Epidemiology of pelvic and acetabular fractures across 12-mo at a level-1 trauma centre
2022-08-19RoryCuthbertSamuelWaltersDavidFergusonEdwardKaramJonathanWardHomaArshadPaulCulpanPeterBates
lNTRODUCTlON
Major trauma/suicide remains the leading cause of death under the age of 45 in the United Kingdom (UK)[1]. In an effort to centralise trauma care and optimise outcomes, the National Health Service (NHS) introduced the Trauma Network System in 2012[2]. This designated 27 hospitals in England as Major Trauma Centres (MTCs) responsible for the specialist management of severely injured patients. 22 MTCs are responsible for the management of adult pelvic and acetabular trauma[3].
To our knowledge, this is the first study to analyze the epidemiology of high-energy (non-fragility) pelvic and acetabular trauma over a one-year period at a major trauma centre in the United Kingdom since introduction of the Trauma Network System. Given evolving safety measures and public travel preferences, the primary objectives were to characterise the epidemiology of current pelvic and acetabular fractures and their associated injuries, to demonstrate the wide-ranging resources required to care for these patients and explore opportunities for future injury prevention research.
MATERlALS AND METHODS
Study design
This retrospective observational study analyzed consecutive patients presenting to a level-1 trauma centre in the UK between December 2017 and December 2018. Research and audit approval was obtained from the Clinical Effectiveness Unit, and the NHS Research Ethics Committee decision tool excluded need for ethical review.
The NHS Research Ethics Committee decision tool excluded need for ethical review as this was a retrospective observational study.
Data collection
Orthopaedic multidisciplinary team documentation, consultant radiology reports and electronic patient records were analyzed by orthopaedic registrars (residents) to populate a standardised collection proforma. The following study outcomes were recorded: age, gender, pelvic or acetabular fracture (pelvic ring fracture only, pelvic ring and acetabulum fracture, acetabulum fracture only, iliac wing fracture, sacral body fracture, spinopelvic dissociation, other), Young-Burgess classification for pelvic ring fractures - lateral compression (LC) 1/2/3, anteroposterior compression (APC) 1/2/3, vertical shear (VS) or combined[5], open pelvic or acetabular injury, mechanism (fall, crush injury, other and road traffic accident which was further subdivided into pedestrianvehicle, vehiclevehicle and cyclistvehicle), suicide attempt, intensive care admission, head injury (AIS ≥ 1), abdominal injury (AIS ≥ 1), spine fracture, upper limb fracture / dislocation, lower limb fracture / dislocation, pelvic or acetabular surgery, number of further orthopaedic surgeries during admission, length of stay (days) and 30-d mortality.
Statistical analysis
Statistical analysis to compare groups within the study was performed using Fisher’s exact test for categorical variables. This was preferred to the Chi-square test due to small numbers in some categories. The-value for statistical significance was set at < 0.05. Statistical analysis was performed using Stata version 15.1 (Stata Corp LLC, College Station, Texas).
RESULTS
Epidemiological characteristics
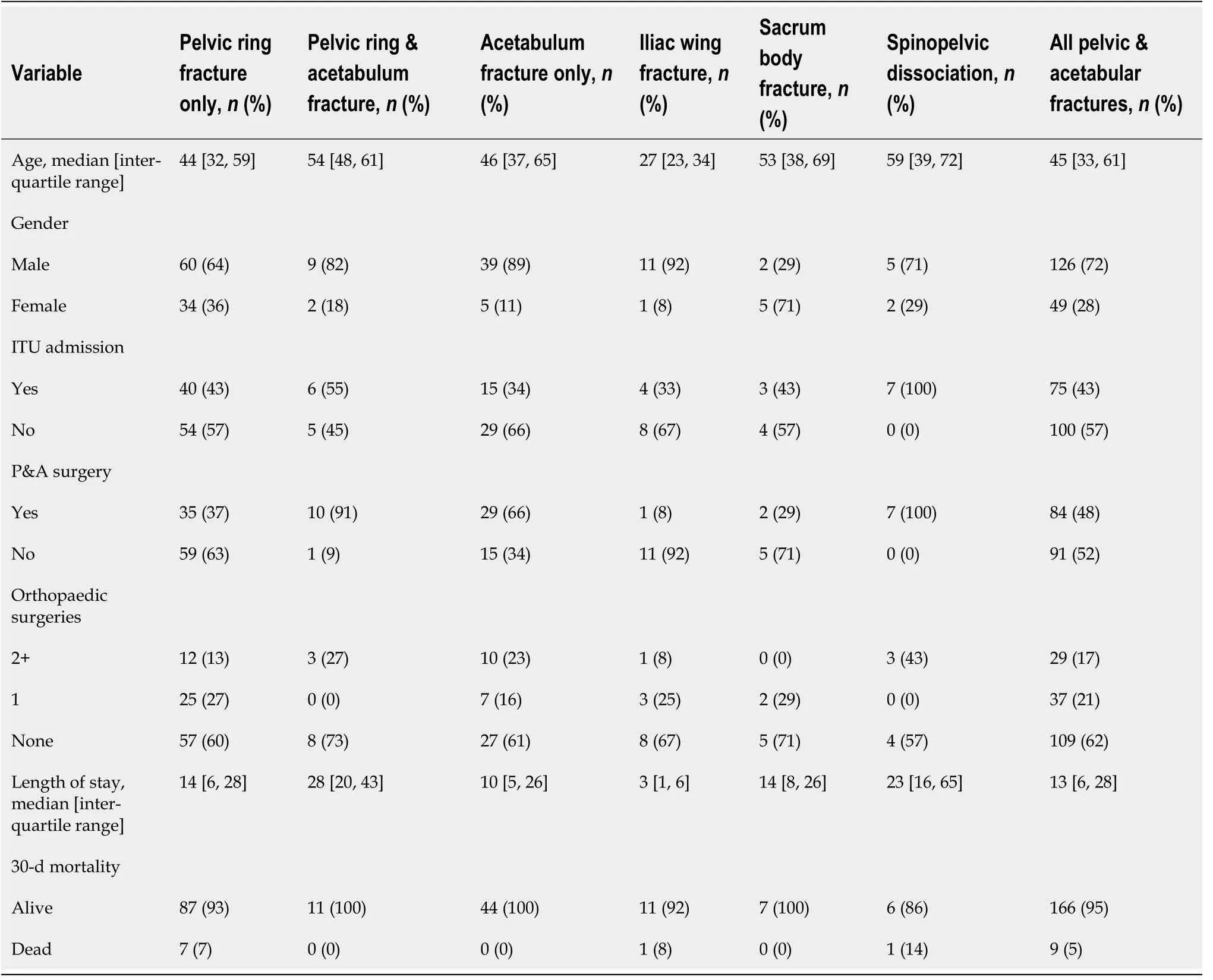
72% of all pelvic and acetabular fractures occurred in male patients at a median age of 45 years. 48% of patients required pelvic or acetabular surgery, with 38% undergoing additional surgery for other orthopaedic injuries. 43% of patients were admitted to intensive care with a median total hospital stay of 13 d. The 30-d mortality for all high-energy pelvic and acetabular fractures was 5% with only 1.7% of patients dying within the first 24 h of injury (Table 1).
Spinopelvic dissociation was associated with the greatest likelihood of additional surgery for other orthopaedic injuries (43%), and the highest 30-d mortality rate (14%). 37% of pelvic ring fractures required surgical intervention comparative to 66% of acetabular fractures. Combined pelvic ring and acetabular fractures were associated with the longest median total hospital stay of 28 d (Table 1).
I learned this with a laugh one morning after delivering a calf5. When it lifted up its fluffy6() head and looked at me, its eyes held the absolute bewilderment(,) of the newly born. A moment before it had the even black nowhere of the womb, and suddenly its world was full of colour, movement and noise. I’ve never seen anything so shocked to be alive.
