Experimental study on the distribution and change of manganese in manganese exposure rats after manganese removal
2022-08-30anzhong
, , , , , ,g , , anzhong
(School of Public Health,Zunyi Medical University,Zunyi Guizhou 563099,China)
[Abstract] Objective To explore whether the brain tissue continues to maintain a high manganese state after manganese removal was related to the release of bone manganese.Methods Atomic absorption spectroscopy was recruited to quantify the content of manganese in brain tissue,blood and femur of SD rats after manganese exposure for 3 months,manganese exposure for 3 months and then manganese removal for 3 months,and manganese exposure for 12 months,respectively.Results After manganese exposure for 3 months,the level of blood manganese in manganese exposure group was higher than that in time-matched control group.In normal conditions,manganese was mainly distributed in brain tissue and bone,with little content in blood,and the concentration gradient was:cortex > striatum > hippocampus > femur > whole blood >cerebrospinal fluid (CSF).After manganese exposure for 3 months,manganese mainly accumulates in bone,and the concentration gradient was femur > striatum > hippocampus > cortex > whole blood > CSF.In manganese exposure for 3 months followed by manganese removal for 3 months,the content of bone decreased obviously,but it was still higher than that in other tissues,while the content of brain tissue did not change compared with that in manganese exposure for 3 months.The concentration gradient at this time was femur >whole blood > striatum > hippocampus > cortex > CSF.Before and after manganese removal,bone manganese was positively correlated with whole blood manganese,and weakly positively correlated with hippocampus and striatum.However,no correlation between bone manganese and cortex was shown.Conclusion Bone manganese plays "manganese pool" effect,accumulates a large amount of manganese in excessive exposure,releases manganese continuously after manganese removal to maintain high manganese level of brain tissue.This might be one of the reasons for the progressive aggravation of neuronal damage in occupational workers after manganese removal.
[Key words] manganese; neuronal damage; progressive aggravation; chronic experiment; brain
Manganese (Mn) is an essential trace element of human body,which is involved in the composition of manganese superoxide dismutase and glutathione synthase,and is also an important factor in the synthesis and metabolism of neurotransmitters[1-4].China is a major producer of ferromanganese alloy,with hundreds of thousands of employees.With the increasing popularity of cars,the massive use of gasoline antiknock (methylcyclopentadienyl manganese tricarbonyl (MMT)),as well as stainless steel products with excessive manganese in daily life,pesticides containing manganese,manganese pollution of drinking water and food,etc.may incur the general population exposed to manganese environment that exceeds physiological needs[5-7].Numerous studies have confirmed that excess manganese is one type of environmental neurotoxin[8-9],but until recent years,people gradually noticed that effect of manganese on neurological function may persist and be progressively aggravated after several years of cessation of occupational manganese exposure[3].On the one hand,this effect may be related to irreversible nerve damage caused by manganese,but it may also be related to maintaining excessive content of manganese in the brain after high manganese exposure,although the latter lacked direct evidence.
Studies showed that bone and brain tissue are the main target organs of manganese accumulation[9-11].The half-life of manganese in human bones can be up to 8-9 years,and bone manganese is highly positively correlated with manganese in striatum,hippocampus and CSF(CSF),bone manganese can better reflect the level of manganese accumulation in human body[12].We speculate that the accumulation of manganese in bones may form endogenous “manganese pool”.Manganese removal after exposure,bone manganese is released into blood and enters brain tissue to maintain the high load of manganese in the brain,which may be one of the reasons why the neurotoxicity of manganese poisoning is progressively aggravated after removal[13-15].
Accumulation and relative changes of manganese in brain tissue,blood and femur of SD rats were studied after manganese exposure and manganese removal after exposure to observe whether the content of manganese in brain tissue remained high level and the possible role of bone manganese.
1 Materials and methods
1.1 Animals and groups 60 SPF male SD rats weighing (280±20) g were provided by the experimental animal center of Third Military Medical University (animal certificate:SCXK (Yu) 2012-0005).Random grouping of animals:chronic experiment 30 rats exposed to manganese group (50 mg/kg Mn2+) and 30 rats in control group (sterilized ultra-pure water).Feeding conditions:room temperature 18-22 ℃,relative humidity 50%-60%.Light alternated with darkness every 12 hours,the rats drank and ate freely.After a week of adaptive feeding and then all rats were exposed to manganese by oral gavage for 12 months,5 times a week,once a day.Blood samples of 6 rats random selected from each group were taken from orbit to detect content of manganese at the 3rd,6th,9th,12th month.Three months later,7 rats in manganese exposure group (50 mg/kg Mn2+) and 7 rats from control group were randomly selected and sacrificed for tissue detection,and 6 rats were randomly selected from Mn exposure group treated as control group (manganese removal).Six months later,the 6 manganese removal rats and 6 control rats randomly selected from control group were sacrificed for tissue detection.All the remaining rats were sacrificed on 12th month for tissue detection.All operations were performed after anesthesia.
