et al. CABG in patients with left ventricular dysfunction: indications, techniques and outcomes[J]. Indian J Thorac Cardiovasc Surg, 2018, 34(Suppl 3): 279–286.
[18] KHALAF S, CHAMSI-PASHA M, AL-MALLAH M H. Assessment of myocardial viability by PET[J]. Curr Opin Cardiol, 2019, 34(5): 466–472.
[19]KINUYA S, YOKOYAMA K, KONISHI S, et al. Increased uptake of99mTc-HL91 in tumor cells exposed to X-ray radiation[J]. Ann Nucl Med, 2000, 14(2): 139–141.
[20] OKADA R D, JOHNSON G R, NGUYEN K N, et al.99mTc-HL91: “hot spot” detection of ischemic myocardium in vivo by gamma camera imaging[J]. Circulation, 1998, 97(25): 2557–2566.
[21] IMAHASHI K, MORISHITA K, KUSUOKA H, et al. Kinetics of a putative hypoxic tracer,99mTc-HL91, in normoxic, hypoxic, ischemic, and stunned myocardium[J]. J Nucl Med, 2000, 41(6): 1102–1107.
[22] LIU M, MA Z, GUO X, et al. Technetium-99m-labelled HL91 and technetium-99m-labelled MIBI SPECT imaging for the detection of ischaemic viable myocardium: a preliminary study[J]. Clin Physiol Funct Imaging, 2012, 32(1): 25–32.
[23] 邓波,梁锐,陈小凤.99mTc-HL91乏氧显像与硝酸甘油介入99mTc-MIBI心肌显像检测存活心肌的对比分析[J]. 广东医学, 2007, 28(1): 76–78.
[24] 张弘, 蒋宁一. 心肌乏氧显像及其临床应用[J]. 国外医学(放射医学核医学分册), 2004, 28(3): 113–117.
Application of SPECT/CT imaging in the evaluation of viable myocardium in patients with ischemic cardiomyopathy
Department of Nuclear Medicine, Affiliated Hospital of Guilin Medical College, Guilin 541001, Guangxi, China
18F-fluorodeoxyglucose (18F-FDG) PET/CT myocardial metabolic imaging was used as the gold standard, to investigate the value of technetium-99m labeled 4,9-diaza-3,3,10,10-tetramethyldodecan-2,11-dione dioxime (99mTc-HL91) single-photon emission computed tomography/computed tomography (SPECT/CT) hypoxia imaging combined with technetium-99m labeled sestamibi (99mTc-MIBI) SPECT/CT myocardial perfusion imaging in the evaluation of viable myocardium with different degrees of ischemia and different coronary blood supply areas in patients with ischemic cardiomyopathy (ICM).99mTc-HL91 hypoxia imaging was performed on the same day as99mTc-MIBI myocardial perfusion imaging, and18F-FDG myocardial metabolism imaging was performed the next day in 66 patients with ICM. The left ventricular myocardium was divided into 17 segments. The radioactivity distribution of99mTc-MIBI and99mTc-HL91 was analyzed. According to the results, ischemic myocardial segments were divided into viable segments and necrotic segments, and the results were compared with gold standard. The diagnostic efficacy of99mTc-HL91 hypoxia imaging in the evaluation of different degrees of ischemia and different coronary blood supply areas in patients with ICM was calculated by four-grid method.There were a total of 1122 myocardial segments in 66 patients with ICM were analyzed.99mTc-MIBI myocardial perfusion imaging showed 304 normal and 818 ischemic myocardial segments. Of these,99mTc-HL91 hypoxia imaging showed 514 viable myocardial segments and 304 necrotic myocardial segments, and18F-FDG myocardial metabolism imaging showed 641 viable myocardial segments and 177 necrotic myocardial segments. There were statistically significant differences in diagnostic sensitivity and accuracy between the mild to moderate ischemia group and severe ischemia with infarction group (all<0.001), but there were no statistical difference in specificity between the two groups(=1.000). There were no statistical differences in sensitivity and accuracy between the left anterior descending artery group and left circumflex branch group (were 0.121, 0.653), but there were statistically significant differences between the left anterior descending artery group and right coronary artery group (all<0.001) and between the left circumflex branch group and right coronary artery group (all<0.001). There were no statistical differences in specificity between the three groups (all=1.000).99mTc-HL91 hypoxia imaging combined with99mTc-MIBI perfusion imaging is an effective method for evaluating the survival state of ischemic myocardium, and has great clinical value for the evaluation of viable myocardium in ICM patients with left coronary lesions or severe myocardial ischemia with infarction. However, the diagnostic value of combination imaging in patients with mild to moderate ischemia or with right coronary artery lesions is lower.
Hypoxia imaging; Myocardial perfusion imaging; Myocardial metabolic imaging; Ischemic cardiomyopathy; Viable myocardium
R81
A
10.3969/j.issn.1673-9701.2023.29.008
广西医疗卫生适宜技术开发与推广应用项目(S2020111)
付巍,电子信箱:380015540@qq.com
(2022–12–19)
(2023–09–06)