Mechanism of injury
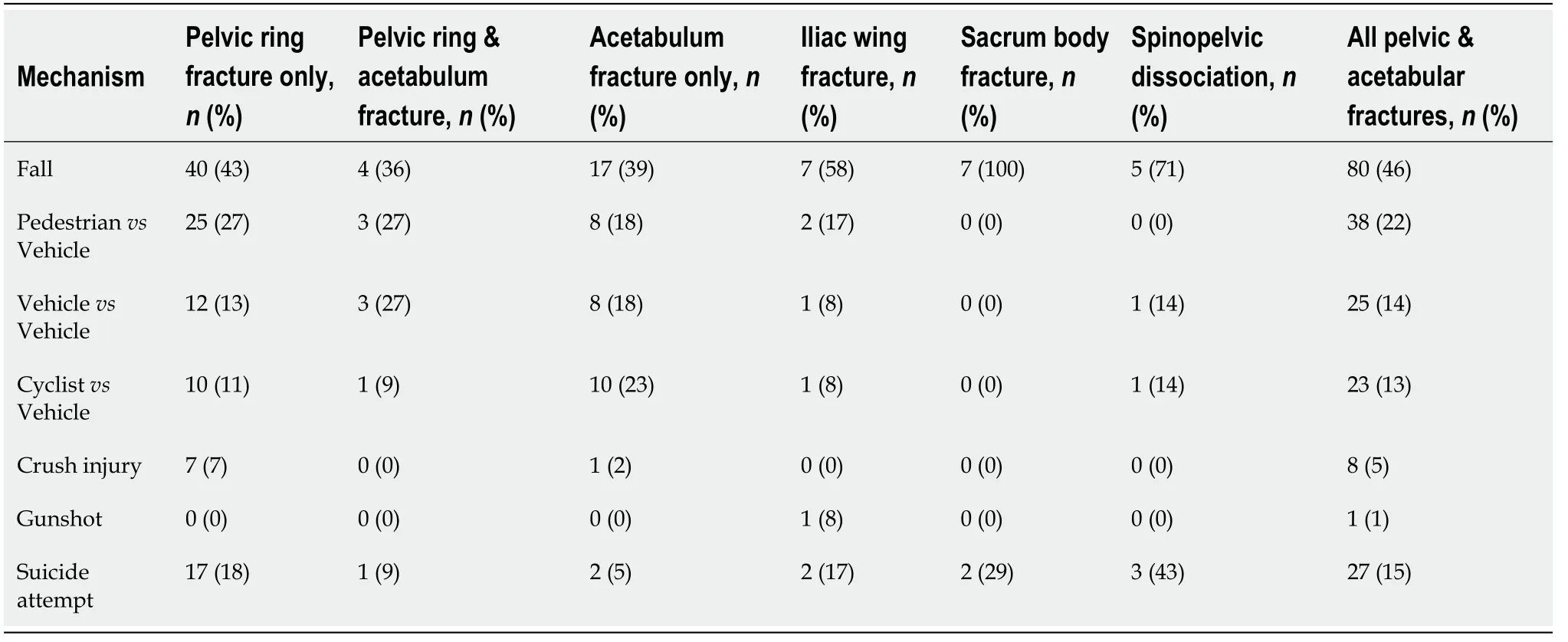
51% of pelvic ring fractures occurred following road traffic accidents, 43% were the result of falls from height and 7% were secondary to crush injuries. Road traffic accidents were responsible for 59% of acetabulum fractures with 39% due to falls. The most common subcategory of road traffic accident in pelvic ring fractures was pedestrianvehicle (27%). The most common subcategory of road traffic accident in acetabular fractures was cyclistvehicle (23%).
So first with one blow of the Sword of Sharpness he cut the iron chain that bound her, and then he asked her what she did there, and why men treated her so cruelly
This study sought to characterise the epidemiology of high-energy pelvic and acetabular trauma, to demonstrate the wide-ranging resources required to care for these patients and explore opportunities for future injury prevention research.
