The Dynamic Changes and Clinical Significance of Serum Neuroglobin Levels in Patients With Acute Ischemic Stroke
2022-11-22CHENGMinHANYaTingLINaGUOHuaiLian
CHENG Min,HAN Ya-Ting,LI Na,GUO Huai-Lian
(1)Department of Neurology,People’s Hospital,Peking University,Beijing 100044,China;2)Central Laboratory,People’s Hospital,Peking University,Beijing 100044,China;3)Key Laboratory for Neuroscience,Ministry of Education,National Health and Family Planning Commission,Peking University,Beijing 100191,China)
Abstract Objective Neuroglobin(Ngb)has been described as a neuroprotective agent in cerebral ischemia,which has a high affinity for oxygen and helps to prevent hypoxic-ischemic brain damage,and to affect the outcomes after acute ischemic stroke(AIS).In this study,the changes of serum Ngb level after AIS were investigated and the relationship of Ngb and stroke severity and prognosis were evaluated.Methods We prospectively measured the serum levels of Ngb in AIS patients at different time points(within 72 h and on day 14(D14)after onset of cerebral infarction)and in control subjects.Serum Ngb levels were compared between the AIS patients and controls.The serum Ngb levels in the AIS patients with and without diabetes mellitus(DM)were also compared.Correlations between Ngb level and infarct size and that between Ngb level and National Institutes of Health Stroke Scale(NIHSS)score of the patients were analyzed.Receiver operating characteristic(ROC)curve was used to appraise their value in predicting the outcome at day 90 after AIS,which was evaluated using the modified Rankin Scale(mRS).Results Serum Ngb levels in patients were 105.7(88.3,123.1)μg/L within 72 h and 72.8(58.7,86.9)μg/L on D14 after cerebral infarction,respectively.Serum Ngb level in control group was 58.2(35.0,81.6)μg/L.Serum Ngb level within 72 h after AIS increased significantly compared with that in the control group(P<0.05).Serum Ngb levels of AIS patients with or without DM showed no significant difference within 72 h and on D14 after AIS(P>0.05).Serum Ngb level within 72 h was significantly correlated with NIHSS score(Spearman correlation coefficient=0.232,P=0.038).Serum Ngb levels had no significant difference in patients with large infarction than in those with small or moderate infarction at each time point(P>0.05).ROC curve analysis suggested that the serum Ngb level had a significantly good predictive power for outcomes.Conclusion The results indicated that serum Ngb level increased within 72 h after AIS,which is independent of comorbidity with diabetes.Serum Ngb level within 72 h was significantly correlated with NIHSS score,and Ngb might have the potential to be a predictor of stroke severity and prognosis.
Key words acute ischemic stroke,cerebral infarction,neuroglobin,infarction volume DOI:10.16476/j.pibb.2022.0420
Acute ischemic stroke(AIS)is a sudden neurologic deficit that results from impairment of blood supply to the brain,and is a major cause of death and disability in modern life.In recent years,the measurement of blood biomarkers has drawn more interest,but a precise early prognostic biomarker of AIS is still lacking.Therefore,more reliable biomarkers are needed to guide the clinical diagnosis of AIS.Neuroglobin(Ngb)is a member of the tissue globin family with a high affinity for oxygen,and is highly and specifically expressed in brain neurons[1].Ngb is an oxygen-binding heme protein found in the brains of vertebrates,including humans.The involvement of Ngb in protection against ischemia has been studiedin vitroandin vivo.Knockdown of Ngb expression exacerbated hypoxia and ischemic neuronal damage in rodents[1-2].Some evidences have clearly demonstrated that Ngb has neuroprotective effects on the cultured neurons and animal brains against hypoxic and ischemic injuries[2-5].In Parkinson’s disease,Ngb upregulation protected neurons from H2O2‑induced neurotoxicity[4].Ngb has been described as a neuroprotective agent in cerebral infarction,and it has a high affinity for oxygen and helps prevent hypoxic-ischemic brain damage,therefore it has the potential to affect outcomes after AIS.Human studies have suggested a relationship between Ngb polymorphisms and risk for cerebrovascular disease.Ischemic stroke increases expression of the neuroprotective protein neuroglobin,suggesting Ngb may represent a novel target for stroke therapy in experiment[6-7].But the relationship between stroke infarct volume and Ngb level is still not fully understood.In addition,Ngb level also increased in patients with diabetic proliferative retinopathy[8-9],and a lot of AIS patients has vascular risk factors such as diabetes.However,there was no research exploring the difference of Ngb levels between AIS patients with and without diabetes.To investigate these questions,we examined the dynamic changes of serum Ngb after AIS and analyzed the relationship between Ngb levels and clinical outcomes of AIS.
