Innovative combined therapy for multiple keloidal dermatofibromas of the chest wall: A novel case report
2023-01-13JiahuaXingYiChenLiwuZhengYanShaoYichiXuLingliGuo
Jiahua Xing ,Yi Chen ,Liwu Zheng ,Yan Shao ,Yichi Xu ,Lingli Guo
a Department of Plastic and Reconstructive Surgery,The First Medical Center,Chinese PLA General Hospital,Beijing 100853,China
b School of Medicine,Nankai University,Tianjin 300071,China
c Department of Burn and Plastic Surgery,No.988 Hospital of Chinese PLA,Zhengzhou 450042,Henan,China
Keywords:Keloidal dermatofibroma Combined therapy Chest wall Differential diagnosis Postoperative radiotherapy
ABSTRACT Dermatofibromas are benign soft tissue tumors that predominantly affect the limbs,and more rarely the chest.Keloidal dermatofibroma is a rare subtype with distinct clinicopathological features and an aggressive clinical course.By researching the evolution of the disease in this study,we aimed to summarize our experience of managing a rare patient who underwent five surgeries for keloidal dermatofibroma that developed sequentially in the upper arm and chest and propose a novel treatment for keloidal dermatofibroma.We concluded that keloidal dermatofibroma involving larger areas,high tension sites,and multiple localizations can be treated using the principles of pathological scar management.
1.Introduction
Keloids are pathological scar tissue and fibrous proliferative skin lesions which occur secondary to skin trauma or form spontaneously.1Dermatofibroma,a common benign skin tumor,has many variants owing to its broad spectra,such as sclerosing hemangioma and hemangiopericytoma-like fibrous histiocytoma.2Dermatofibromas are usually simple to diagnose and occur most frequently in the extremities and more rarely in the chest and face.According to a previous study,the most common subtype of dermatofibroma is fibrous histiocytoma,while keloidal dermatofibroma is rarer (about 1%).3This new variant of keloidal dermatofibroma was first reported in China in 1998 by Kuo et al.Its clinical presentation was similar to that of common dermatofibroma.Microscopically,the tumor was located superficially under the epidermis.The authors discovered focal hemorrhages,iron-containing heme deposits,and a variable number of multinucleated giant cell reactions in the superficial or central regions of the tumor,as well as typical dermatofibroma morphology at the base of the tumor or surrounding it.4Immunohistochemical results showed scattered KiM1P-,CD68-,and Mac387-positive and factor XIIIa-negative or CD34-negative cells in the keloid region.Although the clinical presentation was similar to that of keloids,Kuo et al.concluded that this variant of dermatofibroma should not be overlooked as a simple scar.They suggested that keloidal dermatofibroma may result from trauma to a previous dermatofibroma and speculated that trauma or other mechanical irritation may explain the scar-like changes observed in dermatofibromas.The purpose of this study was to present our experience in treating a patient with chest keloidal dermatofibroma.
2.Case presentation
The patient was a 21-year-old male.He had been inoculated with the BCG vaccine on his left upper arm when he was young,which resulted in gradual swelling at the site of inoculation,which was initially overlooked and left untreated.In February 2010,the patient underwent a biopsy of the mass at the Peking Union Medical College Hospital (PUMCH),the results of which indicated a dermatofibroma.In February 2010,the patient underwent partial excision of the left upper arm mass with expander implantation at our hospital(Fig.1A).The patient was re-admitted to our hospital in June 2010 for left upper arm fibroma excision,dilator removal,and local flap transfer repair,and the postoperative pathological examination indicated dermatofibroma(Fig.1B).He underwent scar excision at our hospital on January 21,2011,because of growth of the wound scar,and the postoperative pathological examination reported keloidal dermatofibroma of the left upper arm(Fig.1C).Afterward,the patient did not undergo further standardized treatment for pathological scarring.

