二磷酸腺苷受体抑制剂对老年冠心病合并糖尿病患者冠状动脉造影介入术后抗栓作用评价
2023-06-28陆赋斌蔡小琴孙永毅吴忠旭董萍
陆赋斌 蔡小琴 孙永毅 吴忠旭 董萍


摘 要 目的:評价不同二磷酸腺苷(ADP)受体抑制剂对老年冠心病合并糖尿病患者冠状动脉造影介入术(PCI)后疗效。方法:收集2021年1月至12月行PCI术的老年冠心病合并糖尿病患者145例,分为术后口服替格瑞洛(90 mg 每天2次)治疗组66例和氯吡格雷(75 mg每天2次)治疗组79例。用血栓弹力图评价ADP诱导的血小板抑制率以及随访12个月因再次入院接受血管重建术事件。结果:替格瑞洛组抑制血小板聚集率[8.1(1.4~28.8)]效果优于氯吡格雷组[42.2(21.8~59.8)],组间差异有统计学意义(P<0.001)。氯吡格雷是血小板高反应性的独立预测因子。生存曲线显示替格瑞洛能延缓老年冠心病合并糖尿病患者PCI术后血管重建,但差异无统计学意义(HR=0.473,95% CI:0.183~1.227,Log-rank P=0.147)。结论:替格瑞洛具有更明显的血小板抑制率,能明显减少老年冠心病合并糖尿病患者PCI术后HPR发生率,并能降低PCI术后1年内的血管重建率,延缓血运重建时间。
关键词 冠心病;糖尿病;替格瑞洛;氯吡格雷;血小板聚集率
中图分类号:R459.7 文献标志码:A 文章编号:1006-1533(2023)06-0031-04
引用本文 陆赋斌, 蔡小琴, 孙永毅, 等. 二磷酸腺苷受体抑制剂对老年冠心病合并糖尿病患者冠状动脉造影介入术后抗栓作用评价[J]. 上海医药, 2023, 44(6): 31-34.
Anti-thrombolytic evaluation of adenosine diphosphate receptor inhibitor in elderly patients with coronary heart disease and diabeteson after percutaneous coronary intervention
LU Fubin1, CAI Xiaoqin1, SUN Yongyi2, WU Zhongxu3, DONG Ping4
(1. Department of Pharmacy; 2. Changlong General Practitioner Team; 3. Changyang General Practitioner Team; 4. Department of Endocrinology of Daqiao Community Health Service Center of Yangpu District, Shanghai 200093, China)
ABSTRACT Objective: To evaluate the clinical efficacy of different adenosine diphosphate(ADP) receptor inhibitors in elderly patients with coronary heart disease and diabetes after percutaneous coronary intervention(PCI). Methods: One hundred and forty-five elderly patients with coronary heart disease and diabetes who underwent PCI were collected from January to December 2021, and divided into the treatment group of postoperative oral ticagrelor(90 mg twice a day) with 66 cases, the treatment group of clopidogrel(75 mg twice a day) with 79 cases. Thromboelastogram was used to evaluate the platelet inhibition rate induced by ADP and the event of re admission to hospital for vascular reconstruction after 12 months of follow-up. Results: The inhibitory effect of ticagrelor group on platelet aggregation rate[8.1 (1.4-28.8)] was better than that of clopidogrel group[42.2(21.8-59.8)], and the difference between groups was statistically significant(P<0.001). Clopidogrel was an independent predictor of platelet hyperreactivity. The survival curve showed that ticagrelor could delay vascular reconstruction after PCI in elderly patients with coronary heart disease and diabetes, but there was no significant difference(HR=0.473, 95% CI: 0.183-1.227, log rank P=0.147). Conclusion: Ticagrelor has a more obvious platelet inhibition rate, and can significantly reduced the incidence of HPR in the elderly with coronary heart disease and diabetes after PCI, also reduce the rate of vascular reconstruction within 1 year after PCI, and delay the time of blood circulation reconstruction.
