Angiotensin converting enzyme inhibitor associated spontaneous herniation of liver mimicking a pleural mass: A case report
2022-07-02SameerSaleemTebhaZainAliZaidiSehrishSetharMuhammadAsifAbbasVirkMuhammadNadeemYousaf
Sameer Saleem Tebha, Zain Ali Zaidi, Sehrish Sethar, Muhammad Asif Abbas Virk, Muhammad Nadeem Yousaf
Sameer Saleem Tebha, Department of Neurosurgery and Neurology, Jinnah Medical and Dental College, Karachi 75600, Sindh, Pakistan
Zain Ali Zaidi, Department of Medicine, Jinnah Medical and Dental College, Karachi 75600, Sindh, Pakistan
Sehrish Sethar, Department of Radiology, Jinnah Medical and Dental College, Karachi 75600, Sindh, Pakistan
Muhammad Asif Abbas Virk, Department of Medicine, Division of Gastroenterology, Well Span York Hospital, York, PA 17403, United States
Muhammad Nadeem Yousaf, Department of Medicine, Division of Gastroenterology and Hepatology, University of Missouri, Columbia, MO 65212, United States
Abstract BACKGROUND Spontaneous diaphragmatic herniation of the liver is a rare entity. It may mimic pulmonary mass especially in the absence of trauma. Cough is a common side effect of angiotensin converting enzyme (ACE) inhibitors that may cause diaphragmatic rupture due to a sudden increase in trans-diaphragmatic pressure. We present a case of ACE-inhibitor associated spontaneous herniation of the liver mimicking pleural mass.CASE SUMMARY An 80-year-old woman presented with dry cough for 1 mo and sudden onset of cramping abdominal pain for 1 d. She denied history of trauma, prior surgeries, smoking, alcohol or illicit drug use. She has a history of diabetes and was started on an ACE inhibitor 6 mo ago for the management of hypertension. Examination was remarkable for right upper quadrant tenderness. Lab work-up was unremarkable. Chest X-ray showed a right lower lung opacity suspecting right pleural mass. Chest computed tomography scan ruled out pleural mass, however, revealed herniated right lobe of the liver (3.9 cm × 3.6 cm × 3.4 cm) into the thoracic cavity through the posterolateral diaphragmatic defect. Laparoscopic repair of the diaphragmatic defect was performed and the ACE inhibitor was stopped. Patients’ symptoms had completely resolved on follow-up.CONCLUSION ACE inhibitor-associated cough may cause diaphragmatic liver herniation mimicking pleural mass. Early diagnosis, surgical repair and addressing the triggering factors improve patients’ outcomes.
Key Words: Diaphragmatic hernia; Liver herniation; ACE-inhibitors; Cough; Non-traumatic diaphragmatic hernia; Case report
INTRODUCTION
Spontaneous diaphragmatic herniation of abdominal organs into the thoracic cavity is an uncommon entity. A congenital defect in the diaphragm is the most common cause of diaphragmatic hernia with a reported incidence of 0.8-5 per 10000 births[1]. Acquired rupture of the diaphragm is most commonly caused by high-velocity blunt or penetration abdomino-thoracic trauma and postsurgical diaphragmatic defect that may result in herniation of abdominal contents into the thoracic cavity[2,3]. Spontaneous diaphragmatic herniation is an uncommon subtype of acquired hernia without history of trauma. Commonly herniated abdominal organs are the stomach, small or large intestines, mesentery and spleen[2,4,5]. Spontaneous herniation of the liver into the thoracic cavity due to a non-traumatic rupture of the diaphragm is unusual with only a few cases reported[4,6,7].
Clinical presentation of diaphragmatic hernias are variable depending upon the acuity of diaphragmatic rupture, size of the defect and underlying etiology. Majority of patients present with abdominal pain, chest pain, tachycardia, shortness of breath and cough, however, a subset of patients remain asymptomatic in cases of a small defect in the diaphragm[8]. Diaphragmatic liver herniation may mimic pleural malignancy. A high index of clinical suspicion is required for early identification of diaphragmatic hernias and differentiating them from pleural malignancy with a careful review of crosssectional radiological imaging of chest and abdomen. We present a case of cough induced spontaneous diaphragmatic herniation of the liver due to the use of angiotensin converting enzyme (ACE) inhibitor.
CASE PRESENTATION
Chief complaints
An 80-year-old female presented for evaluation of dry cough for 4 wk.
History of present illness
Patient’s cough was severe, persistent, without associated hemoptysis or sputum production. She also reported the sudden onset of upper abdominal pain and mild shortness of breath for 1 d prior to visiting the hospital.
History of past illness
She had past medical history of diabetes mellitus and hypertension and was started on an ACE inhibitor 6 mo ago for the management of hypertension. She denied history of previous surgery or recent trauma.
Personal and family history
Family history was unremarkable.