Associated injuries
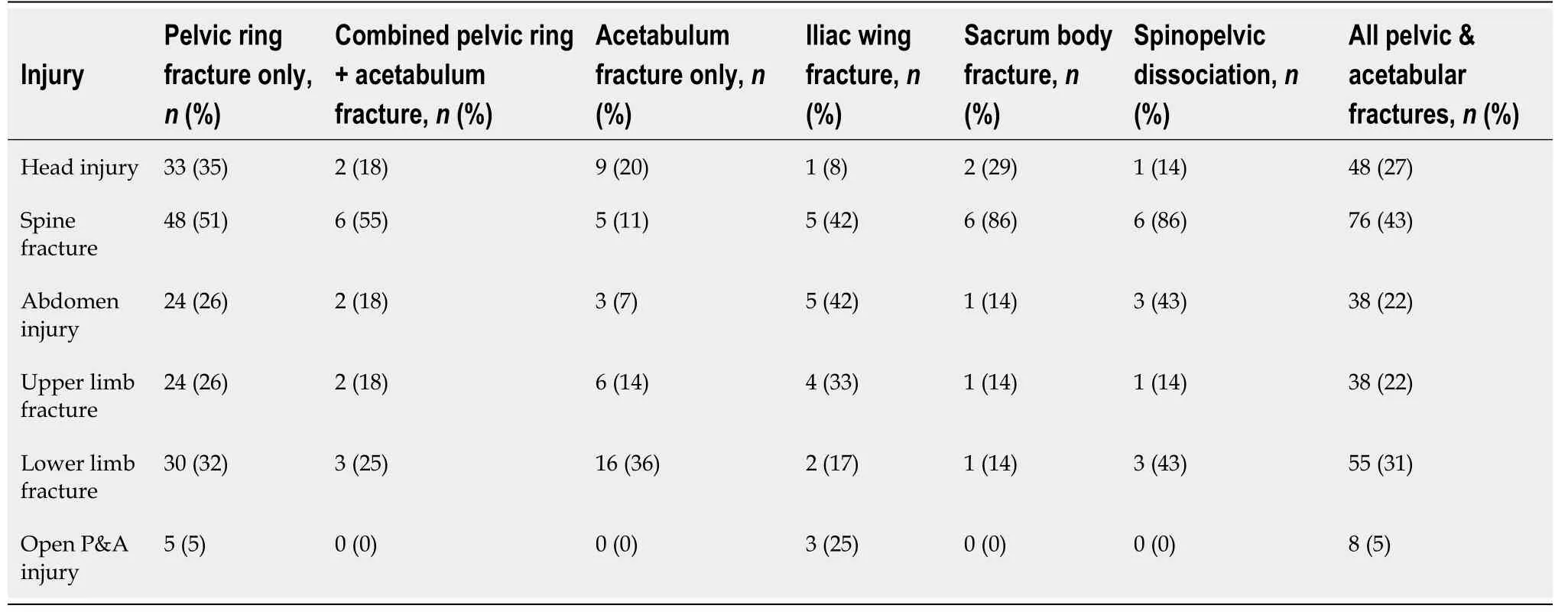
43% of all pelvic and acetabular fractures had an associated spine fracture. This was followed by lower limb fractures (31%), head injury (27%) and upper limb fractures (22%). 5% of all pelvic and acetabular fractures were open injuries (Table 3).
25. The sexton: An official who looks after the church (Oxford 764). Like his superior, he is not motivated by greed but by proper conduct or place. Return to place in story.
Just two days before Christmas, however, a storm swept through the area, dumping more than an inch of rain. The roof of the old church sprung a leak just behind the altar. The plaster soaked up the water as if it were a sponge and then crumbled3, leaving a gaping4 hole in the wall.
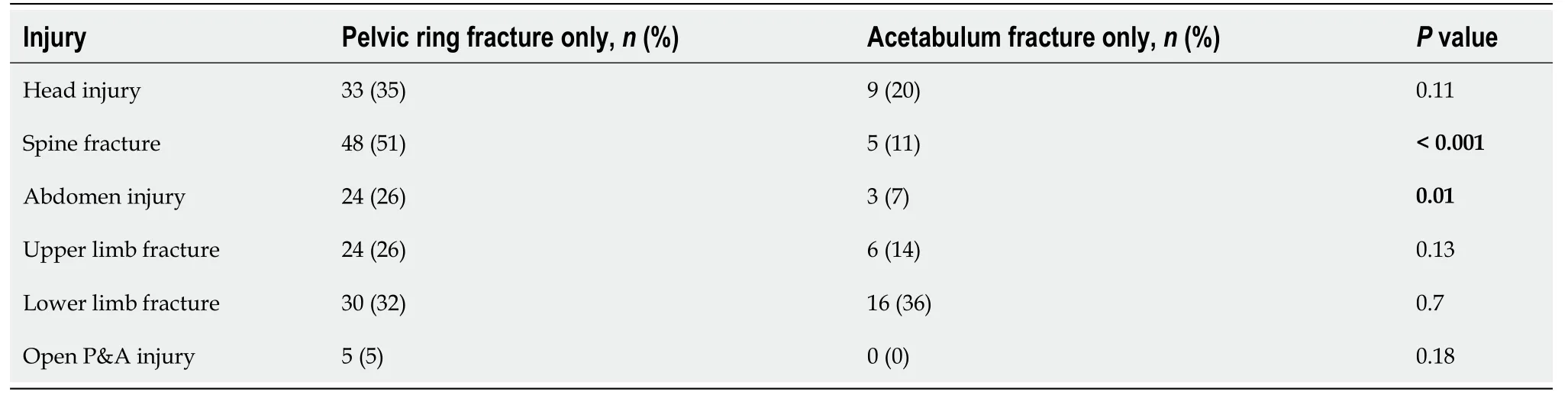
Comparison of pelvic ring and acetabulum fractures demonstrated a statistically significant association between pelvic ring fractures and both abdominal injury (= 0.01) and spine fractures (< 0.001) (Table 4).
