Anterolateral complex of the knee: State of the art
2022-08-19LuigiSabatiniMarcelloCapellaDanieleVezzaLucaBarberisDanieleCamazzolaSalvatoreRisitanoLucaDroccoAlessandroMass
lNTRODUCTlON
Anterior cruciate ligament (ACL) reconstruction techniques have sought to restore knee kinematics and reduce rotational instability. Since the 1970s[1] the idea that anterolateral rotatory instability (ALRI) was due not only to ACL injury, but also to the structures of the anterolateral complex (ALC), began to catch on. Over the last decade, awareness of the ALC has increased, especially since the anterolateral ligament (ALL) has been described and identified[2]. Several biomechanical studies have been carried out and different reconstruction techniques have been proposed.
Roy and I had invested a great deal of time and work into the patio that spring. The flowers and hanging baskets were breathtaking. It was definitely a heavenly place of rest and tranquility. If I can t be still with God in that environment, I can t be still with Him anywhere, I thought. While Roy was talking on the telephone, I slipped out the backdoor and sat down on my favorite patio chair. I closed my eyes and began to pray, counting my many blessings6.
The anterolateral ligament of the knee is a distinct ligamentous structure about which there is no consensus regarding its function and existence. Some authors deny the existence of such a structure, emphasizing the importance of other anatomical structures, such as the deeper portion of the iliotibial band (ITB) and the anterolateral capsule[3,4]. In contrast, other studies have identified the ALL as a ligament in its own right[5,6]. This disagreement originates from the anatomic dissection techniques that are performed[7,8].
Associated ACL and ALL injury have been shown to significantly increase knee rotational laxity and tibial internal rotation (IR), posing as the background for suboptimal outcomes, potential failure of an isolated ACL reconstruction (ACLR), and secondary meniscal or cartilage injury, as well as for early development of arthritic degeneration[9]. Controlling rotational laxity in ACLR still remains a challenge, with evidence of ALRI persistence in up to 25% of patients regardless of the ACLR technique used[10]. Several studies, in the last years, have identified the ALC as responsible for this residual instability and have pointed at the ALL and the ITB as the main players to internal tibial rotation restrain.
To improve residual rotational instability, more anatomical ACLR techniques have been developed, seeking a more oblique path of the femoral tunnel using the medial portal technique. Recently, the addition of a posterolateral bundle to the anteromedial bundle in double-bundle ACLR has been proposed; however, the technique did not improve rotatory stability and it has now been almost abandoned[11].
HlSTORY
Although there have been sporadic references before 2013 about the existence of a capsuloligamentous structure connecting the femur and tibia in the anterolateral region, descriptions have been vague and often in disagreement. The first reference to the ALL date back more than 100 years. Segond[12], in 1879, described an avulsion fracture of the anterolateral margin of the tibia. He reported a "pearly band extending in an oblique fashion from the femur inserting into the avulsed tibial bone" without elaborating further on the details and anatomical relationships of this structure. However, this finding was ignored until it was rediscovered in a study by Hughston[1] in the 1970s in which they illustrated different patterns of rotational instability. They described a structure, called the "mid-third lateral capsular ligament", that was intimately connected to the lateral meniscus and how it could be involved in rotational instability. This structure, however, was not mentioned again, except sporadically in subsequent studies. In the same year, Johnson[13] described "the anterior oblique band of the lateral collateral ligament." On the other hand, Terry[14] pointed out that the main players in the anterolateral region were the deep, capsulo-osseous and superficial layers of the ITB without making references to distinct structures that could refer to the ALL.
In 2007, Vieira[15] described how the capsulo-osseous layer acts as "an anterolateral ligament". This term was used a few years later by Vincent[16] who identified, during TKA implantation, a ligamentous structure with connections to the distal femur, proximal tibia, and lateral meniscus in the anterolateral region of the knee. Nevertheless, before the study by Claes[2] in 2013 that was the first to provide a detailed description of ALL, this term was used to identify likely different structures and to describe their role in the rotational control.
ANATOMY
In agreement with previous studies, Sonnery-Cottet[40] demonstrated how a section of the ALL did not lead to an increase in tibial IR at 20° of flexion angle but increased it at 90° and also showed that the ITB also participates in rotational control. In a study by Noyes[41], after sectioning of the ALL and the ITB, in agreement with evidence demonstrating a synergistic role of these structures in limiting IR, an increase of 5.1° at 60° of flexion and 6.7° at 90° of flexion has been observed. The latest evidence (in cadaver biomechanical studies) agrees that the ALL possesses an IR stabilizing function only at high degrees of flexion. Only at flexion angles of 60° and 90° a restriction to the IR by the ALL can be observed[42]. These results indicate that the ALL does not own a role in the pivot shift phenomenon that occurs at flexion degrees of 20°-30°[43], and one must therefore look for the ALRI responsible not in a single structure, but in the entire ALC. Terry[14] showed, in a cadaveric study of 82 knees, an anterolateral capsular lesion in 93% of patients with ACL injury and that this damage was significantly correlated with the degree of pivot shift.
