Comparison of short-term efficacy between totally laparoscopic gastrectomy and laparoscopic assisted gastrectomy for elderly patients with gastric cancer
2022-10-11RuiYangZhaoHangHangLiKeChengZhangHaoCuiHuanDengJingWangGaoBoWei
Rui-Yang Zhao, Hang-Hang Li, Ke-Cheng Zhang, Hao Cui, Huan Deng, Jing-Wang Gao, Bo Wei
Rui-Yang Zhao, Hang-Hang Li, Ke-Cheng Zhang, Huan Deng, Jing-Wang Gao, Bo Wei, Department of General Surgery, First Medical Center, Chinese PLA General Ηospital, Beijing 100853, China
Rui-Yang Zhao, Hang-Hang Li, Huan Deng, Jing-Wang Gao, Bo Wei, Medical School of Chinese PLA, Chinese PLA General Ηospital, Beijing 100853, China
Hao Cui, School of Medicine, Nankai University, Tianjin 300071, China
Abstract BACKGROUND Totally laparoscopic gastrectomy (TLG) entails both gastrectomy and gastrointestinal reconstruction under laparoscopy. Compared with laparoscopic assisted gastrectomy (LAG), TLG has been demonstrated in many studies to require a smaller surgical incision, result in a faster postoperative recovery and less pain and have comparable long-term efficacy, which has been a research hotspot in recent years. Whether TLG is equally safe and feasible for elderly patients remains unclear.AIM To compare the short-term efficacy of and quality of life (QOL) associated with TLG and LAG in elderly gastric cancer (GC) patients.METHODS The clinicopathological data of 462 elderly patients aged ≥ 70 years who underwent LAG or TLG (including distal gastrectomy and total gastrectomy) between January 2017 and January 2022 at the Department of General Surgery, First Medical Center, Chinese PLA General Hospital were retrospectively collected. A total of 232 patients were in the LAG group, and 230 patients were in the TLG group. Basic patient information, clinicopathological characteristics, operation information and QOL data were collected to compare efficacy.RESULTS Compared with those in the LAG group, intraoperative blood loss in the TLG group was significantly lower (P < 0.001), and the time to first flatus and postoperative hospitalization time were significantly shorter (both P < 0.001). The overall incidence of postoperative complications in the TLG group was significantly lower than that in the LAG group (P = 0.01). Binary logistic regression results indicated that LAG and an operation time > 220 min were independent risk factors for postoperative complications in elderly patients with GC (P < 0.05). In terms of QOL, no statistically significant differences in various preoperative indicators were found between the LAG group and the LTG group (P > 0.05). Compared with the laparoscopic-assisted total gastrectomy group, patients who received totally laparoscopic total gastrectomy had lower nausea and vomiting scores and higher satisfaction with their body image (P < 0.05). Patients who underwent laparoscopic-assisted distal gastrectomy were more satisfied with their body image than patients in the totally laparoscopic distal gastrectomy group (P < 0.05).CONCLUSION TLG is safe and feasible for elderly patients with GC and has outstanding advantages such as reducing intracorporeal blood loss, promoting postoperative recovery and improving QOL.
Key Words: Totally laparoscopic gastrectomy; Laparoscopic assisted gastrectomy; Gastric cancer; Elderly patients; Efficacy comparison; Quality of life
lNTRODUCTlON
China has a high incidence of gastric cancer (GC), and GC incidence and mortality both rank second among malignant tumors[1], resulting in serious health and medical burdens for Chinese people. Despite slight decreases in GC incidence and mortality with the improvements in diagnosis and treatment, they have gradually increased for elderly patients with GC[2]. Therefore, reasonable treatment regimens still need to be developed for elderly patients with GC.
In 1994, Kitanoet al[3] carried out the first laparoscopic gastrectomy (LG)[3]. In recent years, an increasing number of multicenter clinical studies have confirmed that LG has comparable surgical safety and long-term prognosis compared to those who received open gastrectomy[4-6]. Therefore, minimally invasive surgery,i.e., laparoscopy, has become an alternative surgical approach for the treatment of GC. Gastrointestinal reconstruction is a key step in LG. With continuous improvements in surgeons’ skills and improvements in intracorporeal staplers, totally laparoscopic gastrectomy (TLG) with complete intracorporeal anastomosis has become a research hotspot. Previous studies have shown that compared with laparoscopic assisted gastrectomy (LAG) or open gastrectomy, TLG requires a smaller incision, induces less postoperative pain and improves postoperative quality of life (QOL)[7,8]. These advantages are also shown in patients who have received the neoadjuvant chemotherapy[9].
Because of the advantages of TLG and significant advancement in intracorporeal operation, the number of studies concerning TLG is increasing. A multicenter prospective study focusing on the effects of totally laparoscopic distal gastrectomy (TLDG) or laparoscopic-assisted distal gastrectomy (LADG) on postoperative QOL is being performed in South Korea[10]. However, it is still unclear whether TLG is identically safe and feasible for elderly patients. Therefore, we conducted this study to provide a proof for the application of TLG for elderly patients by comparing the short-term efficacy and QOL between elderly GC patients who received TLG or LAG.