Epidemiological characteristics based on the Young-Burgess classification
59% of acetabular fractures occurred following road traffic accidents and 39% were secondary to falls from height. Again, this is lower than the incidence of acetabular fractures in road traffic accidents observed globally: 66% of acetabular fractures in Qatar were attributable to road traffic accidents and 28% were the results of falls from height[9].

DlSCUSSlON
Non-fragility pelvic and acetabular fractures are the result of high-energy trauma. In our study, 47% of pelvic ring injuries were secondary to road traffic accidents and 40% followed falls from height. The incidence of road traffic accidents in pelvic ring fractures is lower than the incidence observed globally (road traffic accidents are reported as being responsible for 77% of pelvic ring fractures in India, for example)[6]. Data in the UK from 1989-2001 demonstrated 63% of pelvic ring fractures were attributable to road traffic accidents[7]. The reduced incidence in our study can be explained by the progressive improvement in UK road and vehicle safety, which is illustrated by government figures demonstrating the decline in road traffic accidents causing serious injuries and fatalities[8]. This skew away from road injuries may also represent the local inner-city population, many of whom are socially deprived, with unusually high incidences of interpersonal violence and mental illness. Accordingly, it is notable that attempted suicide contributes to 15% of the high-energy injuries in our study.
He remembered quite well that the right-hand way was short and dangerous, but he bethought himself too that whatever was written on his forehead would happen, and took the forbidden road
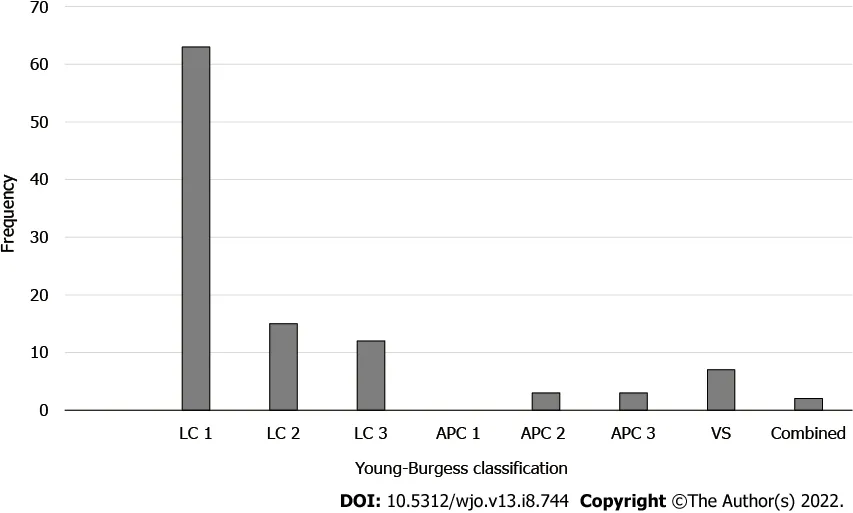
The breakdown of pelvic ring fractures based on the Young-Burgess classification is illustrated in Figure 1. There was a statistically significant difference between classification-types when the mechanism of injury was a fall (= 0.03) or road traffic accident (= 0.01). Falls were responsible for 86% of VS fractures, and 96% of all pelvic ring injuries secondary to road traffic accidents were LC-type. Crush injuries occurred more frequently in APC-type injuries (50%) but this did not reach statistical significance (= 0.05) (Table 5).