KEY WORDS coronary heart disease; diabetes; ticagrelor; clopidogrel; platelet aggregation
冠状动脉粥样硬化性心脏病是人类死亡的主要病因之一,其病理生理学机制是冠状动脉(冠脉)因长期粥样硬化导致冠脉阻塞,致使心肌细胞长期缺血和缺氧,最终因心肌细胞坏死致心脏衰竭[1-2]。目前,支架置入术已经成为最有效改善冠脉狭窄的方法,但由于介入手术会导致内皮受损,支架植入术后易导致血小板聚集,发生支架内血栓,再发血栓事件[3]。为了预防支架植入术后血栓发生,指南推荐在冠脉造影支架植入术(percutaneous coronary intervention,PCI)后使用阿司匹林联合二磷酸腺苷(adenosine diphosphate,ADP)受体拮抗剂抗栓治疗至少12个月[4]。在PLATO研究中,相较于氯吡格雷,替格瑞洛能通过增加血小板抑制率减少支架术后血栓以及主要心血管不良事件(major adverse cardiovascular events,MACE)的发生率,亚组分析结果显示,冠心病合并糖尿病(diabetes mellitus,DM)患者应用替格瑞洛亦能减少血栓事件发生[5]。目前,欧美国家及中国等多项指南均将替格瑞洛作为急性冠脉综合征(acute coronary syndrome,ACS)患者PCI术后抗栓治疗的一线推荐用药,2017年欧洲心脏病学会(European Society of Cardiology,ESC)对拟行PCI的稳定性冠心病患者优先推荐替格瑞洛[6]。
对于老年患者,因其内皮功能退化导致血栓风险增加,同时合并肝肾功能逐步退化,增加药物个体间代谢差异,因此对于老年冠心病合并DM患者行PCI术后的抗栓治疗需要尤其谨慎[6]。目前对于老年冠心病合并DM患者抗栓治疗研究较少,本研究通过临床前瞻性病例对照研究评价不同ADP受体抑制剂对于老年冠心病合并糖尿病患者PCI术后的疗效。
1 资料与方法
1.1 一般资料
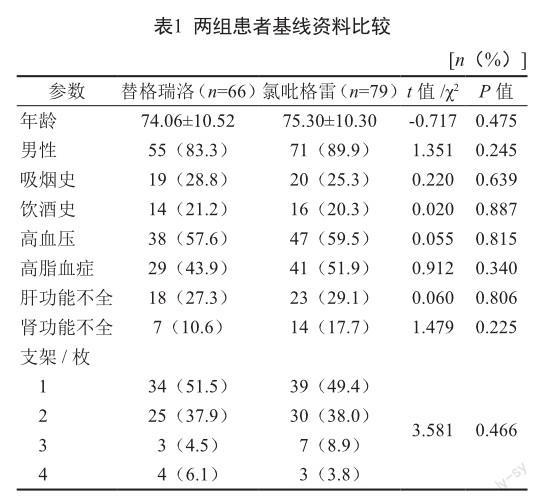
本研究为单中心、前瞻性病例对照研究。收集2021年1月至12月行PCI术的老年冠心病合并2型DM患者145例,均经皮冠脉造影确诊狭窄超过70%,空腹血糖>7 mmol或者正在服用口服降糖药。患者根据术后所用ADP受体抑制剂类型分为替格瑞洛(阿斯利康制药有限公司)治疗组66例和氯吡格雷(赛诺菲制药有限公司)治疗组79例,两组一般资料包括年龄、性别、合并症(高血压、高血脂以及糖尿病等)以及支架植入信息等具可比性,见表1。排除出血史不能耐受长期抗栓治疗者。对患者进行12个月随访,收集发生的因再次入院接受血管重建术事件。
1.2 方法
替格瑞洛組患者术后口服阿司匹林(拜耳医药保健有限公司)100 mg每天1次和替格瑞洛90 mg每天2次;氯吡格雷组患者术后口服阿司匹林100 mg每天1次和氯吡格雷75 mg,每天2次。两组患者服用上述抗血小板药物至少1年,后根据随访情况决定是否停用ADP受体抑制剂。若无禁忌,建议患者终身服用阿司匹林。
患者出院后(30±5)d至医院门诊进行随访,取空腹静脉血,置于含3.8%枸橼酸钠或浓度>14.51 IU肝素的真空管内,弃用前2~3 mL全血后,采血至试管刻度线,共2 mL时停止采血。将采血管轻轻上、下颠倒3~5次,确保全血与抗凝剂充分混合。将血样送实验室,在全自动血栓弹力图仪TEG 5000(美国Haemoscope公司)上进行血栓弹力图(thrombelastography,TEG)检测。将血小板聚集抑制率(inhibition of platelet aggregation,IPA)<30%定义为血小板高反应性(high on-treatment platelet reactivity,HPR);IPA≥30%为血小板低反应性(low on-treatment platelet reactivity,LPR)[7-8]。