Since the femoral insertion points of ALL and FCL are in close relationship, both structures can be described with the term "lateral collateral ligament complex." Likewise, the ALL could be the lateral counterpart of the deep medial collateral ligament[2]. However, some studies, have emphasized how the ALL structure and location can vary[20]. While several authors agree in identifying the tibial insertion, the disagreement about the femoral insertion is of particular interest. This discordance has biomechanical implications: The femoral insertion has been described as anterior and distal to the insertion of the FCL[2] or posterior and proximal with the fibers overlapping the FCL itself[18,21]. It is unclear whether this difference is due to interindividual differences or different dissection techniques.
The huntsmen went in, and then came back and said, In the hollow tree there lies a wonderful animal that we don t know, and we have never seen one like it; its skin is made of a thousand pieces of fur; but it is lying down asleep
In contrast, another model described by Helito[22] shows the existence of 2 distinct bundles: A more superficial one with femoral insertion posterior and proximal to the epicondyle and a deeper one with insertion in the center of the epicondyle. It is also likely that the ALL has an intimate relationship with the ITB, supported by a high association of lesions of the ALL and distal ITB[23].
The ALLR technique with the most clinical data available in the literature is reported by Sonnery-Cottet[10]: They described a combined ACL and ALL reconstruction technique using a 3-strand semitendinosus graft coupled with a free gracilis tendon graft. That resulted in a graft that, therefore, had a quadruple section, used for ACL reconstruction, that continues into a single gracilis strand used for ALL reconstruction. An isometric point near the femoral condyle is identified and drilled with an outside-in technique to serve as both the femoral tunnel for the intra-articular ACL and the femoral attachment for the extra-articular ALL reconstruction. The gracilis strand is then advanced distally into a tibial tunnel with an entry point superolateral to Gerdy's tubercle and then flipped back on itself, resulting in an inverted Y shape. This distal double bundle technique differs from most other ALL reconstruction techniques, which tend to use a free graft and a single tibial fixation point[66,67].
The capsulo-osseous layer has been described by Lobenhoffer[25] as a deep portion of the ITB, an arcuate retrograde fiber tract extending from the intermuscular septum of the femur in the lateral supracondylar region to the Gerdy’s tubercle. This ligament-like unit forms a sling around the posterolateral aspect of the distal femur. More recent studies[26] have confirmed the presence of this layer as a distinct anatomic entity separated from the ALL and have also suggested a synergistic role of these structures in restraining IR.
HlSTOLOGY
The histologic analysis provides evidence of particular interest in demonstrating the existence of the ALL as a distinct ligamentous structure with the presence of dense, well-arranged connective tissue and not as a simple capsular thickening that would have less organized and less cellular tissue[6]. The primary composition is type I collagen (90%) with a fibroblast concentration of 121/min adults and 1631/min fetal preparations[27]. In a study, by Caterine[28], the ALL shows fascicular organization in cross-section and also mechanoreceptors and nerve terminal fibers. Likewise, in anstudy of patients undergoing TKA, it was shown that the structure of ALL, compared to ACL, owned a similar pattern of collagen fibers orientation, nuclei’s form, and a similar cellularity[29]. Furthermore, a clear distinction between ALL and capsule is present since the joint capsule resembles a loose connective tissue. Additionally, the ALL femoral insertion shows a transition from ligamentous tissue to mineralized cartilage and bone; this transition indicates ligamentous tissue[28].
As time moved on my grief and anger at his untimely death began to recede16(,) . I realised that his affirmation of me from his deathbed had filled a gaping17 hole of insecurity I had constantly carried around.
lDENTlFlCATlON OF ALL
Although ALRI must be clinically assessed, there are diagnostic tools that allow visualization of the ALL.
Magnetic resonance imaging
Scientific studies that have investigated anterolateral complex lesions in patients with ACL injuries with magnetic resonance imaging (MRI) often highlight conflicting results with association rates from 40% to 80%[30,31]. These discrepancies may be due to inclusion criteria, in some studies, of patients with chronic ACL injuries.
To visualize more easily a thin structure, such as the ALL, the use of a 3 T MRI with 0.4-mm slice and fat-suppressed acquisition is recommended[28] (Figure 1). In a study by Helito[32], MRIs of patients with acute ACL lesions were analyzed to point out the injured structures that were most frequently associated with an ALL lesion: FCL (= 0.004), popliteal tendon (= 0.005), MCL (= 0.011), anterolateral capsule (= 0.000034), and ITB with an increased correlation with a greater degree of injury (= 0.000021). Tears of the ALL are found in 40% of acute ACL injuries, whereas no association was found with meniscal injuries. There was also no association between ALL injury and partial ACL injury, suggesting that the ALL is torn only in major traumas or that its integrity is a protective factor for ACL[32].