Cuthbert R designed the research study, performed data acquisition, and wrote the manuscript; Walters S, Ferguson D and Karam E designed the research study and performed data acquisition; Ward J, Arshad A, Culpan P and Bates P contributed towards conception of the study and final editing; all authors revised the article critically for important intellectual content, and provided final approval for the paper to be published.
15% of all pelvic and acetabular fractures occurred after a suicide attempt. Analysis of injury patterns demonstrates accidental falls are associated with upper limb injuries secondary to self-protection, whereas suicide attempts are associated with pelvic and acetabular fractures following direct impact or transmitted axial forcesthe hip joint[13]. De Moore illustrated 54% of patients who attempted suicide by jumping from height were psychotic at the time of the incident - contrasting with 4% of patients who attempted suicide using a firearm[14]. This highlights the importance of dual orthopaedic and psychiatric care in the acute management and rehabilitation of these vulnerable patients. The success of this approach is evident in the literature: in a Swedish study of 12 patients who had attempted suicide by jumping from height, all patients were alive at 4 years with 75% reporting satisfactory quality of life outcomes[15]. We do not have outcome data on those who attempted suicide in our study.
The word alone Gerda understood very well, and knew how much it expressed. So then she told the crow the whole story of her life and adventures, and asked him if he had seen little Kay.
Due to the high-energy mechanisms involved, pelvic and acetabular fractures are often associated with further injuries. In our study, lower limb fractures were observed in 32% of pelvic ring fractures and 36% of acetabular fractures. This is comparable with epidemiological analysis in India demonstrating lower limb fractures in 29% of pelvic ring fractures and 26% of acetabular fractures[6,16]. When comparing pelvic ring and acetabular fractures, there was a significant association between pelvic ring fractures and both spine fractures (< 0.001) and abdominal injury (= 0.01). 5% of our patients after high energy trauma had open injuries. This underlines the importance of the presence of multidisciplinary surgical teams at trauma calls; and supports British Orthopaedic Association Standards for Trauma guidance that all patients suffering high-energy trauma should have an examination of the perineum and rectum documented on arrival[17].
Despite our study solely analysing high-energy pelvic and acetabular fractures, the mortality rate was only 5% with just 1.7% of patients dying within the first 24 h of injury. In Giannoudis’ largescale study of UK pelvic ring fractures published in 2007, the 3-mo mortality was 14.2% with a median time to death of 6.2 h[7]. This is likely a reflection of the vast multidisciplinary advancements in acute haemorrhage control - both in a pre- hospital setting and operativelypelvic packing and interventional radiological techniques[18,19].
The Young-Burgess classification is the most widely used classification system for pelvic ring fractures and has been incorporated into Advanced Trauma Life Support guidelines[20]. This characterises pelvic ring injuries mechanistically, correlating with the direction and location of applied force[5]. In our study, there was a statistically significant association between falls and VS fractures (= 0.03), and road traffic accidents and LC fractures (= 0.01). The association between road traffic accidents and LC fractures may partly be explained by analysis demonstrating an increased risk of pelvic fracture following high magnitude side door or door panel intrusion in lateral impact crashes[21]. The need for improved lateral impact vehicle safety is evident, and in 2020 the European New Car Assessment Programme upgraded side mobile barrier testing to promote strengthening around the Bpillar (between the side doors of a car), fitment of side airbags and development of energy absorbing structures in seats and door panels[22].
The management of pelvic and acetabular fractures consumes considerable hospital resource. The literature has demonstrated pelvic fracture patients have more intensive care admissions (24.5%11.7%) and longer inpatient stays (158 d) than any other high-energy trauma patients[7]. In our study, intensive care admission was necessary in 43% of patients, with a median total hospital length of stay of 13 d. Furthermore, 48% of patients required pelvic or acetabular surgery, with 38% undergoing additional surgery for other orthopaedic injuries. British Orthopaedic Association Guidelines advise reconstruction of the pelvic ring should occur within 72 h of stabilisation of the patient’s physiological state[17], with Willett demonstrating time to surgery is a significant predictor of radiological and functional outcome for both elementary and associated displaced fractures of the acetabulum[23]. Therefore, it is crucial that major trauma centres allocate sufficient bed space and theatre capacity for the dedicated management of pelvic and acetabular fractures.