MATERlALS AND METHODS
Patients
The inclusion criteria were as follows: (1) Age ≥ 70 years; (2) Gastric adenocarcinoma confirmed by preoperative gastroscopic pathology, endoscopic ultrasonography, abdominal computed tomography (CT) or positron emission tomography-CT; and (3) Postoperative pathological staging of Ia-IIIc. The exclusion criteria were as follows: (1) Intraoperative conversion to open surgery for any reason; (2) American Society of Anesthesiologists (ASA) classification > grade III; (3) Gastric stump cancer treated by gastric surgery; (4) Previous proximal gastrectomy; and (5) Absence of clinical and pathological data.
Based on the above criteria, clinical and pathological data were retrospectively collected from 462 elderly GC patients who underwent TLG or LAG at the Department of General Surgery, First Medical Center, Chinese PLA General Hospital between January 2017 and January 2022, including 230 patients in the TLG group and 232 patients in the LAG group. The clinicopathological characteristics of the patients are provided in Table 1. This study meets the requirements of the Declaration of Helsinki and has been approved by the Research Ethics Committee of Chinese PLA General Hospital (Approval Number: S2021-605-01).
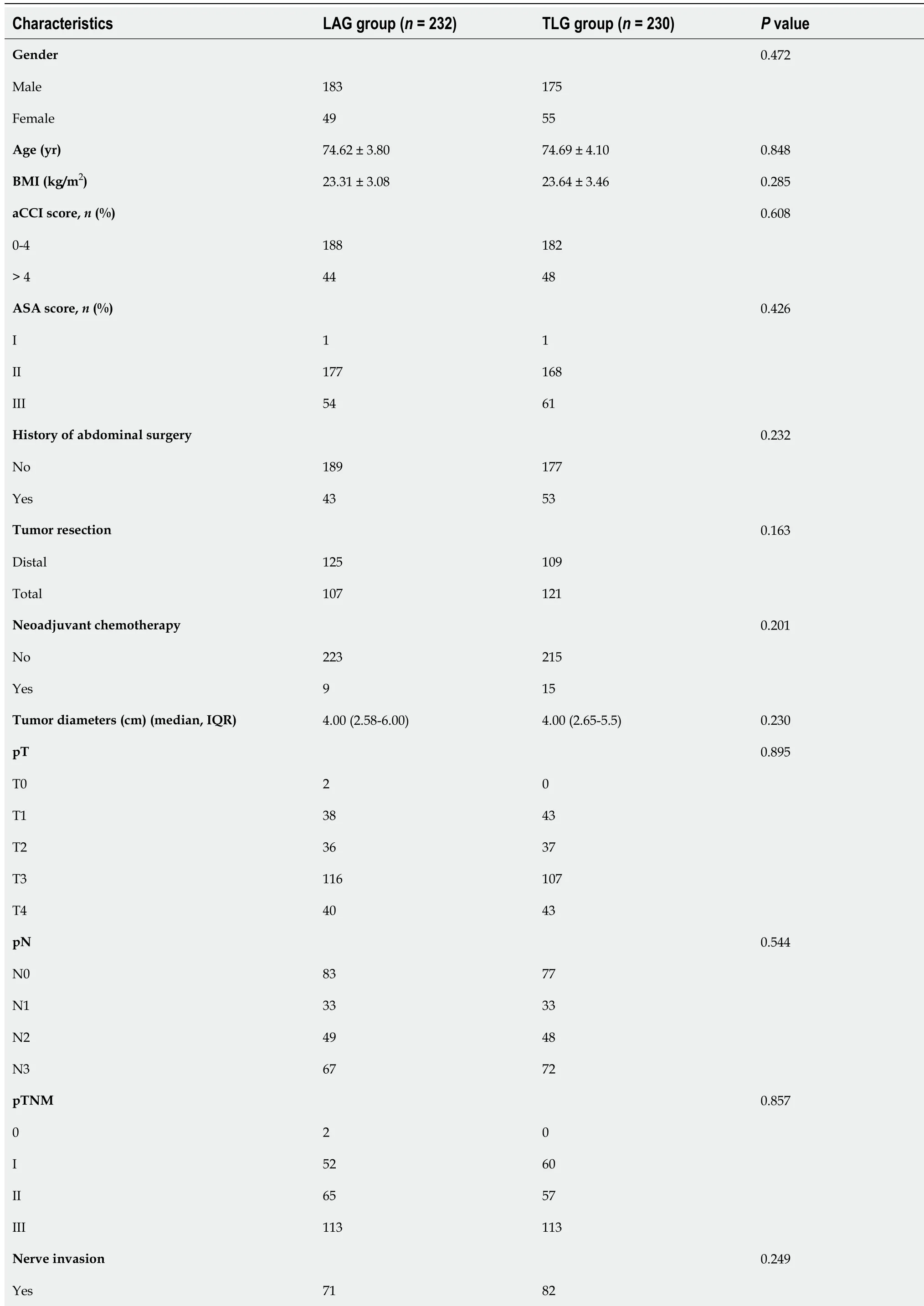
Table 1 Clinical and pathological characteristics of laparoscopic assisted gastrectomy and totally laparoscopic gastrectomy group for elderly patients (mean ± SD)
LAG: Laparoscopic assisted gastrectomy; TLG: Totally laparoscopic gastrectomy; aCCI: Age-adjusted Charlson Comorbidity Index; BMI: Body mass index; ASA: American Society of Anesthesiologists; SD: Standard deviation; IQR: Interquartile range.