As early as 1990, LET combined with ACLR was shown to reduce graft stress by 43%[77] and combined use is being sought to improve joint kinematics and reduce graft failure rates[78].

A systematic review by Puzzitiello[33] concluded that at least a portion of the ALL is visualizable on MRI in 76-100% of knees, and its possible injury in patients with acute ACL injury is identifiable from 10.8% to 62.5% of cases. Additionally, the level of inter- and intra-observer reliability varies from moderate to almost perfect. A higher prevalence of ALL lesions has been identified in MRI in patients with acute ACL injury and high-grade pivot shift with a positive correlation between pivot shift grade and lesion severity (< 0.013)[34]. The finding of these injury associations helps to delineate how the anterolateral rotational stability of the knee is due to the synergistic work of these structures.
Arthroscopy
Several authors have described the possibility of arthroscopic identification of ALL and have provided step-by-step descriptions[35]. According to Zein[35], it is possible to identify it with a 30° scope through the AL portal. It is necessary to place the limb in a figure of-4-position. In the lateral compartment, the popliteal tendon (PT), popliteal hiatus and synovial bulge anterior to the meniscal bare area are identified. By advancing the arthroscope into the lateral gutter above the synovial bulge, PT, FCL, and ALL can be identified, which run in different planes and directions. Applying an internal rotation, a tensioning of ALL can be observed. It is also possible to identify the meniscotibial attachment of the ALL below the lateral meniscus, anterior to the PT.
BlOMECHANlCS
Regarding the ALL, there is no agreement in the literature regarding its role in knee biomechanics. While in some studies it has been shown that the ALL possesses a stabilizing role in an extension and internal rotation position[36], in a cadaveric study[37], the ALL limits internal rotation only at flexion angles greater than 35°, while providing minimal resistance to anteroposterior translation. However, it must be pointed out that the differences reported in these studies may be due to the dissection techniques adopted. In the study by Rasmussen[36], the ALL was not dissected but all anterolateral structures, from Gerdy's tubercle to the head of the fibula, were sectioned not considering that additional structures of the ALC might affect stabilization. Given that additional evidence points to the ITB as the main restrain to internal rotation[38], having it removed may have overestimated the role of the ALL.
It must be remembered that the ligamentous structures of the knee are unlikely to possess isometric behavior, and the various surgical techniques that seek isometric reconstruction fail to achieve anatomic positioning. Although the geometry of the condyles would make the area through which the transepicondylar axis passes a relatively isometric insertion zone, the roll-glide mechanism of the lateral condyle makes it impossible to find isometric femorotibial connections[39]. Structures, that therefore insert posteriorly to the epicondyle, are strained in extension, whereas anterior structures are strained in flexion.
Out the windows, we drink in the passing scene of cars on nearby highways, of children waving on a crossing, of cattle grazing on a distant hillside, of smoke pouring from a power plant, of row upon row of corn and wheat, of flatlands and valleys, of mountains and rolling hillsides, of city skylines and village halls
According to Claes[2], a distinct anatomical structure connecting the distal femur and proximal tibia can be distinguished on the anterolateral portion of the knee. The structure is entirely extracapsular. The proximal insertion point lies on the prominence of the lateral femoral epicondyle, anterior to the fibular collateral ligament (FCL) insertion and proximal and posterior to the insertion of the popliteus tendon; the distal insertion of the ALL is located posterior to Gerdy's tubercle and anterior to the head of the fibula[17-19]. However, it is possible to recognize more superficial fibers that continue into the lateral intermuscular septum of the thigh and more posterior fibers that are closely connected to the more proximal portion of the FCL[2]. Connections to the body of the lateral meniscus also belong to the ALL, divided into meniscofemoral and meniscotibial portions. The lateral inferior geniculate artery and the vein invariably run between the ALL and the lateral meniscus.
It must be pointed out, however, that this evidence come fromstudies. Since anatomical dissections demonstrate connections between the ALL and ITB by Kaplan fibers, the actual functionmight prove to be different as the ITB might dynamically influence the ALL tension[42]. Zens[44] observed, in a cadaveric study, a progressive increase in the length of the ALL in the passive range of motion from 0° to 90° with an average increase of 0.15% per degree of flexion. They also observed that the greatest change in length (+33.77% ± 9.62%) was observed at 90° flexion in 25° internal rotation.
Through biomechanical studies, the failure of the ALL has also been demonstrated to occur in: Ligamentous tear at the tibial or femoral insertion point, intrasubstance tear, or complete tibial detachment with bone fragment avulsion (Segond fracture)[45].