This study has limitations which must be considered when interpreting findings. Patients could only be included if they had undergone computed tomography of the pelvis to allow fracture classification. This meant patients who died in a pre-hospital or very early ED setting, prior to undergoing computed tomography of the pelvis, were excluded from analysis. We acknowledge the inevitable effect of geographical and national variation in terms of making comparisons with other centres around the world. The single centre studied is an inner-city level-1 facility with high rates of interpersonal violence, mental illness and low socioeconomic status, compared with the rest of the UK. Therefore, the distribution of injuries will inevitably reflect this diversity. Comparison between nations is also difficult to control due to cultural, legal and behavioural differences within the population which will also affect injury types and mechanisms - examples include the use of roundabouts in the UK and Europestop junctions in the United States. Suicide by gunshot is rare in the UK and Europe but much more common in United States and countries where firearm accessibility is relatively high, which may account for the high proportion of suicide falls from height in our series. Similarly, we recorded no pelvic or acetabular injuries resulting from gunshots, which would be much more common in other centres around the world. Moreover, the authors acknowledge the lack of clinical or radiological follow-up in this study. Ideally, an epidemiological study would be complemented by outcomes data, but this was not available for the cohort studied. Finally, analysis of the distribution of acetabular fractures in accordance with the Letournel and Judet classification system was not included in this study.
A principle of NHS funding is that insurance industries have a legal obligation to pay healthcare costs for patients who have been injured in an accident and have successfully claimed personal injury compensation. The tariff for the Injury Cost Recovery Scheme is currently capped at £915 per day with a maximum charge of £54682. Outpatient appointments are not funded by the scheme once the patient has received inpatient treatment[24]. Given the estimated cost of an intensive care bed alone is £1932 per night (which 43% of patients in our cohort required)[25], future research should analyse the direct cost of pelvic and acetabular fractures to help determine whether the current compensation arrangements adequately reimburse major trauma care.
CONCLUSlON
Pelvic and acetabular fractures most commonly occur in young male patients following high-energy trauma and are associated with concomitant orthopaedic injuries (most commonly spine and lower limb fractures), intensive care admission and long inpatient stays. The vast majority of pelvic ring injuries secondary to road traffic accidents are lateral compression type. Injury prevention research should seek to drive advancements in lateral impact cycle and motor vehicle safety, along with mental health surveillance for those deemed to be potential suicide risks.
ARTlCLE HlGHLlGHTS
Research background
To optimise trauma outcomes, the National Health Service introduced the Trauma Network System in 2012 which designated 27 hospitals in England responsible for the specialist management of severely injured patients. To our knowledge, this is the first study to analyse the epidemiology of high-energy pelvic and acetabular trauma over a one-year period at a major trauma centre since introduction of the Trauma Network System.
Research motivation
Non-fragility pelvic and acetabular fractures are the result of high-energy trauma. Despite evolving safety measures, high-energy trauma/suicide remains the leading cause of death under the age of 45 in the United Kingdom. Therefore, it is critical that research explores opportunities for future injury prevention in these high-risk patients.
Ogre fell down and broke his crown, and the beanstalk came toppling after: Jacobs uses a humorous reference to another Jack, this time the Jack in the Jack and Jill nursery rhyme, to gloss64 over the ogre s death:Jack and Jill went up the hill,To fetch a pail of water;Jack fell down And broke his crown,And Jill came tumbling after
Research objectives
71% of spinopelvic dissociations and 100% of sacrum body fractures were secondary to falls from height. 15% of all high energy pelvic and acetabular fractures were the result of a suicide attempt (Table 2).
Research methods
227 consecutive patients at a level-1 trauma centre with pelvic and acetabular fractures were analyzed over a one-year period. Paediatric patients, fragility fractures and patients without computed tomography of the pelvis were excluded leaving 175 patients for inclusion in the study. Statistical analysis was performed using Fisher’s exact test for categorical variables.
59. My story is done. See! there runs a little mouse; anyone who catches it may make himself a large fur cap out of it: This ending reflects the oral sources from which the tale came. Storytellers would often end or begin their tales with short verses to set or change the tone of the audience. Verses at the end of the tale often contained a moral or a request for money as a tip for the story provided. Here the verse effectively ends the tale and makes a small attempt to lift the overall somber142 and scary tones of the story despite its happy ending.Return to place in story.