Fig. 1.Pathological images taken from the patient’s five operations.(A) The patient’s left upper arm pathology initially reported as dermatofibroma in February 2010.(B) A recurrent lesion on the left upper arm reported as dermatofibroma in June 2010.Subcutaneous epidermal thickening beneath the scar is observed,with a maximum thickness of 1.0 cm and a tough grayish-white woven texture.(C) The patient underwent another surgical procedure in January 2011 for incision of hypertrophic scar,and the postoperative pathology revealed keloidal dermatofibroma.(D)Chest skin pathology performed in August 2020 revealed spindle-shaped cytopathic lesions with a nodular distribution and a mild cell morphology.Immunohistochemical results showed Ki-67 (+1%),SMA (+),NF (-),CD68 (-) tumor.Considering the pathological findings,we diagnosed the lesion as dermatofibroma.(E) The patient’s pathological findings of the chest wall mass in January 2021 revealed a fibroblastic proliferative lesion with sparse cells,a mild morphology,multinodular growth with poorly defined borders in some areas,and keloid-like changes in some areas.Immunohistochemical results revealed β-catenin (weakly positive),CD68 (+),and CD34(-).Based on the patient’s clinical presentation and pathological findings,we made a diagnosis of keloidal dermatofibroma.
Subsequently,some incisional scars gradually grew and were accompanied by scattered keloid-like swellings on the chest,which affected his appearance and were associated with pain and itching.The patient presented to our hospital in July 2020 and was diagnosed with keloid-like swellings on the left upper arm and chest.The patient’s chest wall was covered with irregular round or oval swellings,the largest of which was approximately 3.0 cm ×6.0 cm,protruding from the skin surface,dark red,hard in texture,with clear borders,and not likely to rupture(Fig.2A,2B).Considering the patient had a history of incisional scar tissue-like hyperplasia after excision of the left upper arm mass and recurrence of dermatofibroma on histopathological examination,we adopted the principles of keloid treatment as the management strategy,including surgery combined with postoperative radiotherapy,hyperbaric oxygen therapy,and compression with elastomeric clothing.We selected a part of the chest wall mass for surgical treatment(Fig.2C)and used a surgical approach to remove the scar-like tissue from the core of the mass.After surgery,we performed local superficial radiation therapy in our radiotherapy department once a day for 3 days,with a single dose of 3-5 Gy for a total dose ranging from 15 to 20 Gy.Additionally,we administered oxygen therapy in the hyperbaric oxygen unit twice daily for 5 days.The patient was also treated with compression and immobilization with an elastic garment and provided symptomatic support treatment,such as anti-infectives.The postoperative pathological examination indicated dermatofibroma,and the immunohistochemical analysis revealed S-100 (-),Ki-67 (+1%),SOX-10 (-),CD68 (-),Vimentin (+),NF (-) tumor (Fig.1D).We further treated the patient with elastic band compression and application of topical silicone gel preparation on the left upper arm.On January 16,2021,the patient was admitted to our hospital for chest wall mass excision to treat the remaining chest wall mass.The incision at the last surgical site had healed well(Fig.2D).The treatment at this point was the same as the previous treatment(Fig.2E,2F).The patient’s postoperative pathological examination revealed keloidal dermatofibroma with irregular,thick,eosinophilic collagen fibers.Immunohistochemistry results demonstrated SOX-10(-),β-catenin(small amount positive),SMA (+),CD34 (-),CD68 (+),Ki-67 (+1%),and Bcl-2 (-)tumor (Fig.1E).The patient was discharged after adequate healing of the chest incision after surgery (Fig.2G,2H).After the operation,the patient was followed up once a month,and after 12 months of followup,the patient showed no signs of recurrence.The incision in the surgical site had healed well (Fig.2I).