After performing LETs extensively in the early 1980s, there is now renewed interest in these techniques as combined procedures for ACL reconstruction. These procedures were initially abandoned because of concerns about excessive constraint of the lateral compartment and potential development of osteoarthritis.
In summary, anterolateral soft tissues contribute to rotational stability in ACL-deficient knees, with the deep ITB possibly playing a more important role closer to extension than the ALL, which has a greater control of IR at higher flexion angles.
ALC STlFFNESS
A study by Wytrykowski[50] analyzed the stiffness of the ALL (21 N/mm) and the load at failure (141 N), and also described the load at failure of the gracilis tendon (200.7 N) and ITB (161.1 N). Other biomechanical studies have measured the mean maximum load during pull-to-failure testing of KFs (170 N for DKF and 71.3 N for PKF), and thus, suggest an important role for resistant structures like the ALL[26]. It follows that both LETs and anterolateral ligament reconstructions (ALLRs) with ITB strips and gracilis grafts own sufficient strength for anterolateral procedures.
lNDlCATlONS
The clinical indications for ALLR or LET are not clearly defined, and level one clinical studies are currently lacking. It has not yet been established whether there is significant clinical knee instability that requires correction with an additional procedure.
Currently, the indication to perform an extra articular procedure associated with ACL reconstruction is based on preoperative clinical evaluation and patient characteristics. Radiologic investigation is not routinely used as an objective assessment of ALL stability because relatively small lesions can be easily missed in a setting of more obvious associated injuries. Some authors recommend the routine use of such procedures in all ACL reconstruction[51,52].
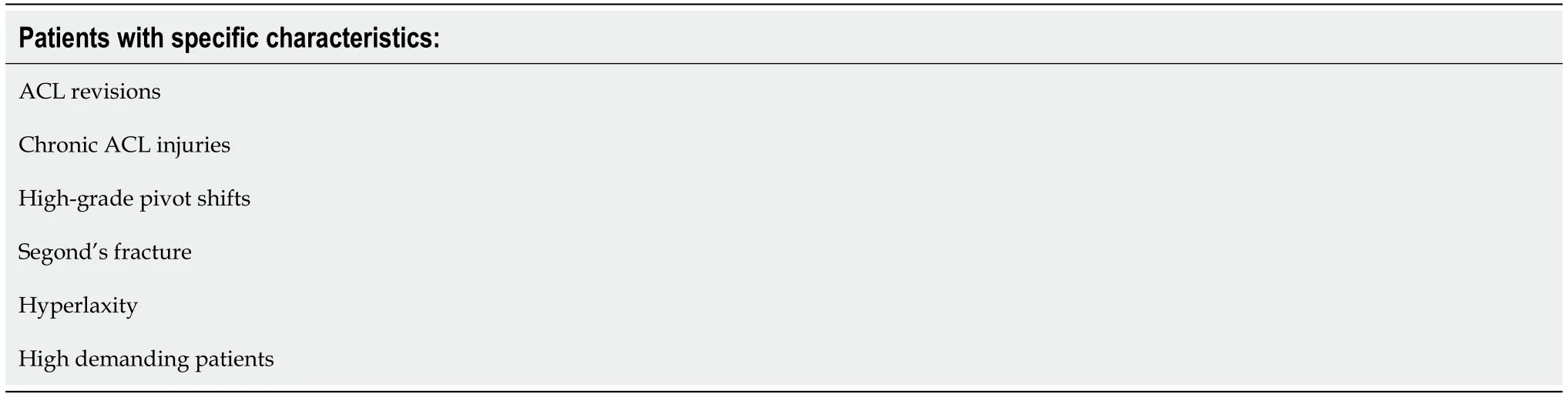
In contrast, other authors recommend an associated procedure only in selected cases[41] based on comparative studies that have demonstrated significant benefits in specific populations, such as: ACL revisions[53,54], chronic ACL injuries[55], patients with high-grade pivot shift[10,56], patients with Segond's fracture[10], patients with hyperlaxity[55], or in high demanding patients with a need to return to high levels of sports activity and pivoting activities[52] (Table 1).
LATERAL EXTRA-ARTlCULAR TENODESlS (LET)
Lateral extra-articular tenodesis was originally used as an isolated technique in patients with ACL deficiency. Several LET techniques showed good clinical results in the short term[57]. However, longterm results highlighted that isolated LETs tended to fail, returning again to a condition of rotatory instability[58].
In contrast, according to a robotic study by Kittl[46], it is the ITB that provides the greatest resistance to tibial IR (44%). The deep fibers of the ITB, Kaplan fibers, act as an IR stabilizing ligament, fixing the ITB against the lateral epicondyle[47]. Indeed, after a section of the KFs, it's been observed that the ITB is no longer attached to the lateral epicondyle, thus losing its effectiveness in rotational control[48]. The role of the KFs was also confirmed by Geeslin[49], demonstrating that sectioning of the KFs resulted in an IR control loss from 30° to 90° of flexion.