Research results
72% of pelvic and acetabular fractures occurred in male patients at a median age of 45 years. 15% were the result of a suicide attempt. 48% of patients required pelvic or acetabular surgery, with 38% undergoing further surgery for additional orthopaedic injuries. Vertical shear pelvic ring fractures were associated with falls (= 0.03) while lateral compression fractures were associated with road traffic accidents (= 0.01).
Research conclusions
High-energy pelvic and acetabular fractures are associated with concomitant orthopaedic fractures (most commonly spine and lower limb). Most pelvic ring injuries secondary to road traffic accidents are lateral compression type illustrating the need for future research to drive advancements in lateral impact vehicle safety.
Research perspectives
Future research should drive advancements in lateral impact vehicle safety given the statistically significant association between lateral compression fractures and road traffic accidents. Additionally, research should focus on mental health surveillance strategies for patients deemed to be potential suicide risks.
Then a servant fetched in the polluted, blue-eyed headsman, who asked: Whose sun of life has come near its setting? took the prince by the arm, placed him upon the cloth of execution, and then, all merciless and stony52 hearted, cut his head from his body and hung it on the battlements
FOOTNOTES
Cyclistvehicle collisions were the commonest cause of acetabular fractures in road traffic accidents, and were responsible for 11% of pelvic ring fractures. Self-service cycle-hire schemes, cycleto-work tax incentives and large-scale investment in cycling infrastructure has triggered a surge in cycling popularity in the UK. In Ireland, a 90% increase in cycling-related acetabular and pelvic fracture referrals was observed between 2016 and 2017[10]. There is a paucity of literature analysing pelvic and acetabular fractures in cyclists. Bass hypothesises that cyclists attached to their pedals by straps or clips are likely to fall directly onto the hip which could promote acetabular fractures[11]. Similarly, Cerynik reports a case of a professional cyclist falling on the right side and sustaining a hyperextension injury to the left hip which remained clipped in the pedal[12]. Future research should seek to develop understanding of the mechanism of pelvic and acetabular fractures in cyclists and drive cycle safety advancements similar to those witnessed in motor vehicles.
227 patients with pelvic and acetabular fractures were identified using Abbreviated Injury Scale (AIS) codes on the institution’s prospectively maintained Trauma Audit and Research Network database. All adult patients (≥ 18 years) with pelvic or acetabular fractures confirmed on computed tomography were included. Paediatric patients (< 18 years), fragility fractures (in accordance with the World Health Organisation definition as falls from standing height or less)[4] and patients who did not undergo computed tomography of the pelvis were excluded. This left a total of 175 patients for inclusion in the study.
Informed consent was not required for the above study as data was collected retrospectively and anonymized.
All authors report no relevant conflict of interest for this article.
When he got there he gave the messengers who brought her a letter of thanks and a handsome present for their master and rewards for themselves; and then without delay he took the poor woman and her tiny baby-boy up on to his camel and rode off to a wild desert
No additional data are available.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Once, while he was taking a journey, a foot-bridge gave way under him; once he was attacked by armed robbers; a rock rolled down upon him in a mountain pass; a heavy stone coping fell from a roof at his feet in a narrow city alley
United Kingdom
Rory Cuthbert 0000-0001-6211-3789; Samuel Walters 0000-0002-3454-4482; David Ferguson 0000-0003-2876-8225; Edward Karam 0000-0002-5737-7998; Jonathan Ward 0000-0001-7601-4378; Homa Arshad 0000-0002-7045-2817; Paul Culpan 0000-0003-2557-9242; Peter Bates 0000-0002-9776-3930.
General Medical Council, No. 7455521; Royal College of Surgeons, No. 9109620; and British Orthopaedic Association, No. 20619.
Wu YXJ
A
Wu YXJ
杂志排行

World Journal of Orthopedics的其它文章
- Rates of readmission and reoperation after operative management of midshaft clavicle fractures in adolescents
- Bilateral hip heterotopic ossification with sciatic nerve compression on a paediatric patient-An individualized surgical approach: A case report
- Quantitative alpha-defensin testing: ls synovial fluid dilution important?
- Effect of pelvic fixation on ambulation in children with neuromuscular scoliosis
- Risk modeling of femoral neck fracture based on geometric parameters of the proximal epiphysis
- Higher cost of arthroplasty for hip fractures in patients transferred from outside hospitals vs primary emergency department presentation