1.3 统计学分析
采用SPSS 23.0软件进行统计分析,计量资料用平均值±标准差表示,行t检验;计数资料用百分率(%),行卡方检验。两组患者ADP诱导血小板抑制率用t检验,用非条件logistic回归进行多因素分析HPR,利用生存曲线分析两种不同ADP受体抑制剂对MACE影响。以P<0.05表示差异有统计学意义。
2 结果
2.1 两组血小板抑制率比较
替格瑞洛组抑制血小板聚集率为8.1(1.4~28.8),效果优于氯吡格雷组的42.2(21.8~59.8),组间差异有统计学意义(P<0.001)。且HPR发生率明显低于氯吡格雷组(24.2%比60.8%,P<0.001)。将HPR单因素回归分析中P<0.1的变量纳入多因素回归分析,显示相较于替格瑞洛,氯吡格雷是HPR的独立预测因子(表2)。
2.2 两组心血管事件比较
在12个月的随访期间,替格瑞洛组和氯吡格雷组中分别有5例和12例患者因血管再狭窄再次入院接受血管重建术(7.6%比15.2%,OR=0.458,95% CI:0.152~1.374,P=0.156)。生存曲线显示替格瑞洛能延缓老年冠心病合并2型DM患者PCI术后血管重建,但差异无统计学意义(HR=0.473,95% CI:0.183~1.227,Log-rank P=0.147)(图1)。
3 讨论
DM通过多种机制导致血小板功能障碍,包括高血糖、氧化应激、胰岛素抵抗、炎症反应等,并且影响着冠脉粥样硬化的发生与发展[7]。DM是一种进行性的疾病,在PCI后,DM持续刺激血小板活化,导致MACE发生[8]。已证实双联抗血小板治疗(dual anti-platelet therapy,DAPT)可以显著降低PCI术后MACE的发生率,并可改善冠脉内皮功能与炎症水平[9-10]。同时,老年患者的内皮受损严重程度显著高于年轻患者,因此,对于老年冠心病合并DM患者更需强化抗栓治疗。本研究结果表明,在标准DAPT治疗下,患者可以从阿司匹林与替格瑞洛中获益。尽管氯吡格雷是最为广泛使用的ADP受体抑制剂,替格瑞洛在急性冠脉综合征中的疗效显著优于氯吡格雷[5]。而在DM患者中,替格瑞洛的获益可能是由于高糖状态下氯吡格雷代谢受损,使氯吡格雷的代谢产物减少[11]。
THEMIS大型随机双盲试验显示,对于稳定性心绞痛合并2型DM患者,替格瑞洛合并阿司匹林的抗血小板治疗相较于阿司匹林单抗治疗能显著降低缺血性心血管事件的发生率(7.7%比8.5%,HR=0.90,95% CI:081~0.99,Log-rank P=0.04)[12]。THEMIS-PCI试验选取THEMIS试验中行PCI术的患者进行亚组分析,以替格瑞洛为基础的DAPT能进一步增加临床获益[13]。相反,CHARISMA研究则提示了在与上述相同的人群中,相较于单抗治疗,用阿司匹林合并氯吡格雷治疗未能提供益处,且增加了一定的出血风险[14]。本研究结果显示相较于氯吡格雷,替格瑞洛具有更明显的血小板抑制率,能明显减少老年冠心病合并DM患者PCI术后HPR发生率,并能降低PCI术后1年内的血管重建率,延缓血运重建时间。
DM患者的抗栓治疗管理存在着一系列挑战。DM患者存在连续的心血管风险,然而,强化抗栓治疗的人群、持续时间尚无定论。未来应开发基于冠心病合并DM人群的缺血、出血评分,以提升患者的获益。其次,抗栓治疗的药物选择也存在一定的争议。有学者建议用低剂量的替格瑞洛(60 mg)与阿司匹林的DAPT,在有效抑制缺血事件的同时降低出血的临床结局,但仍需更大型的临床研究。最后,患者对药物的依从性也是挑战之一,这将影响患者的长期预后。
参考文献
[1] 沈迎, 张瑞岩, 沈卫峰. 稳定性冠状动脉粥样硬化心脏病血运重建策略研究进展[J]. 国际心血管病杂志, 2016, 43(6): 321-325; 344.