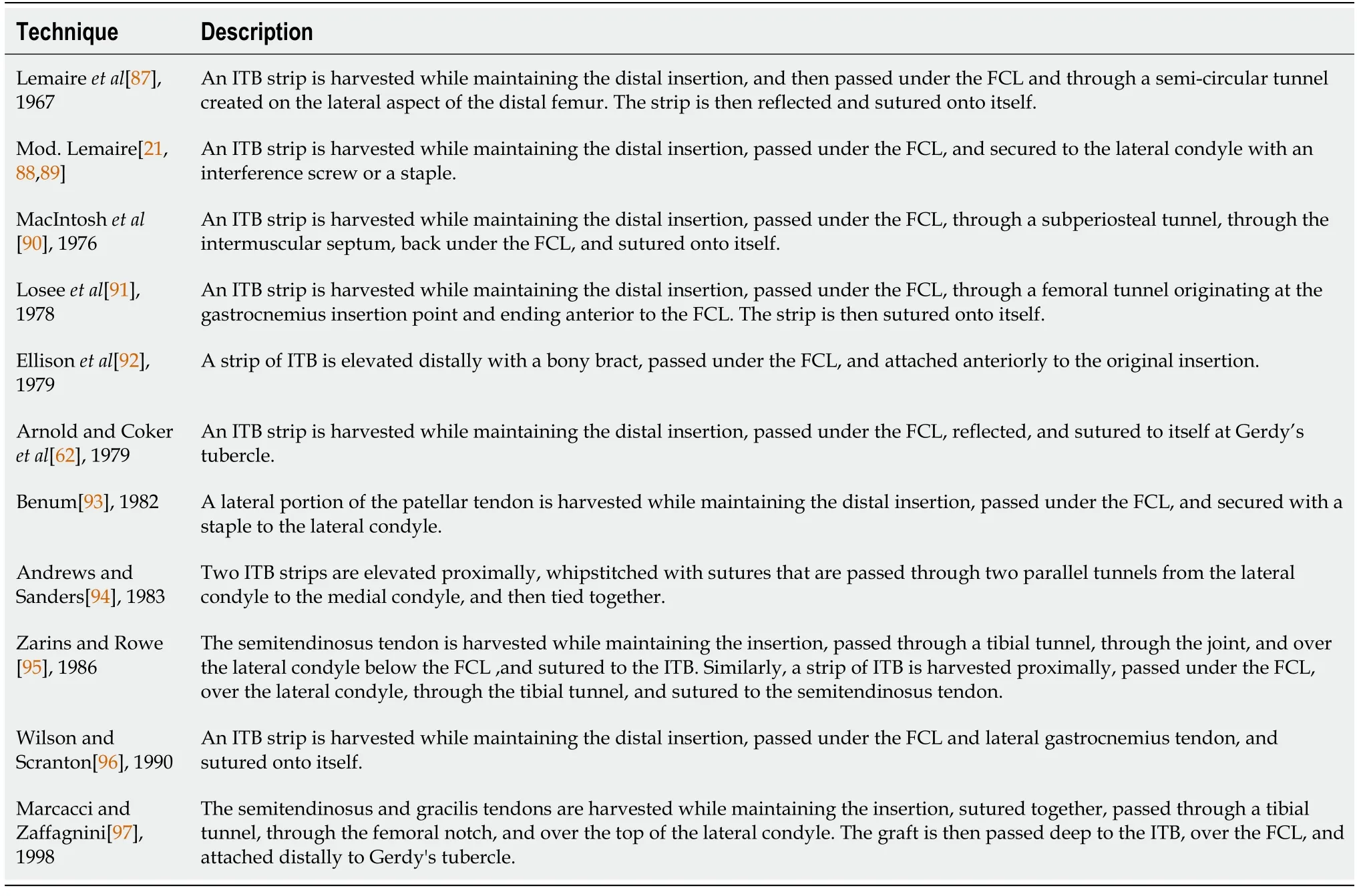
More than 12 LETs (Table 2) have been described, most of which use a variable-length ITB strip passed underneath the FCL and attached at various points on the lateral femoral condyle or at Gerdy's tubercle. The FCL acts as a pulley above the graft while maintaining a relative isometry of the graft itself. However, clinical studies to determine the superiority of one technique over the others are lacking. A correlation can be established on the biomechanical function of KF and LET techniques since both provide a connection between the ITB and the distal femur to control IR.