1 Subjects and methods
1.1 Subjects
Between October 2017 and October 2020,a prospective cohort of patients with AIS was collected in the Department of Neurology at Peking University People’s Hospital.Patients who suffered from acute cerebral infarction within 72 h for the first time were included.All patients were confirmed AIS through serial neurological examinations and by evaluating with cranial computed tomographic(CT)or magnetic resonance imaging(MRI)scan.To avoid interfering factors,patients who suffered lacunar infarction,cerebral hemorrhagic infarction,epilepsy,history of neurological diseases,myocardial infarction,renal and hepatic abnormalities,hematological system disorders,autoimmune disease,tumor,severe systemic infection,surgery or trauma within 3 months,or taking estrogen drugs were excluded.
Accordingly,demographic data of subjects,including age,gender,and clinical data,such as features and duration of symptoms,and location of infarcts were documented.Control group consisted of people who came to our hospital for regular physical checkups during the same period.All controls finished medical examinations and had negative imaging studies and no neurological disease,such as recent infection,stroke,tumors,vascular anomalies,abnormalities of blood system,transient ischemic attack,head trauma,or serious illness,which were matched with patient group by sex,age,hypertension,diabetes mellitus(DM),hyperlipidemia,and cardiac disease.This study had the approval from the hospital ethics committee and all subjects gave informed consent for participating in the study.
1.2 Measurement of serum Ngb
Blood samples from patients with AIS were obtained from the antecubital vein within 72 h and on day 14(D14)after stroke,after an overnight fast.Blood samples were also obtained in the controls.Samples were centrifuged(2 000 r/min,10 min)to segregate serum,and was frozen at-80°C until the later analysis.Ngb in serum was measured by enzymelinked immunosorbent assay(ELISA)with commercially available kits(Novus Biologicals,USA),according to the manufacturer’s instructions.
1.3 Clinical assessments
All patients were evaluated with head CT or MRI and the National Institutes of Health Stroke Scale(NIHSS)score as indicator of neurological deficit.All the imaging studies were reviewed by 2 staffs of the radiology department,who were blinded to clinical diagnosis.Based on the head CT and/or MRI,the cerebral infarct volume was measured and calculated using the formula(A×B×C)/2(where A=maximal longitudinal diameter,B=maximal transverse diameter perpendicular to A and C=number of 10-mm slices containing infarct)[10].Patients were classified as having a large infarction(LI,volume>10.0 cm3),a small infarction(SI,volume<5.0 cm3)or a moderate infarction(MI,volume between 5.0 and 10.0 cm3).Outcome at day 90 after AIS was evaluated using the modified Rankin Scale(mRS):0=no symptoms;1=no significant disability;2=slight disability;3=moderate disability;4=moderately severe disability;5=severe disability;6=dead[11].For statistical comparison,favorable outcome was defined as a mRS score of 0-2,and unfavorable outcome was defined as a mRS score of 3-6.Surviving patients participated in followup interviews by telephone.
1.4 Statistical analysis
The statistical package SPSS 27.0 was used for all analyses.All values were expressed as mean±standard or medium(P25,P75).K-S test was used for Ngb levels comparisons between AIS patients at 2 selected time points and controls,and the same statistical analysis was performed to identify differences in Ngb levels and differences in infarction size.Differences in Ngb levels between the SI or MI and LI subgroups were assessed with K-S test.Relations between variables were assessed by Spearman correlation coefficient.All analyses were two tailed.Values were considered significant atP<0.05.A receiver operator characteristic(ROC)curve and the area under the ROC curve(AUC)were used to assess the accuracy of predictions of outcome from the serum Ngb levels.