Surgical approach
The surgical procedure was performed in accordance with theChinese Guidelines for laparoscopic gastrectomy for gastric cancer(2016 edition). The scope of surgical resection and lymph node dissection was based on the standard criteria established by theJapanese gastric cancer treatment guidelines 2018(5thedition)[11]. D2 Lymph node dissection was performed for all patients who underwent distal or total gastrectomy. The intracorporeal gastrointestinal reconstruction procedure in the TLG group was performed in accordance with theChinese Expert consensus and surgical operation guidelines for gastrointestinal reconstruction in totally laparoscopic gastrectomy(2018 edition). After completing intracorporeal reconstruction, a small upper abdominal median incision (length of incision ≤ 7 cm) was made for specimen removal only. After lymph node dissection in the LAG group, the upper abdominal median incision (incision length ≤ 10 cm) was used to remove the specimens, and the extracorporeal gastrointestinal reconstruction was performed. A circular anastomosis was performed at the esophagojejunal anastomotic site in laparoscopic assisted total gastrectomy (LATG). In totally laparoscopic total gastrectomy (TLTG), a linear anastomosis, including overlap or π anastomosis, was performed at the esophagojejunal anastomotic site. The methods for gastrointestinal reconstruction were selected based on the surgeon’s preferences and executed in accordance with standardized procedures.
Definition and classification of postoperative complications
The incidence and severity of complications within 30 d after surgery were assessed[12] using the Clavien-Dindo classification. The evaluation criteria mainly included the following: (1) Grade I: Any deviation from the normal postoperative recovery process but without the need for drugs, surgical intervention, endoscopy or interventional therapy; (2) Grade II: A need for drug therapy including blood transfusion, or total parenteral nutrition (except antiemetic, antipyretic, analgesic, diuretic, rehydration and other symptomatic drug therapy); (3) Grade III: Surgical intervention, endoscopy or interventional treatment needed (Grade IIIa, does not require general anesthesia; Grade IIIb, requires general anesthesia); (4) Grade IV: Life-threatening condition with treatment needed in the intensive care unit (Grade IVa, single organ failure; Grade IVb, multiple organ failure); and (5) Grade V: Death. In this study, complications within 30 d after surgery were defined as Clavien-Dindo grade ≥ II, and severe complications within 30 d after surgery were defined as Clavien-Dindo grade ≥ IIIa because of the limitation associated with a retrospective study design.
QOL questionnaire and scoring method
In this study, the Chinese versions of the European Organization for Research and Treatment of Cancer Quality of Life Core Questionnaire (EORTC QLQ-C30)[13] and QLQ-ST022[14] were used to assess the QOL of patients before and 3 mo after surgery. The EORTC QLQ-C3O is a core scale for all cancer patients, with a total of 30 items. Among them, items 29 and 30 are scored using 7 grade options, which are assigned 1 to 7 points based on the answer options. Other items are scored using 4 grade options,i.e., not at all, a little, quite a bit, and very much, and are assigned 1 to 4 points when scoring. The QLQ-C30 questionnaire is divided into 15 domains, including 5 functional domains (physical, role, cognitive, emotional, and social functioning), 3 symptom domains (fatigue, pain and nausea and vomiting), 1 overall QOL domain and 6 single items (each as a domain). The QLQ-STO22 includes 22 items related to the QOL of GC patients and consists of 9 scales, including dysphagia, pain, reflux, eating restriction, anxiety, dry mouth, taste, body shape and hair loss.
Statistical analysis
SPSS 26.0 statistical software was used for analysis. Normally distributed measurement data are expressed as the mean ± SD. Categorical data are expressed asn(%). Data with a skewed distribution are expressed as the median (interquartile range). Binary logistic regression was used to analyze the relationships between postoperative complications and clinical and pathological factors. Factors withP< 0.20 in the univariate analysis were included in the multivariate analysis.P< 0.05 was considered statistically significant.
RESULTS
Clinical and pathological characteristics
Among the 462 patients, 183 males and 49 females were included in the TLG group, with an average age of 74.69 ± 4.10 years, and 175 males and 55 females were included in the LAG group, with an average age of 74.62 ± 3.80 years. No significant differences in clinical characteristics, such as age, sex, body mass index, age-adjusted Charlson comorbidity index score, ASA score, a history of abdominal surgery and the range of surgical resection, were identified between 2 groups (P> 0.05). In terms of pathological characteristics, no significant differences in pathologic T stage, pathologic N stage, pTNM stage, tumor size, nerve invasion, vascular invasion or tumor differentiation were found between the 2 groups, suggesting that the baseline characteristics of the 2 groups were comparable (Table 1).
In the subgroup analysis, we compared the baseline characteristics between the TLTG group and LATG groups and between the TLDG and LADG groups. The results suggested that the tumor diameter in the TLDG group was smaller than that in the LADG group (P= 0.035). No significant differences were noted between other clinicopathological indicators (P> 0.05, Supplementary Table 1).