After this the robbers did not trust themselves in the house again; but it suited the four musicians of Bremen so well that they did not care to leave it any more. And the mouth of him who last told this story is still warm.21
Recently, some authors have described a “more anatomical” extra-articular tenodesis that aims to tension the capsulo-osseous layer and reconstruct the distal KFs[59]. An ITB strip is elevated, maintaining the distal insertion, passed over the FCL, and then fixed into a tunnel drilled at the level of a bony prominence 31.4 mm proximal to the lateral epicondyle (DKF insertion point).
Over the past few years, the authors have tried the use of different LETs and have decided to use mainly the Cocker-Arnold technique. It is a simple technique, easily reproducible, and does not require the preparation of tunnels or the use of suture anchors. The Cocker Arnold technique has proven effective in patients with a preoperative pivot shift 2+ or 3+ at decreasing the phenomenon and reducing the ALRI[60]. Good results were also found in ACLR revisions in high function demand patients with an excellent return to sport rate[61].
The day flew and before I knew it I was at a basketball court at midnight watching him shoot hoops()with friends. After anyone would make a basket he would come over and kiss me. I realized that he was very into me so I pulled him from the game to sit with me at a picnic table; nearby but reasonably private.
Cocker Arnold Mod. Technique[62]
A longitudinal, 10-cm, slightly curved incision is made just posterior to the lateral femoral epicondyle. Dissection continues by identifying the posterior margin of the ITB and removing any fascial attachments down to the level of Gerdy's tubercle. A 1-cm-wide, 8 to 10-cm-long strip of ITB is elevated from the anterior aspect of the posterior half of the ITB. The insertion of the ITB strip to Gerdy's tubercle is preserved, removing any deep attachments of the strip from the vastus lateralis. Identification of the FCL is performed by palpation, facilitated by placing the knee in a figure-of-4 position, which stretches the ligament. Once the FCL has been identified, a blunt dissection is made anteriorly and posteriorly to the proximal portion of the ligament. Efforts should be made to remain extracapsular in order not to damage the popliteal tendon. The ITB graft is then guided under the FCL from distal to proximal, flipped over the Gerdy’s tubercule, and sutured to itself using a high resistance non adsorbable suture, with the knee in near full extension and neutral rotation (Figure 2).

ANTEROLATERAL LlGAMENT RECONSTRUCTlON
Combining an ALLR reduces IR compared to isolated ACLR while having no significant effect on anterior translation. The resulting decrease in IR is more pronounced by increasing the degree of flexion. Specifically, applying a torque of 6 N/m decreased internal rotation of 1.64° (< 0.001) in patients undergoing ACLR + ALLR compared to patients undergoing isolated ACLR[79].
Several studies have shown that isometry of the graft used in ALLRs is achieved by fixing it distal to Gerdy's tubercle and very proximal and posterior to the distal metaepiphyseal junction of the femur[63]. However, this positioning does not match the anatomic insertions of the ALL. The ALL is an anisometric structure: the length and tension of the ligament changes with knee flexion. The best compromise[64,65] between the anatomic reconstruction and the ideal location of the graft insertions is as follows: At the femur, fixation proximal and posterior to the lateral epicondyle; at the tibia, fixation midway between Gerdy's tubercle and the ALL insertion. Fixation should also be done with the knee extended and the foot in neutral rotation. It is critical not to tension the graft in external rotation to avoid stiffening the knee and increasing stress.
So Tsarevitch Ivan took his place in the garden, and sat down to watch under the apple tree that bore the golden apples. He watched an hour, he watched two hours, he watched three hours. When midnight drew near sleep al most overcame him, but he drew his dagger5 and pricked6 his thigh7 with its point till the pain aroused him. And suddenly, an hour after midnight, the garden became bright as if with the light of many fires, and the Fire Bird came flying on its golden wings to alight on the lowest bough8 of the apple tree.
The latest evidence emphasizes that the control of the ALRI is due to the entire anterolateral complex. The ALC works together with the ACL to restrain internal tibial rotation. The ALC consists of the ALL, the superficial and deep portion of the ITB, the capsulo-osseous layer, and the anterolateral capsule. Indeed, the deep part of the ITB and its complex insertion points at the distal femur contribute significantly to rotational control. Kaplan's fibers (KFs) play a role, along with the ITB, as a secondary passive stabilizer after the ACL[24]. They are described as a deep, posterior portion of the ITB connected to distal femur, divided into two bundles, the proximal fibers (PKF) and the distal fibers (DKF).
ALLR VS LET
Biomechanical studies explain that LET procedures have an advantageous lever arm in resisting IR compared to ALLR techniques. This is due to the more anterior point of fixation at Gerdy's tubercle, which provides a more efficient force vector[68].