2 Results
2.1 Characteristics of AIS patients and controls
Of the 40 patients(22 men and 18 women,21 of them with DM)included in this study,their age ranged from 40 to 84 years(average age 69.7 years).Locations of infarct,as evidenced by radiologic and neurologic symptoms or signs,included the Internal carotid artery infarction(35 cases)and vertebrobasilar infarction(5 cases).14 patients had LI,and 26 patients had SI or MI.The control group contained 10 men and 12 women.Their age averaged 59.3 years and ranged from 49 to 79 years.Clinical characteristics(sex ratio,age,smoking,complications with hypertension or hyperlipidemia)of the two groups are summarized in Table 1.Comparison of clinical characteristics between the two groups showed no significant difference(P>0.05).

Table 1 Characteristics of patients with AIS and controls
2.2 Serial changes in serum Ngb levels in AIS patients
The mean serum Ngb level of the control group was 58.2(35.0,81.6)μg/L.Ngb levels in serum tended to increase after cerebral infarction.Ngb level increased significantly within 72 h[105.7(88.3,123.1)μg/L)]compared with control(P=0.004),and it decreased significantly on D14[72.8(58.7,86.9)μg/L]compared with that within 72 h(P=0.029).The Ngb levels had no significant difference between control and D14 group(P=0.149)(Table 2).No significant differences were found in the subgroups with or without DM(Table 3).
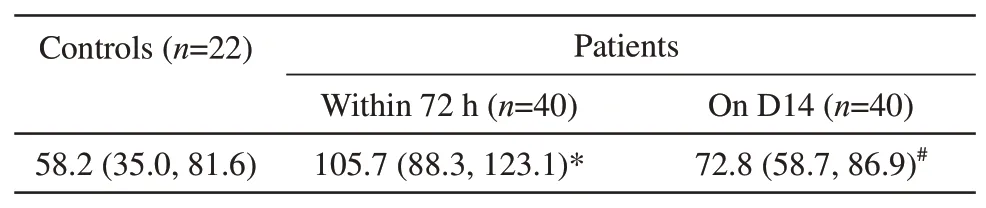
Table 2 Serum Ngb levels in AIS patients at different time points and in control group μg/L

Table 3 Serum Ngb levels in AIS patients with or without DM μg/L
2.3 Serum Ngb levels and infarct size and NIHSS score
Based upon the calculated infarct volume,the patients were divided into SI or MI(n=26)and LI(n=14)groups.The serial changes of serum Ngb levels in these two groups were shown in the Table 4.The Ngb levels in patients have no significant difference with LI group and SI or MI groups.Significant correlations were found between serum Ngb level within 72 h and NIHSS score on admission(Spearman correlation coefficient=0.232,P=0.038).

Table 4 Serum Ngb levels in subgroups of patients with LI and SI or MI at different time points μg/L
2.4 Serum Ngb levels and outcome
Outcome at day 90 after AIS was favorable for25 patients and unfavorable for 15 patients.The serum Ngb level within 72 h was significantly higher in patients with an unfavorable outcome than that in patients with a favorable outcome.Using the ROC,we found that the serum Ngb level within 72 h had a significantly good predictive power for prognosis(Figure 1).
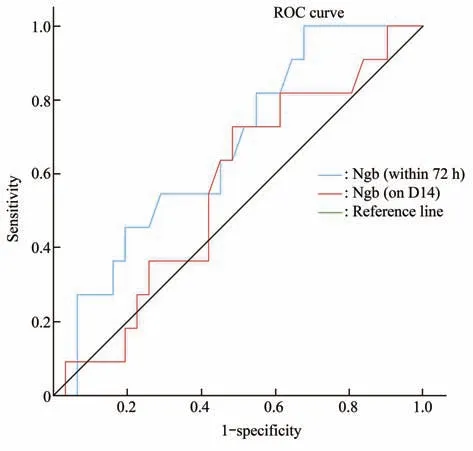
Fig.1 ROC curve to predict the possibility of outcome at day 90 after acute ischemic stroke by the serum levels of Ngb
3 Discussion
Currently,a number of biomarkers have been used to indicate brain injury,such as S100B,glial fibrillary acidic protein(GFAP),and neuron-specific enolase(NSE)[12].Although biomarkers in the cerebrospinal fluid(CSF)are more sensitive and specific to indicate brain damage than in blood,the CSF samples are difficult to obtain.In our study,we detected the dynamic changes of the serum levels of Ngb,which can be used as indicators for neuronal damage.