Perioperative outcomes and postoperative recovery
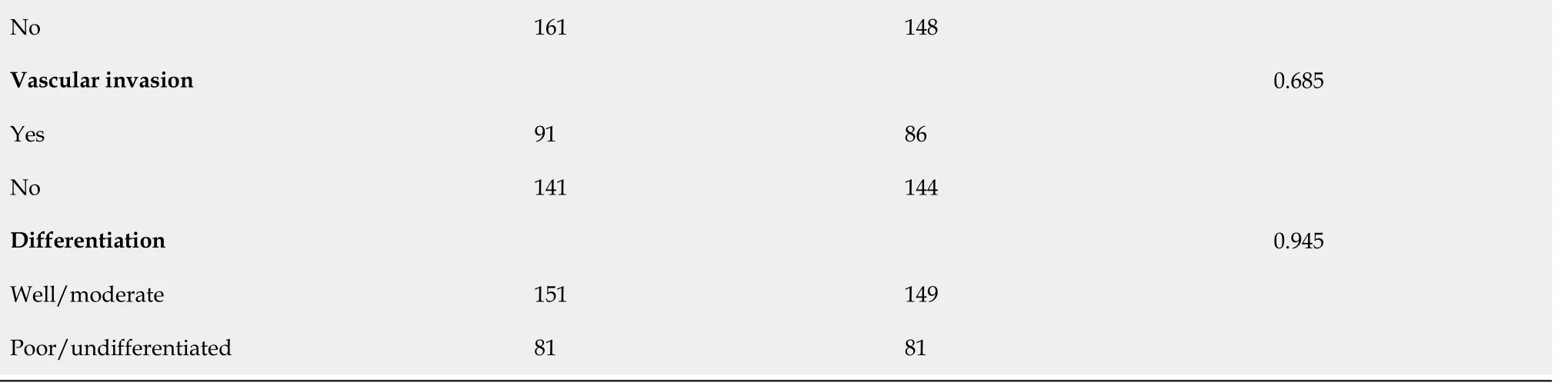
The perioperative outcomes are presented in Table 2. Compared with those in the LAG group, intraoperative blood loss in the LTG group was significantly lower [100 (50-100) mLvs100 (50-200) mL] (P< 0.001), the time to first flatus was significantly shorter [(3.79 ± 1.15) dvs(4.43 ± 1.20) d] (P< 0.001), and the postoperative hospitalization time was shorter [7.75 (6.0-9.0) dvs8.0 (7.0-10.0) d] (P< 0.001). No significant differences in the operation time, anastomosis methods, numbers of retrieved lymph nodes or R0 resection rates were observed between the 2 groups (P> 0.05). In terms of postoperative complications, the overall incidence of postoperative complications in the TLG group was significantly lower than that in the LAG group (16.5%vs26.3%,P= 0.01). Additionally, no significant differences in the incidence of anastomotic-related complications (2.6%vs3.4%,P= 0.599) or the incidence of severe complications (3.9%vs4.3%,P= 0.830) were found between the TLG and LAG groups.
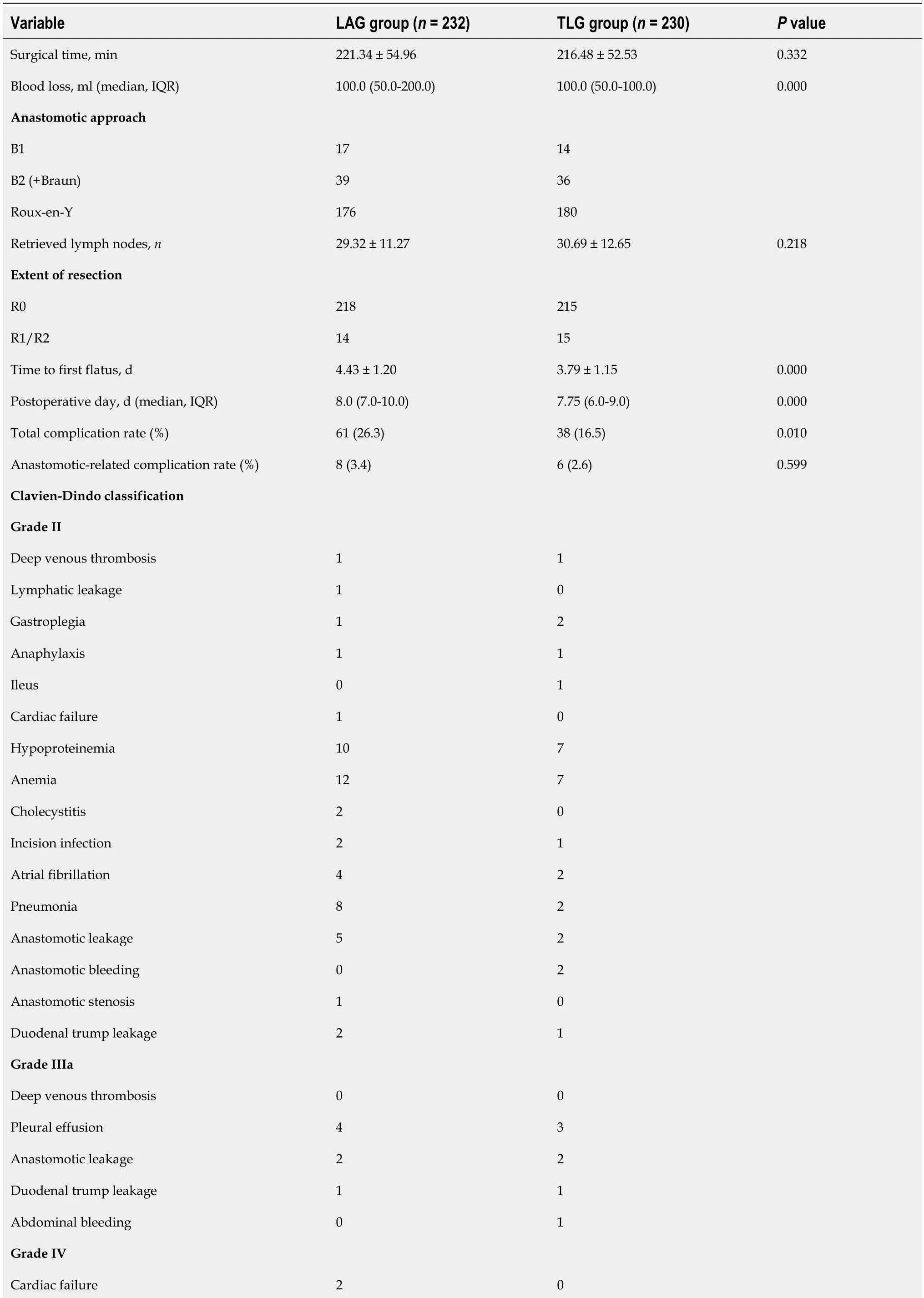
Table 2 Perioperative outcomes between laparoscopic assisted gastrectomy and totally laparoscopic gastrectomy group for elderly patients (mean ± SD)

Statistically significant P values are in bold (P < 0.05). LAG: Laparoscopic assisted gastrectomy; TLG: Totally laparoscopic gastrectomy; SD: Standard deviation; IQR: Interquartile range.