Since a major concern lies in the overconstraint of the lateral compartment[69], several studies have been concerned with analyzing the effectiveness of different techniques at different degrees of tension[70]. The authors verified the optimal graft tension by applying different fixation tensions. The results show that a modified Lemaire tenodesis (in which an ITB strip is elevated, passed under the FCL, and fixed to the distal femur with a suture anchor) can restore proper knee kinematics with a tension of 20 N regardless of the degree of flexion (0°, 30°, and 60°) while maintaining the foot in neutral rotation. An ALL-anatomical reconstruction, on the other hand, cannot sufficiently reduce rotational laxity even at 40 N tension. According to the research of Inderhaug[71], a double-bundle ALLR (with one femoral attachment point and two distinct tibial attachment point) procedure can restore rotatory laxity when the graft is fixed in full extension. However, it has been reported that flexion-extension of the knee leads to the detensioning of one of the 2 bundles, and therefore the use of a stronger single bundle, has been recommended.
Long-term effects on articular cartilage wear in outcomes of LET or ALLR procedures do not yet have high levels of evidence[72]; however, it makes sense to opt for effective procedures at lower levels of tension in order not to increase the contact pressure of the articular surfaces. In a study by Marcacci[52], in which patients who underwent ACLR and LET were prospectively followed for up to 13 years, there was no evidence of increased arthritic degeneration when comparing patients who underwent ACLR alone.
Previous studies recommended fixation of the graft (in LET procedures) by maintaining the tibia in an external rotation position. However, more recent studies recommend fixing the graft while keeping the tibia in a neutral rotation position so as not to inhibit physiologic rotational motion[73]. Since anterolateral structures are thought to affect ALRI, it is reasonable to assume that fixation while keeping the knee in extension (at a flexion angle where pivot shift occurs) is favorable for seeking normal knee kinematics[71]. Additionally, the ALL or LET graft is stretched and fixed after ACL graft fixation to minimize the overconstraint.
Regarding the choice of graft, both an ITB strip and a gracilis graft own sufficient strength to vicariate the function of the ALL. In a study by Kittl[64], patterns of change in length and isometry in lateral extra-articular reconstructions were analyzed. Of the variables examined, only two effectively and reproducibly predicted a relative isometric graft behavior in different degrees of flexion: a graft path below the FCL and a femoral graft fixation proximal and posterior to the lateral epicondyle. In a biomechanical study, it was shown that an anatomic reconstruction of the ALL did not significantly reduce IR or anterior translation. In contrast, a LET procedure significantly improved anterior translation and rotational laxity[21].
Then the reindeer jumped for joy; and the little robber-girl lifted Gerda on his back, and had the forethought to tie her on, and even to give her her own little cushion to sit on.
I was willing to give him that pleasure, but I was afraid that he wouldn t be able to find the way here by himself, so I made myself ready to go with him
Severalbiomechanical studies have attempted to quantify the efficacy of LET procedures. However, it is difficult to reach objective conclusions of superiority and durability given the large variability in different surgical techniques, graft selection, and type of fixation.
RESULTS
The indication for performing an anterolateral procedure is based on the concept of reducing stress forces on the ACL graft and more accurately restoring normal knee kinematics[74]. Improved knee stability results in a protective effect of the ACL graft and on the menisci[75]. These biomechanical advantages translate into clinical benefits, including reduced risk of ACL graft rupture, higher rates of return to previous sports physical activity, and lower risk of meniscal repair failure[76].
I remember some ten years ago when he was made a King s Counsel, Amos and I, seeing him get off the London train, went to congratulate him. We grinned with pleasure; he merely looked as miserable as though he d received a penal6 sentence. It was the same when he was knighted; he never smiled a bit, he didn t even bother to celebrate with a round of drinks at the Blue Fox . He took his success as a child does his medicine. And not one of his achievements brought even a ghost of a smile to his tired eyes.
The concepts of ALLR and LET are sometimes used synonymously, since these procedures share conceptual similarities in terms of technique and goals. However, in ALLRs an anatomical reconstruction of the ALL is sought, while in LETs a functional and not an anatomical reconstruction is performed.
Historically, several ACL reconstruction techniques have been proposed to restore rotational instability. Isolated ACL reconstructions, whether single or double bundle, have failed in the attempt by resulting in a residual rotational laxity. In a study by Monaco[51], it was demonstrated "" that the combination of a LET with a single-bundle ACLR procedure was significantly more effective than an isolated double-bundle technique (= 0.0001) in reducing tibial IR.
In a study with 2-year follow-up in 502 patients[80], it was shown that the combination of ACLR (with hamstring graft) and ALLR had a 2.5-fold lower rate of ACL graft failure than isolated ACLR with BTPB and 3.1-fold lower rate than isolated ACLR with hamstring graft.
In a recent study by Sonnery-Cottet[81], it was shown at an average follow-up of 104 mo that patients undergoing ACLR combined with ALLR experienced significantly better ACL graft survival (= 0.0027), lower overall revision rates (< 0.05), lower ACLR revision rates (< 0.05), and comparable complication rates to patients undergoing isolated ACLR. Overall, patients undergoing isolated ACLR had a 5-fold increased risk of ACL revision.