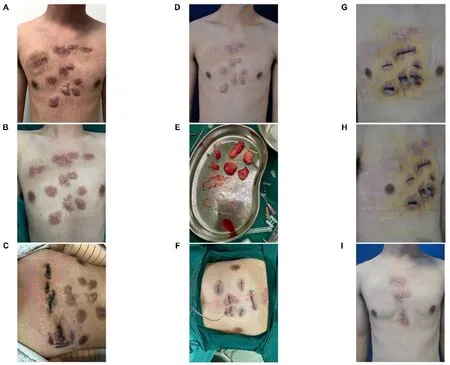
Fig. 2.Changes in the patient’s chest wall masses over time.(A,B) In July 2020,the patient was diagnosed with keloid-like masses on the left upper arm and chest and elected to undergo surgery.(C) In July 2020,the patient underwent a first partial excision of the anterior thoracic tumor and recovered well from surgery.(D)In January 2021,the patient underwent a second chest wall mass resection.Before surgery,the patient’s anterior chest wall was covered with numerous irregularly shaped,dark red lumps that were protruding from the skin and had a tough texture.The incision at the previous surgical site healed successfully with a satisfactory outcome.(E,F)We performed resection on the patient’s residual chest wall masses during an uneventful operation,and the masses were successfully removed.(G,H) The patient’s chest incision healed well postoperatively,with no redness,seeping,or suppuration and the patient showed satisfactory recovery.(I) The patient did not develop any new lesions during a 1-year follow-up,and the surgical site was healing well.
3.Discussion
Keloids often appear as thin,smooth,and shiny skin at the elevation of the lesion,surrounded by “crab feet” or “worm-like” edges.The cut surface is grayish-white,rugged,and elastic.On microscopic examination,the lesions are located in the dermis and consist of many coarse,dense collagen fibers crisscrossed or disorganized,with vitreous degeneration,deep eosinophilic red tissue staining,and stroma rich in mucopolysaccharides.However,fibroblasts are generally not dense and no fibrous tumor suggestive of a fibrous histiocytoma component is not observed.A clear clinical history of trauma or surgery is often present.5Dermatofibroma,which is the most common mesenchymal skin tumor,generally develops on the extremities but rarely presents on the chest or face.Tumors are generally small,often 0.3-1.0 cm in diameter,well-defined,and lack an envelope.Microscopic examination of the epidermis often reveals hyperkeratosis,irregular hyperplasia,and hyperpigmentation of the basal layer.In cases where superficial nodular fibrous tissue of the dermis proliferates,the proliferating cells are arranged in longitudinal bundles or swirls,and the cellular composition varies with the temporal phase of the tumor.The reaction phase of the tumor often has more cellular components,less fibrous tissue,and more delicate collagen fibers;whereas,the more advanced phase is characterized by fewer cellular components,predominantly mature fibroblasts,often with non-coarse collagen fiber bundles with vitreous degeneration.6The characteristics of these three skin diseases (keloid,dermatofibroma,and keloidal dermatofibroma)are summarized in Table 1.

Table 1 Characteristics of the three skin diseases (keloid,dermatofibroma,and keloidal dermatofibroma).
A previous study has shown that fibrous histiocytomas of the chest and face are more aggressive.5Keloidal dermatofibromas are rare and often present clinically as firm reddish-brown nodules in the form of erythematous,hard papules that appear scattered.4Keloidal dermatofibroma presents histologically as confined keloid-like areas consisting ofirregular eosinophilic collagen fibers on the tumor surface.A clear histological distinction between the regular proliferation of the overlying epithelium and pigmentation of the basal cell layer is observed in dermatofibroma and keloidal dermatofibroma.6Owing to the low incidence of keloidal dermatofibromas and their similarities with other diseases,combined with our own experience,we believe that keloidal dermatofibromas should be differentiated from keloid and other common types of dermatofibromas.Fibroblasts in keloids are usually not dense,lack a fibroid or fibrous histiocytoma component,and can be linked to a significant history of trauma,surgery,or infection.The common dermatofibromas often exhibit hyperkeratosis,irregular hyperplastic hypertrophy,and basal hyperpigmentation of the epidermis,without the presence of thick and glassy degenerative collagen fibrils as is seen in keloids.Aneurysmal dermatofibrosarcoma often occurs on the trunk and proximal extremities but rarely presents on the chest and face.It generally has a permeable margin that can extend subcutaneously.7Other single spindle cell tumors,such as peripheral nerve sheath and smooth muscle tumors,should also be differentially diagnosed from keloidal dermatofibroma.