The results of the subgroup analysis indicated that the operation time in the TLDG group was significantly shorter than that in the LADG group [(201.82 ± 45.35) minvs(217.88 ± 49.08) min,P= 0.01]. In terms of intraoperative blood loss, the time to first flatus, and postoperative hospitalization time, TLG showed significant advantages over LAG in either distal or total gastrectomy (Supplementary Table 2).
We further explored risk factors for postoperative complications (Table 3). Univariate analysis indicated that TLG and LAG were associated with postoperative complications (P= 0.011). We included factors withP< 0.02 in the multivariate analysis. The results indicated that LAG and an operation time > 220 min were independent risk factors for postoperative complications in elderly patients with GC (P< 0.05). For the comparisons between LDG and LTG, the results suggested that a long tumor diameter > 3 cm and an operation time > 220 min were independent risk factors for postoperative complications in the LDG group (P< 0.05). No independent risk factors for postoperative complications were observed in the LTG group, as shown in Supplementary Table 3.
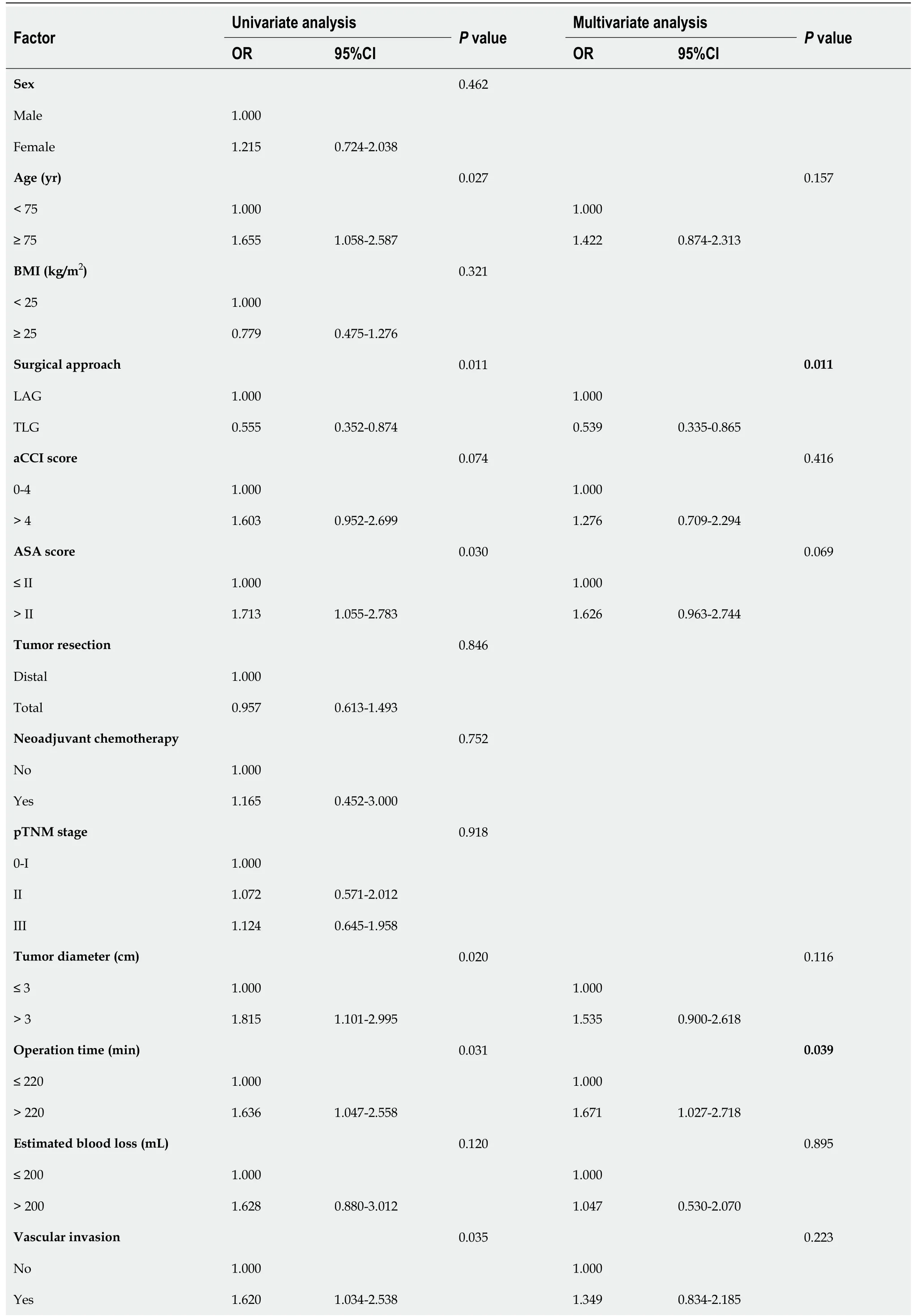
Table 3 Uni- and multivariate analysis of postoperative complications for elderly patients
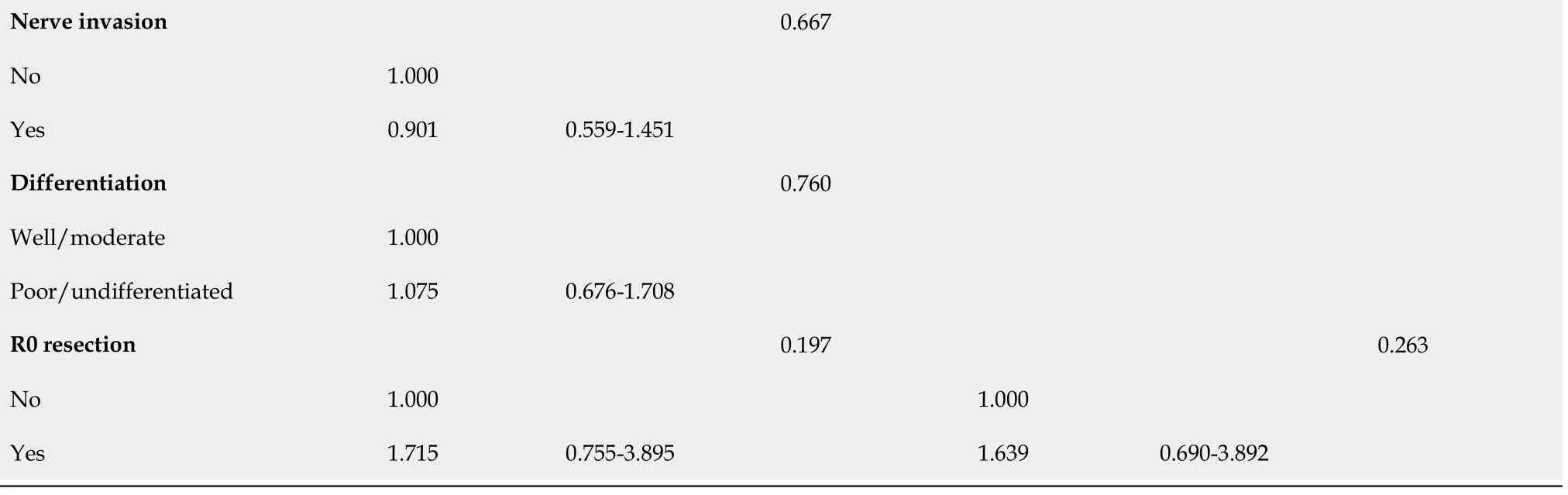
Statistically significant P values are in bold (P < 0.05). LAG: Laparoscopic assisted gastrectomy; TLG: Totally laparoscopic gastrectomy; aCCI: Age-adjusted Charlson Comorbidity Index; BMI: Body mass index; ASA: American Society of Anesthesiologists; OR: Odd ratio.