The experiment was completed from 8∶00 am to 10∶00 am every day.The relevant principles of animal management and animal ethical protection should be followed in the process of breeding and experiment.The experimental procedure is shown (Fig 1).
1.2 Solution preparation Manganese chloride:weighed 17.968 5 g MnCl2·4H2(adamas,99%,21136C),and a small amount of ultra-pure water was added to dissolve the water by ultrasound,then the volume of solution was fixed to 500 ml and filtered by 0.22 μm micro-porous filter membrane,finally kept at 4 ℃ for 2 weeks.
1.3 Materials The rats were anesthetized with 1% pentobarbital sodium,CSF was extracted via the dural puncture method with the improved microinjector under the direct vision improved by Yangzi.etc[16],blood was taken from abdominal aorta,and attained the brain by cutting off.Hippocampus,cortex and striatum were separated in ice bath conditions,and put into marked EP tube.Stripped the left femur of rats,all specimens stored at -80 ℃ to wait for inspection.
1.4 Sample preparation and the detection of manganese
1.4.1 Sample preparation Added 1ml whole blood in 1ml concentrated nitric acid,added 50 μl CSF in 50 μl concentrated nitric acid,added 2 ml of concentrated nitric acid in hippocampus,cortex and striatum weighed exactly.Placed the samples added with concentrated nitric acid in fume hood at room temperature,and waited for the samples to be digested until all samples were clear and bright yellow.Transferred all the digested samples to a clean and dry beaker,used the electric heating plate to remove acid at 100 ℃,the samples were takenout after the solution was nearly dried and stopped heating.When the temperature dropped to room temperature,fixed the volume by 1% dilute nitric acid (the volume of whole blood was set to 10 ml,CSF to 2 ml,hippocampus,cortex and liver to 4 ml).
Removed and accurately weighed excess fat and connective tissue of femur,then made thorough record,placed the samples in polytetrafluoroethylene crucible and ashed it in muffle furnace at (100±5) ℃ for 12 hours.After that,heated temperature to (450±5) ℃ and ashed samples continuously.Then closed muffle furnace,when the temperature dropped to room temperature,took out the samples in crucible,weighed the ash accurately and transferred them to a 10 ml small beaker.Added 3ml concentrated nitric acid into each sample and digested overnight.Heated all samples at 150±5℃ to remove acid after all samples were digested until all samples became bright yellow,stopped heating after the solution was nearly dry.When the temperature of the samples dropped to room temperature and fixed the volume by 1% dilute nitric acid to 10 ml[17].Determined content of manganese by graphite furnace atomic absorption spectroscopy (AAS,Varian,AA210Z) after diluting prepared samples to an appropriate multiple.
1.4.2 The detection of manganese During digestion and determination of graphite furnace atomic absorption,all the instruments were soaked overnight with 30% nitric acid solution,washed repeatedly with pure water and dried for standby.Set the specific parameters of manganese concentration according to the operation regulations of graphite furnace atomic absorption and startthe detection.
Drew standard curve:gradient diluted 1 mg/L manganese standard solution (national standard material network,BWB2069-2016) to 5 μg/L and drew standard curve.

2 Results
2.1 Levels of blood manganese at different time points of manganese exposure Level of blood manganese of all the manganese exposure group at the third,sixth,ninth,twelfth month was higher than those before manganese exposure(allP<0.05),but there was no statistically significant difference between various time points after manganese exposure for 3 months (allP>0.05); Also,after 3 months,level of blood manganese in manganese group was higher than those in time-matched control group (allP<0.05,Fig 2).