Regarding the concern of developing osteoarthritis in patients undergoing ALLR, there are two possible opposing scenarios to consider. The first factor relates to a possible overconstraint of the lateral compartment resulting in increased contact forces. The second factor, in contrast, concerns the possible residual rotational instability in case an ALLR is not performed, resulting in poor tibial rotation control and the consequent risk of secondary meniscal and chondral injuries. Several studies, however, state that there is no association between ALLR and early development of osteoarthritis compared with patients undergoing isolated ACLR[52,82]. In a multicenter study with 675 patients at 12 years of follow-up[83], there was no evidence of an association between ALLR and arthritic degeneration, which was instead reported mainly in cases of medial meniscectomy.
And now the King s son had it carried away by his servants on their shoulders. And it happened that they stumbled over a tree-stump28, and with the shock the poisonous piece of apple which Snow-white had bitten off came out of her throat. And before long she opened her eyes, lifted up the lid of the coffin, sat up, and was once more alive. Oh, heavens, where am I? she cried. The King s son, full of joy, said, You are with me, and told her what had happened, and said, I love you more than everything in the world; come with me to my father s palace, you shall be my wife.
Recent literature states that, in agreement with biomechanical studies, associating an anterolateral procedure significantly improves a high-grade pivot shift, ensuring better clinical functional outcomes[84,85]. Additionally, subjective scores, such as IKDC and Lysholm and objective tests, such as the KT-1000, are also significantly better (< 0.05) in patients who underwent a combined procedure[86].
ACTUAL LlMlTS AND FUTURE PERSPECTlVES
A more complete and comprehensive understanding of ALC has encouraged surgeons to perform combined reconstructions to improve clinical results and long-term outcomes. It should be noted, however, that the heterogeneity of the techniques used in the studies examined cannot provide valid data and results for each anterolateral procedure. Although recent studies have shown the efficacy and safety of these techniques[80,81], randomized clinical trials and level one studies are required to analyze the superiority of a LET or ALLR technique over the others in terms of ALRI reduction and total revision rate.
CONCLUSlON
From the latest evidence, it appears that it is not a single anterolateral structure that determines rotational stability, but rather that several structures act synergistically: the ALL, the superficial and deep layers of the ITB, the capsulo-osseous layer, and the Kaplan fibers. Regardless of the distinct structures that are injured and cause an ALRI, the authors consider it important to obtain a careful clinical evaluation of the patient, repeated just before the surgical procedure under anesthesia. In a scenario where there is no demonstrated superiority of one technique over the others, the authors opted to use the Cocker Arnold Modified Tenodesis as a combined procedure in ACLR deciding to perform it according to […] patient's characteristics (such as a high-grade pivot shift, hyperlaxity, Segond’s fracture) and functional demands. They also use it in any revision surgery where there has been a previous ACL graft failure in order to reduce the ACL graft stress and the risk rate of a new failure.
FOOTNOTES
Sabatini L provided the input in writing the paper; Risitano S, Drocco L, and Capella M collected the literature review; Vezza D, Barberis L, and Camazzola D wrote the paper; Massè A coordinated the writing of the paper.
All authors report no relevant conflict of interest for this article.
On the fifth day his messenger returned with a letter to say that the king of the land of the north would not sell, but he would give, the king the slave girl and her son
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Italy
Luigi Sabatini 0000-0003-4956-1303; Marcello Capella 0000-0002-6076-8527; Daniele Vezza 0000-0002-9710-402X; Luca Barberis 0000-0001-5994-2471; Daniele Camazzola 0000-0001-9701-1889; Salvatore Risitano 0000-0003-4595-1531; Luca Drocco 0000-0002-4982-9106; Alessandro Massè 0000-0003-3999-4121.
Wu YXJ
Filipodia
Miraculously4 he managed to reach his friend, hoisted5() him onto his shoulder, and brought him back to their company s trench. As the two of them tumbled in together to the bottom of the trench, the officer checked the wounded soldier, then looked kindly6 at his friend. I told you it wouldn t be worth it, he said. Your friend is dead, and you are mortally wounded.
Wu YXJ
杂志排行

World Journal of Orthopedics的其它文章
- Rates of readmission and reoperation after operative management of midshaft clavicle fractures in adolescents
- Bilateral hip heterotopic ossification with sciatic nerve compression on a paediatric patient-An individualized surgical approach: A case report
- Quantitative alpha-defensin testing: ls synovial fluid dilution important?
- Effect of pelvic fixation on ambulation in children with neuromuscular scoliosis
- Epidemiology of pelvic and acetabular fractures across 12-mo at a level-1 trauma centre
- Risk modeling of femoral neck fracture based on geometric parameters of the proximal epiphysis