For the subgroup analysis based on surgical resection range, patients who underwent TLG had lower risks of postoperative complications in both the LTG (odds ratio (OR) = 0.612; 95% confidence interval (CI): 0.313-1.198) and LDG (OR = 0.619; 95%CI: 0.313-1.224) groups compared with patients who received LAG, although the differences were not statistically significant.
QOL using the EORTC QLQ-C30 and STO-22
We collected preoperative and 3-mo postoperative QOL questionnaire data from the 462 patients and compared changes in QOL between the LAG and LTG groups (Table 4). The results showed no statistically significant differences in symptom indicators, overall health indicators or functional indicators between the LAG and LTG groups before surgery (P> 0.05). Postoperative patients in the TLG group reported greater relief from nausea, vomiting and constipation than those in the LAG group. Patients in the TLG group were more satisfied with their body image.
Furthermore, the subgroup analysis (Supplementary Tables 4 and 5) showed that patients in the TLTG group had lower scores in the nausea and vomiting domains than those in the LATG group [0 (0-0)vs0 (0-16.6),P= 0.016]. Patients who underwent TLTG were more satisfied with their body image than those who received LAGT [0 (0-0)vs0 (0-33.3)] (P= 0.027). Among patients who received distal gastrectomy, the TLDG group showed more satisfaction with their body image than the LADG group [0 (0-0)vs0 (0-33.3)] (P= 0.002).