The history of surgical treatment and pathological diagnosis of keloidal dermatofibroma in this patient are shown in Fig.3A.The patient underwent a total of five surgical treatments.He initially underwent a pathological biopsy at the age of 9 years at the PUMCH,the results of which indicated dermatofibroma of the upper arm,and he subsequently underwent surgical treatment in our hospital.We followed the treatment principles for benign skin tumors with buried dilators in the upper arm and performed radical excision of the mass with repair of the dilated skin transfer.He was later re-admitted to the hospital for postoperative scar growth,which was excised and sent for pathological examination.The patient was diagnosed with keloidal dermatofibroma of the left upper arm.Mechanical stimulation is an essential factor in the development of dermatofibromas.The lateral upper arm is an area of high tension;therefore,we believe that tension is a mechanical stimulus that contributes to the recurrence of dermatofibroma.
After the patient entered puberty,he developed generalized keloidlike swellings on the chest wall.Considering the previous history of multiple surgeries and the pathological findings,we chose to treat the tumor with the principles of keloid treatment.To reduce the tension of the incision and avoid the recurrence of swelling due to tension stimulation,we chose a surgical approach to remove the core tissue of the swelling while preserving the epidermis,combined with postoperative superficial radiotherapy and other adjuvant treatments (hyperbaric oxygen therapy,cortisol hormone,and elastic compression).Hyperbaric oxygen therapy has been shown to significantly affect the expression of inflammatory factors,such as interleukin-12p40,macrophage inflammatory protein-1β,platelet-derived growth factor-BB,and interleukin-1 receptor antagonist in patients with keloid,indicating that it can achieve a reduction in the inflammatory response.8Hyperbaric oxygen therapy also has a wide range of applications in the field of plastic surgery.Previous studies have shown that hyperbaric oxygen therapy is widely used in surgeries involving skin grafts and treatment of chronic non-healing wounds,9,10with particularly