2.2 Accumulation and distribution of manganese in various tissues after manganese exposure After manganese exposure for 3 months,the content of whole blood,CSF,hippocampus,cortex,striatum and femur was all higher than those of the control group (allP<0.05).Among which,the increase of femur manganese was the highest (542.11%),followed by whole blood (481.52%),CSF manganese(247.29%),hippocampal manganese (173.08%),striatal manganese(151.72%) and cortical manganese (128.89%); After manganese exposure for 12 months,the content of manganese in all tissues was higher than that in the control group (allP<0.05).Among which,the increase of whole blood manganese was the highest (549.38%),followed by femur (519.30%),CSF manganese (275.12%),hippocampal manganese (167.94%),striatal manganese (165.56%) and cortical manganese (130.93%)(Table 1).There was not statistically significant difference between the 3rd and 6th month in all tissues (allP>0.05).
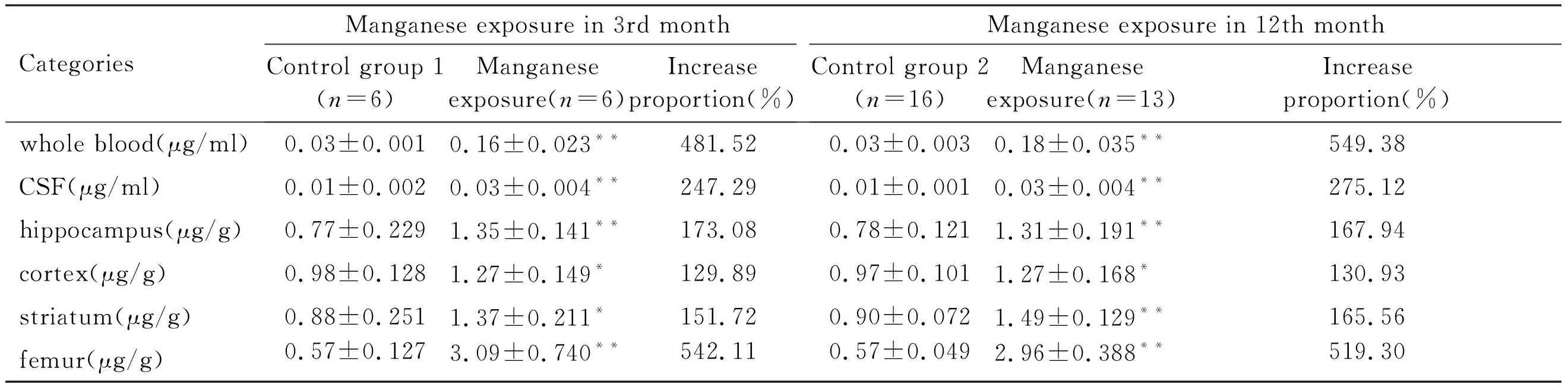
Tab 1 Accumulation of manganese
The concentration gradient of manganese in the control group was cortex > striatum > hippocampus > femur > whole blood > CSF; In the 3rd and 12th month,the concentration gradient of manganese in Manganese exposure group both were femur > striatum > hippocampus > cortex > whole blood > CSF (Fig 3).
2.3 Reduction and distribution of manganese in vivo after manganese removal Compared with that before manganese removal,the content of manganese in femur and whole blood decreased significantly (P<0.05),the content of manganese in femur and whole blood relatively decreased by 346.55% and 132.18% respectively(Table 2,Fig 4).However,the decrease of manganese in CSF,hippocampus,cortex and striatum was not statistically significant (P>0.05).When exposed to manganese,the relative increase level of bone manganese and whole blood manganese was the highest,and after manganese removal,the relative change level of bone manganese decreased sharply,which suggested that bone manganese might play “manganese pool” effect(Fig 4).