DlSCUSSlON
The advantages of TLG have been confirmed by many studies. These advantages include less surgical blood loss, faster postoperative recovery of gastrointestinal functions, a shorter postoperative hospital stay, a smaller incision and improved QOL[8,15,16]. However, no studies have evaluated the short-term efficacy of TLG and LAG in elderly patients.
In this study, we found that intraoperative blood loss in the TLG group was lower than that in the LAG group. However, no significant difference in the operation time was found between the 2 groups. In the subgroup analysis, the operation time for the TLDG group was significantly shorter than that for the LADG group, which is similar to previous results[17]. These results indicate that under the limitation of a small abdominal incision, extracorporeal anastomosis may reduce the surgical efficiency, while intracorporeal anastomosis is more convenient and seems to be easier to execute. Elderly patients have an increased risk of surgical complications due to underlying diseases, decreased physical performance and malnutrition. Therefore, choosing a reasonable surgical strategy is very important[18]. Previous results have shown that the incidence of postoperative complications in elderly patients undergoing LG is comparable with that in younger patients, confirming that laparoscopic surgery is a safe method for elderly patients with GC[19,20]. The results from this study indicate that the overall incidence of postoperative complications in the TLG group was significantly lower than that in the LAG group (16.5%vs26.3%,P= 0.010) and that the incidence of severe complications was comparable (3.9%vs4.3%,P= 0.830). Further analysis revealed that LAG and operation time were independent risk factors for complications in elderly patients. The following reasons may potentially explain these results. For experienced surgeons, anastomosis (especially esophagojejunal anastomosis) under laparoscopy may offer a clearer view and facilitate more precise and accurate manipulation. It may reduce the risk of postoperative complications for patients[21]. Moreover, the longer operation time is mainly due to obesity, advanced tumor stages, intraoperative erroneous injury and difficulties in gastrointestinal reconstruction, which potentially increase the risk of postoperative complications. Based on these results, TLG is a more suitable approach for elderly patients with GC. However, the operation time must be controlled to reduce the occurrence of postoperative complications.
Anastomosis-related complications are crucial indicators when assessing the safety of gastrointestinal reconstruction methods. A meta-analysis of 10 studies by Zhaoet al[22] showed that the incidence of anastomotic site-related complications after TLTG was similar to that after LATG[22]. Hanet al[23] demonstrated that the incidence of anastomotic leakage after TLTG was higher than that after LATG. This phenomenon may be due to the difficulty of dissociating the distal esophagus by intracorporeal anastomosis, which increases the risk of anastomotic ischemia[23]. On the other hand, the physician’s proficiency in intracorporeal anastomosis is also an important determinant of surgical safety[24]. In the group of elderly patients, we found no significant differences in the incidence of anastomotic site-related complications (anastomotic leakage, bleeding and stenosis) between the LTG and LAG groups (P> 0.05). The results of the subgroup analysis also suggest that intracorporeal anastomosis is as safe as extracorporeal anastomosis for both distal and total gastrectomy and does not significantly increase the risks of anastomotic complications.
When addressing postoperative complications, the impact of surgical methods on the QOL of GC patients has become a key factor for surgeons when selecting an appropriate surgical approach. The EORTC QLQ-C30 and STO-22 questionnaires have been commonly used to assess the QOL of GC patients in recent years[25]. The QOL of patients can be assessed based on overall health, cognition, social interaction and symptoms. Whether TLG can improve the QOL of patients after surgery is still controversial. Parket al[7] compared QOL within 1 year after TLTG and LATG, and the results indicated that postoperative dysphagia, pain, eating and odynophagia were significantly improved in the TLTG group compared with the LATG group[7]. Weiet al[26] used circular anastomosis and found that postoperative constipation, dysphagia and anastomotic complications were significantly improved in TLTG group patients compared with LATG group patients[26]. In a study by Woo, no significant difference in QOL was found between patients after TLDG and LADG, and various parameters could not reflect subtle differences in surgical invasiveness between TLDG and LADG[27]. Which may be due to the high expectations of changes in QOL in patients undergoing TLDG, potentially affecting their judgment of subjective symptoms[28]. Postoperative QOL changes in elderly patients are different from those in young patients, and the effects on their physical and role functions are more obvious[29]. Physical function significantly varies with age, and changes in the QOL of elderly GC patients after surgery require close attention. Kimet al[30] found that in patients who underwent TLG, the postoperative return of bowel movements was slower in elderly patients[30]. In this study, we found no significant difference in preoperative QOL parameters between the TLG group and the LAG group. The 3-mo follow-up results indicated that the scores for nausea, vomiting and constipation in the TLG group were significantly lower than those in the LAG group, which is similar to the results of previous studies. In addition, in terms of body image, patients in the TLG group seemed to be more satisfied with their postoperative body image changes, which may be related to the smaller length of the incision in TLG. The above results suggest that for elderly patients, TLG may be a key factor in improving postoperative QOL.