Previous studies have reported that Ngb was upregulated and protective in ischemic strokein vivo[13].Sunet al.[14]found that Ngb expression is increased after hypoxia and ischemia in cultured cortical neurons in rats,and that post-ischemic neuronal survival and animal functional neurological outcome are both improved by Ngb overexpression but worsened by inhibiting Ngb expression.Shanget al.[13]reported that the Ngb expression was significantly upregulated in the cerebral cortex after ischemia-reperfusion,and the level of Ngb in serum was significantly increased at 8 h and reached a peak at 48 h following ischemia.Zhaoet al.[15]has shown that the level of Ngb in serum increased at 1-6 h after the onset of acute cerebral infarction patients,peaked at 24 h,descended to normal at 72 h.Xueet al.[12]reported Ngb level increased in serum after AIS and peaked at 72 h,and it was suggested as a predictor of poor prognosis.Jinet al.[6]reported that Ngb was detected in several brain areas,and its expression was increased in the cortical peri-infarct region after stroke,suggesting Ngb may represent a novel target for stroke therapy.
Although the level of Ngb in serum after ischemia in rats and in AIS patients has been reported previously,the results of previous studies on the changes of serum Ngb levels in patients with AIS were inconsistent,most of which were changes in the early onset,and did not analyze the results with or without DM.In this study,we analyzed the changes in serum Ngb levels following AIS.Additionally,we analyzed the Ngb levels with or without DM.We present an analysis of the relationship between serum Ngb levels and infarction volume and outcomes at day 90 in patients with AIS.Our results demonstrated that the level of Ngb was increased after AIS in the serum,and upregulation of Ngb significantly correlated to the NIHSS score,and Ngb levels can be used as a predictor for prognosis of AIS.However,our study only collected the serum in 2 time points.Without continuous collecting samples,we haven’t found the peak level of serum Ngb in patients with AIS.
Several findings showed that Ngb reduced tissue infarction after stroke,tissue protection by overexpressing Ngb could be sustained for up to 2 weeks,and the volume of cerebral infarcts in Ngb overexpressing transgenic mice was reduced by approximately 30% at 1 day and 14 days after cerebral ischemia[16-17].In this study,we detected correlation between infarct volume and Ngb level,which is inconsistent with the study results in many experimental ischemic stroke models and in AIS patients.But there were also opposite results,Zindyet al.[18]detected that Ngb-deficiency resulted in reduced tissue infarction,suggesting that,at least at endogenous expression levels,neuroglobin in itself is non-protective against ischemic injury.As a whole,apart from few contestable discrepancies,Ngb overexpression is generally considered beneficial against experimental ischemia.The inconsistent maybe related with the Ngb was detected in the cortical periinfarct region after stroke[6].Accordingly,Ngb might serve a similar neuroprotective role in humans.Although direct evidence is lacking,one study has shown that Ngb polymorphism had protective effects on large-artery atherosclerosis and small-vessel occlusion stroke in the Southern Chinese Han population[7].In addition,in our study,a positive correlation was detected between NIHSS and Ngb levels in serum of AIS patients,which is consistent with those observed in ischemic stroke patients[12].
There are some limitations in our study.Firstly,it is unclear whether the Ngb level in serum reflects the Ngb level in central nervous system.Secondly,the number of patients is limited.If we increase sample size,accuracy and sensitivity of the study would be better.
4 Conclusion
Our current observations indicated that the serum Ngb level increased within 72 h,which is independent of comorbidity with diabetes.Ngb might play a role in cerebral infarction,and it might be involved as a predictor of stroke severity and prognosis.