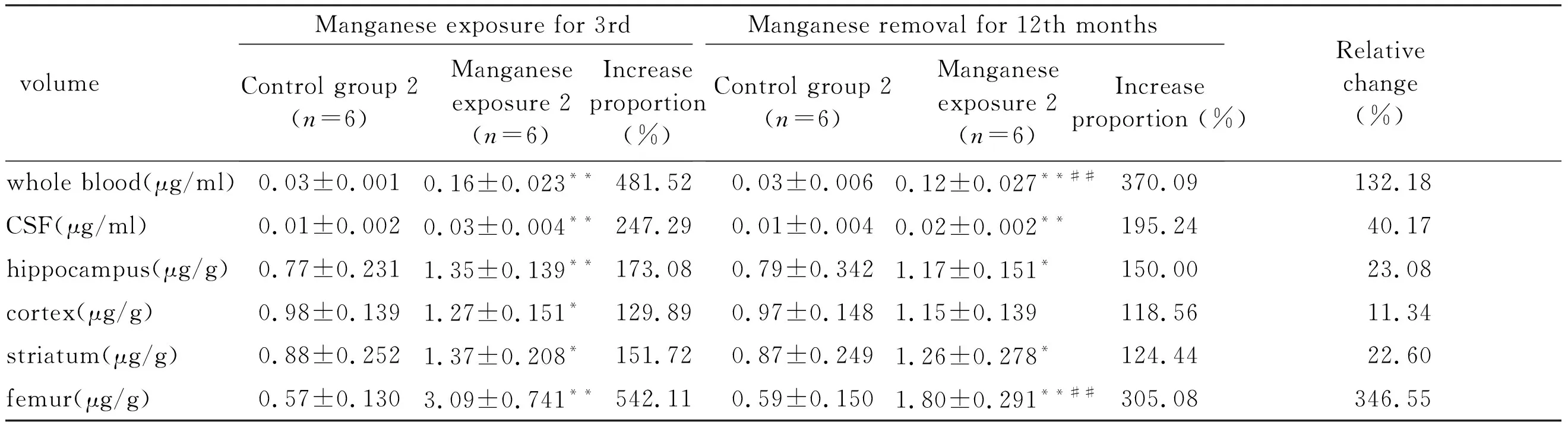
Tab 2 Reduction and distribution of manganese in vivo before and after manganese removal
2.4 Correlation analysis of bone manganese and brain manganese Before and after manganese removal,bone manganese was positively correlated with whole blood manganese (P<0.05),and weakly with hippocampus and striatum (P< 0.05),but not with cortex (P>0.05,Fig 5).
3 Discussion
Manganese is an essential trace element of human body[8,18].Considering that the actual exposure route of manganese is mostly through oral or respiratory intake[19],but oral dose is easier to accurately be grasped,so the chronic experimental model of excessive manganese was established by oral intragastric administration of manganese chloride.The study found that the blood manganese concentration of SD rats was equivalent to that of human chronic manganese exposure after 2 weeks of intragastric administration with 50 mg/kg gavage dose,5 days a week,once a day,which could simulate human chronic manganese exposure[11].Median lethal dose (LD50) of manganese chloride by oral gavage was 338 Mn/kg,and 50 mg/kg was equivalent to 15% of LD50.Meanwhile,the US Agency for Toxic Substances and Disease Registry(ATSDR) has shown that manganese exposure through oral gavage is similar to inhalation[11].After 6 weeks of manganese exposure through oral gavage,the accumulation of manganese in bone was basically stable,and the half-life of manganese in brain tissue of rats was about 52-74 days[19].Therefore,it was reasonable and feasible to establish the model of manganese exposure and manganese removal by using 50 mg/kg Mn2+gavage for three months in this study.
Excessive accumulation of manganese in the body may induce dysfunction of excretory system,retardation of development,abnormal transport of manganese,and abnormality of nervous system,etc[8].Epidemiological investigation showed that the neurotoxicity induced by manganese still had a trend of progressive aggravation after manganese removal.However,due to the lack of noninvasive assessment tools for the distribution and accumulation of manganese in the brain,it is still unable to effectively evaluate the accumulation and distribution of manganese in the brain of occupational workers exposed to manganese after leaving manganese environment[12].Therefore,it is not clear how the level of manganese in the brain tissue of professional workers changes after manganese removal and whether the progressive nerve injury after manganese removal is related to the maintenance of high level of manganese in the brain tissue[20-21].
In this study,we found that the normal concentration gradient of manganese in all tissues was cortex > striatum > hippocampus > femur > whole blood > CSF.After manganese exposure for 3 months,the content of manganese in whole blood,CSF,hippocampus,cortex,striatum and femur increased significantly,among which the content of bone manganese increased the most (542.11%),followed by whole blood (481.52%),CSF manganese (247.29%),hippocampal manganese (173.08%),striatal manganese(151.72%)and cortical manganese(128.89%).When exposed to manganese in 12th month,the relative increase range of bone manganese was slightly lower than that of blood manganese,and the relative increase of manganese in the remaining tissues was in the same order as that of manganese exposure in 3rd month.In addition,the data showed that manganese was mainly accumulated in the bone after manganese exposure for 3 and 12 months and the concentration gradient was femur > striatum > hippocampus > cortex > whole blood > CSF.