good results in the management of wound healing problems following flap transfer in plastic surgery.11Therefore,in this study,we administered hyperbaric oxygen therapy to the patient to promote wound recovery and achieved satisfactory results.We have followed up with the patient for one year,and he is recovering well with no recurrence.An overview of our treatment strategy for keloidal dermatofibromas is shown in Fig.3B.
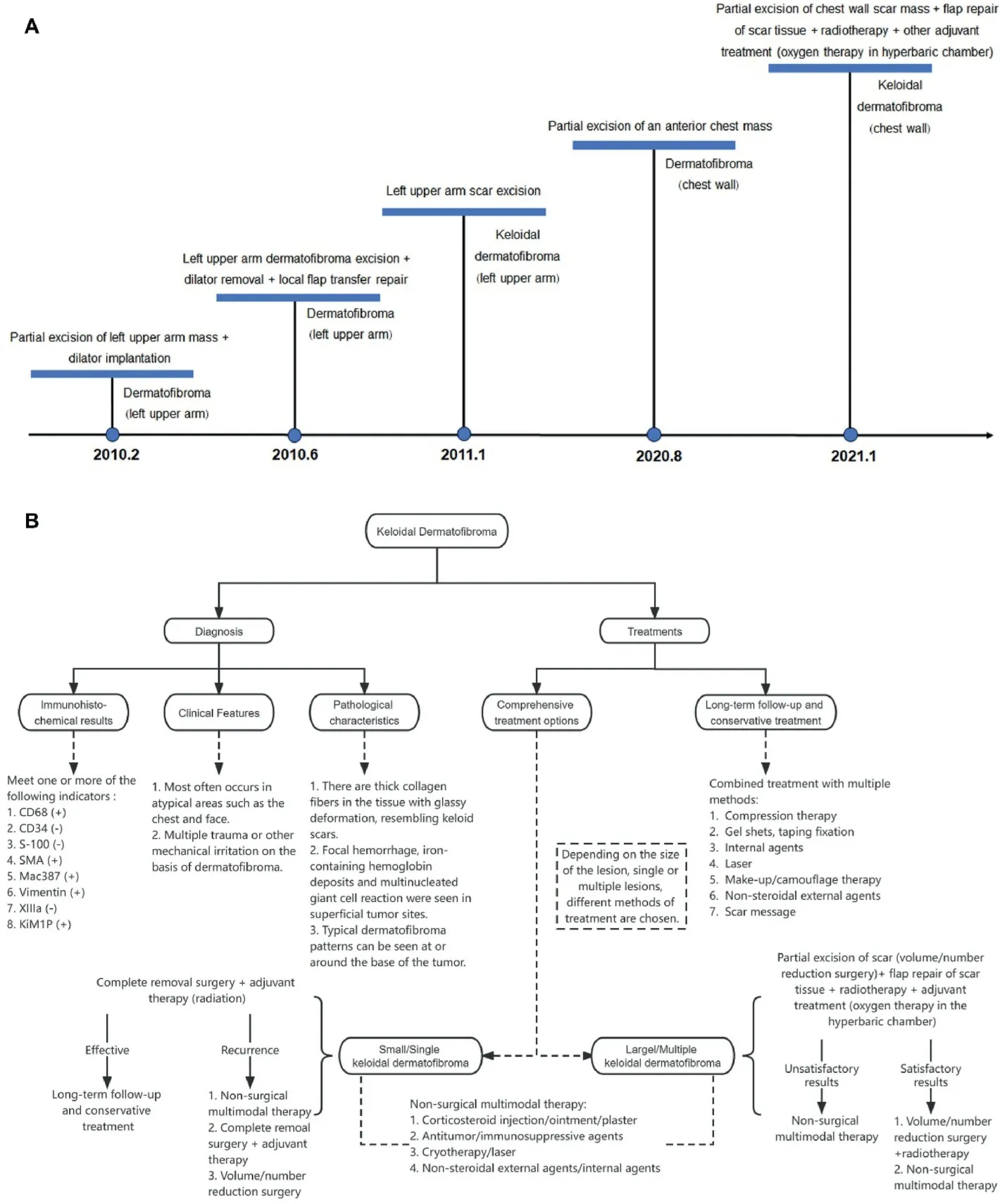
Fig. 3.(A) Timeline of inpatient treatment events.(B) Our treatment strategy in the management of keloidal dermatofibroma.
4.Conclusion
In view of the experience with this case,we believe that successful treatment of keloidal dermatofibroma (e.g.,extremities and chest wall)involving larger areas,high tension sites,and multiple localizations can be achieved using the principles of pathological scar management.
Ethics approval and consent to participate
The need for ethical approval and consent to participate was waived as this is a case report.
Consent for publication
The patient gave written informed consent to publish the data contained within this study.
Authors’ contributions
Xing J: Conceptualization,Methodology,Formal analysis,Writing-Original draft,Writing-Review and editing.Chen Y: Formal analysis.Zheng L: Formal analysis.Shao Y: Formal analysis.Xu Y: Conceptualization,Methodology,Writing-Original draft.Guo L: Conceptualization,Methodology,Formal analysis,Writing-Original draft,Writing-Review and editing.
Competing interests
The authors declare that they have no competing interests.
杂志排行

Chinese Journal of Plastic and Reconstructive Surgery的其它文章
- Rhinoplasty in China: A review of the most important events in its history of development
- A combined therapy for the repair of alar defects that consists of a modified spiral flap and postoperative nasal stent
- DeepPurpose-based drug discovery in chondrosarcoma
- Micropunch grafting for healing of refractory chronic venous leg ulcers
- Oral health-related quality of life between Chinese and American orthodontic patients: A two-center cross-sectional study
- A rare post-coronavirus disease 2019 complication of maxillary mucormycotic osteomyelitis in a Southeast Asian patient