This study has some limitations. First, this study did not include patients who underwent proximal gastrectomy, mainly because most patients who underwent proximal gastrectomy in our center received extracorporeal anastomosis, and the variety of intracorporeal anastomosis methods may cause potential bias. Second, this study followed up on the QOL of the patients only at 3 mo after surgery, with no complete follow-up for 1 year. Further follow-up is needed to compare the effects of TLG and LAG on the QOL of elderly patients. Third, we retrospectively established the short-term efficacy of TLG for elderly GC patients. Further studies, such as multicenter prospective studies, need to be conducted to evaluate the clinical value of TLG for elderly patients with GC.
In summary, this study found that TLG is safe and feasible for elderly patients with GC. TLG has significant advantages over LAG in terms of intraoperative bleeding, postoperative exsufflation and hospitalization and the overall postoperative complication rate. We found that LAG and an operation time > 220 min were independent risk factors for postoperative complications. Therefore, we recommend that experienced surgeons preferentially choose intracorporeal anastomosis during gastrectomy for elderly GC patients under the premise of ensuring a shorter operation time.

Table 4 Quality of life using European Organization for Research and Treatment of Cancer Quality of Life Core Questionnaire and STO-22 questionnaire between laparoscopic assisted gastrectomy and totally laparoscopic gastrectomy group
CONCLUSlON
TLG is safe and feasible for elderly patients with GC and has outstanding advantages in reducing surgical bleeding, promoting postoperative recovery and improving QOL. We recommend that experienced surgeons prioritize TLG as a gastrectomy approach for elderly patients due to the shorter operation time.
ARTlCLE HlGHLlGHTS
Research background
The outstanding advantages of totally laparoscopic gastrectomy (TLG) over laparoscopic assisted gastrectomy (LAG) has been proved in many studies.
Research motivation
The safety and reliability of TLG for elderly patients with gastric cancer (GC) remain unclear.
Research objectives
To evaluate the short-term efficiency and quality of life (QOL) of TLG for elderly patients with GC.
Research methods
The clinicopathological data of 462 elderly patients aged ≥ 70 years who underwent LAG or TLG between January 2017 and January 2022 at Department of General Surgery, First Medical Center, PLA General Hospital were retrospectively collected. We compared the perioperative outcomes between TLG and LAG groups, and used univariate and multivariate analysis to figure out the independent risk factors of LG in elderly patients. QOL data before and 3 mo after surgery were collected to evaluate whether TLG is equally safe and feasible in elderly patients.
Research results
The overall incidence of postoperative complications in the TLG group was significantly lower than that in the LAG group (16.5%vs26.3%,P= 0.01). Furthermore, there was no significant difference in the incidence of anastomotic site-related complications or the incidence of severe complications between the TLG group and the LAG group (P= 0.599,P= 0.830). Binary logistic regression results indicated that LAG and operation time > 220 min were independent risk factors for postoperative complications in elderly patients with GC (P< 0.05). In terms of QOL, there were no statistically significant differences in various preoperative indicators between the LAG group and the LTG group (P> 0.05). Three months after surgery, patients in the TLG group were more satisfied with their body image.
Research conclusions
TLG is safe and feasible for elderly GC patients, especially in reducing surgical bleeding, promoting postoperative recovery and improving QOL.
Research perspectives
In the further study, we will refine the complete one-year follow-up of patients and conduct a multicenter collaborative prospective study to evaluate the clinical value of TLG more thoroughly for elderly patients with GC.
FOOTNOTES
Author contributions:Zhao RY, Li HH and Zhang KC equally contributed to this work; Zhao RY, Li HH, Zhang KC, Cui H, Deng H and Gao JW participated in the patient information collection; Zhao RY, Li HH and Zhang KC cleaned, analyzed the data and wrote the manuscript; Zhao RY, Li HH and Wei B revised the manuscript; Wei B designed and conceived this project; All authors have read and approved the final manuscript.
Supported byNational Basic Research Program of China, No. 2019YFB1311505; National Natural Science Foundation of China, No. 81773135 and No. 82073192; Natural Science Foundation of China for Youth, No. 82103593; Natural Science Foundation of Beijing for Youth, No. 7214252; and Program of Military Medicine for Youth, No. QNF19055.
lnstitutional review board statement:The study involving human participants was reviewed and approved by the Research Ethics Committee of Chinese PLA General Hospital.
lnformed consent statement:All the patients have signed the informed consent before participating in this study.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Data sharing statement:The original anonymous dataset is available on request from the corresponding author at weibo@301hospital.com.cn.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Rui-Yang Zhao 0000-0001-6619-9532; Ηang-Ηang Li 0000-0002-9117-7156; Ke-Cheng Zhang 0000-0002-9257-5607; Ηao Cui 0000-0003-1185-5322; Ηuan Deng 0000-0002-6144-2289; Jing-Wang Gao 0000-0001-5388-3626; Bo Wei 0000-0001-7386-2689.
S-Editor:Fan JR
L-Editor:A
P-Editor:Fan JR
杂志排行
World Journal of Gastrointestinal Surgery的其它文章
- Prediction factors for ischemia of closed-loop small intestinal obstruction
- Successful treatment of acute symptomatic extensive portal venous system thrombosis by 7-day systemic thrombolysis
- Retrorectal mucinous adenocarcinoma arising from a tailgut cyst: A case report and review of literature
- Minimally invasive endoscopic repair of rectovaginal fistula
- Laparoscopic appendectomy, stump closure and endoloops: A meta-analysis
- Effect of cardiac output - guided hemodynamic management on acute lung injury in pediatric living donor liver transplantation