After manganese removal for 3 months,in addition to the cortex,rates in manganese exposure group content of manganese in all tissues was still higher than that of the control group (P< 0.05).The concentration of manganese in all tissues of the manganese exposure group decreased differently,among which the relative decrease of femur manganese was the highest (346.55%),followed by whole blood manganese(132.18%),CSF manganese(40.17%),hippocampus manganese (23.08%),cortex manganese (22.06%),striatum manganese (11.34%).There was a statistically significant difference between the content of manganese in the femur,whole blood after manganese removal and before (P<0.05).However,there was no statistically significant difference in the content of manganese in CSF,hippocampus,cortex,striatum before and after manganese removal (P>0.05).The results indicated that the content of manganese in bone decreased sharply after manganese removal,while the content of brain tissue basically remained stable,but the concentration of manganese in bone was still much higher than that in brain at this time.
These results suggest that bone or blood plays similar “manganese pool” effect,“manganese pool” continues to release high level of manganese in vivo after manganese exposure.Among them,due to ease to collect,less amount to need,high sensitivity,blood is often used as a biological sample for the detection of content of manganese in human body in occupational workers exposed to manganese[22-23].The blood manganese concentration of the rats was maintained at about 5 times of that of the control group,without the time-dependent effect of the content of blood manganese was observed using 50 mg/kg Mn2+gavage from 3 to 12 months.Besides,the half-life of manganese in the blood was about 1.83 h[24],and the blood flow was fast and manganese could be quickly removed,so it was unlikely to accumulate manganese in peripheral blood system[24-26].At the same time,we did not observe the progressive accumulation of bone manganese at the observation time point at the 3rd and the 12th month,which indicates that the time of full load of bone accumulation was less than 3 months,long-term exposure could not lead to a greater accumulation of bone manganese.However,a large number of studies have confirmed that about 43% of manganese in human body is mainly stored in the bone[11],and significant reduction of bone manganese was observed in this experiment after manganese removal,which indicates release effect of bone manganese is very obvious.The released manganese is mainly transported to brain through peripheral blood,thus maintains the relative stability of brain manganese level.
Therefore,we speculate that after the cessation of exogenous manganese exposure,the "manganese pool",that is,the manganese in the bone can also be released slowly into blood and transported to brain through blood circulation to maintain the sustained high level of brain manganese which causes sustained damage of nervous system.In addition,epidemiological studies have found that the intelligence of adults with a history of manganese exposure in childhood is generally lower than that of ordinary contemporaries[26-29].And animal experiments show that even after the cessation of manganese exposure,the brain damage caused by manganese is still aggravated,which may also be evidence of the presence of “manganese pool”.
Manganese exposure remains less than 3 months,manganese by oral gavage mainly enters brain tissue and bone through blood for accumulation,excessive manganese continues to remain exposed for 3 months,the level of bone manganese reaches stable,and the level of brain manganese level continues to increase.Removed manganese for 3 months,the time of manganese removal is longer than half-life 52-71 days of brain manganese.Firstly,the bone manganese is released into blood and then transported into brain to maintain the level of manganese,blood system plays mediation and the effect of the bridge in the whole process.
Zheng etc[30-31]have ever tried to use non-invasive biomaterials such as hair and nails containing manganese to reflect the level of manganese in human body,but similar exposure groups had significantly different levels of manganese in their hair and nails,which may be caused by contamination of biomaterials by exogenous manganese.In the absence of complete removal of exogenous contamination,hair and nails can still not reflect the level of manganese accumulation in human body.At the same time,some researchers found that bone manganese in workers exposed to occupational manganese may act as a biomarker for the accumulation of manganese in human body through detection,but there is no laboratory evidence to verify this[12-13,15,32].The results of this study indicate that bone manganese can be used as a marker of cumulative exposure after continuous manganese exposure,but could not be used as a marker of level in human body,especially the level of brain tissue after manganese removal.
According to this study,bone manganese may play “manganese pool” effect in the occupational workers exposed to manganese,and slowly release into brain after occupational workers retired and leaved from manganese,so as to maintain high level of manganese in brain,which may be one of the reasons for the progressive aggravation of neurotoxicity caused by manganese.Further large-scale sample studies of population are needed to confirm this in the future,so as to provide reasonable suggestions for healthy management services for occupational workers exposed to manganese and those who have been separated from manganese exposure.