[2] Tian Y, Deng P, Li B, et al. Treatment models of cardiac rehabilitation in patients with coronary heart disease and related factors affecting patient compliance[J]. Rev Cardiovasc Med, 2019, 20(1): 27-33.
[3] 楊宇进, 王贺阳, 李毅, 等. 老龄对冠心病患者药物洗脱支架植入术后净临床不良事件发生风险影响[J]. 临床军医杂志, 2017, 45(6): 570-574.
[4] Wang HY, Dou KF, Wang Y, et al. Benefit-risk profile of dapt continuation beyond 1 year after PCI in patients with high thrombotic risk features as endorsed by 2018 ESC/EACTS myocardial revascularization guideline[J]. Cardiovasc Drugs Ther, 2020, 34(5): 663-675.
[5] Wallentin L, Becker RC, Budaj A, et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes[J]. N Engl J Med, 2009, 361(11): 1045-1057.
[6] Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC)[J]. Eur Heart J, 2018, 39(2): 119-177.
[7] Knapp M, Tu X, Wu R. Vascular endothelial dysfunction, a major mediator in diabetic cardiomyopathy[J]. Acta Pharmacol Sin, 2019, 40(1): 1-8.
[8] Armstrong EJ, Waltenberger J, Rogers JH. Percutaneous coronary intervention in patients with diabetes: current concepts and future directions[J]. J Diabetes Sci Technol, 2014, 8(3): 581-589.
[9] Zeymer U, Becher A, Jennings E, et al. Systematic review of the clinical impact of dual antiplatelet therapy discontinuation after acute coronary syndromes[J]. Eur Heart J Acute Cardiovasc Care, 2017, 6(6): 522-531.
[10] Li J, Li Y, Qiu M, et al. Impact of dual antiplatelet therapy duration on 1-year clinical outcomes in diabetic patients with acute coronary syndrome undergoing percutaneous coronary intervention: Insights from the real-world OPT-CAD study[J]. Catheter Cardiovasc Interv, 2020, 95 Suppl 1: 579-586.
[11] Ferreiro JL, Angiolillo DJ. Diabetes and antiplatelet therapy in acute coronary syndrome[J]. Circulation, 2011, 123(7): 798-813.
[12] Steg PG., Bhatt DL., Simon T, et al. Ticagrelor in patients with stable coronary disease and diabetes[J]. N Engl J Med, 2019, 381(14): 1309-1320.
[13] Bhatt DL, Steg PG, Mehta SR, et al. Ticagrelor in patients with diabetes and stable coronary artery disease with a history of previous percutaneous coronary intervention(THEMISPCI): A phase 3, placebo-controlled, randomised trial[J]. Lancet, 2019, 394(10204): 1169-1180.
[14] Bhatt DL, Fox KA, Hacke W, et al. Clopidogrel and aspirin versus aspirin alone for the prevention of atherothrombotic events[J]. N Engl J Med, 2006, 354(16): 1706-1717.