Physical examination
On examination, the patient was afebrile (98.6 F), tachycardiac (112/min) with an elevated blood pressure (140/80 mmHg) and respiratory rate of 20 breaths/minute. Abdominal examination was remarkable for mild right upper quadrant tenderness without evidence of Murphy’s sign or skin bruising. The lower border of the liver was non-palpable; however, a percussion dullness was noted at the right fourth intercostal space of the chest in the midclavicular line. The patient was admitted for further evaluation.
Laboratory examinations
Her baseline blood work including complete blood count, liver function tests and basic metabolic panel were unremarkable except for low hemoglobin and hematocrit (Table 1).

Table 1 Baseline lab investigations
Imaging examinations
Ultrasound of the abdomen showed normal echotexture of the liver without evidence of liver lesions, cholelithiasis, acute cholecystitis or hepatobiliary ductal dilation. Chest radiograph demonstrated a well-defined soft tissue mass noted just above the right hemidiaphragm making an obtuse angle suggesting pleural or extra-pleural mass (Figure 1). Given a suspicion of pleural malignancy, a highresolution computed tomography (CT)-scan of the chest was performed which revealed a defect in the posterolateral aspect of the right diaphragm with a herniated right lobe of the liver into the thoracic cavity representing a mass measuring 3.9 cm × 3.6 cm × 3.4 cm (Figure 2).
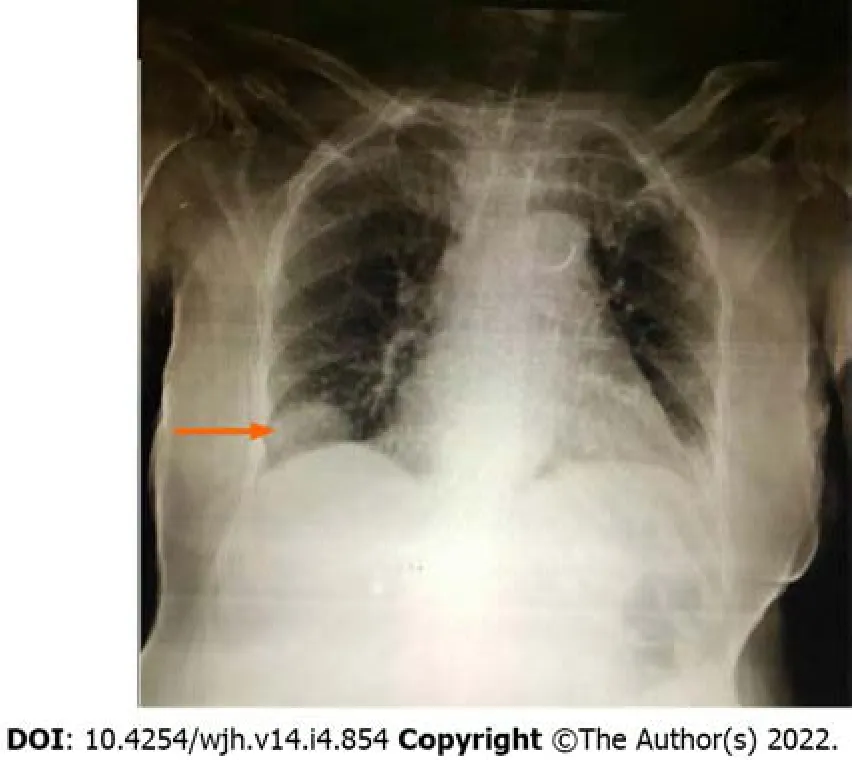
Figure 1 Chest radiograph demonstrates a well-defined soft tissue mass noted just above the right hemi-diaphragm making an obtuse costophrenic angle suggesting pleural or extra-pleural mass.
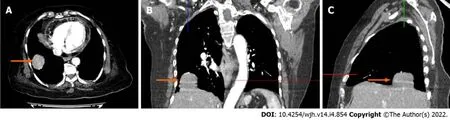
Figure 2 Chest computed tomography images. A: Axial view showing herniated part of the liver through focal defect in the right hemi-diaphragm (arrow) mimicking a pleural/pulmonary mass; B: Coronal view shows extension of liver parenchyma into the thoracic cavity with hepatic artery within herniated liver (arrow); C: Sagittal view shows nubbin of liver parenchyma herniated through diaphragmatic defect posteriorly (arrow).
FINAL DIAGNOSIS
Spontaneous liver herniation through the right diaphragm due to an ACE inhibitor associated cough.
TREATMENT
Laparoscopic surgical repair of the diaphragmatic defect was performed after the retraction of herniated liver into the abdominal cavity. The post-surgical hospital course was uneventful. Patient was discharged on day 3 of hospitalization. Her ACE inhibitor was switched to a calcium channel blocker (verapamil) for the management of hypertension.
OUTCOME AND FOLLOW-UP
At the 8-wk follow-up, the patients’ symptoms were completely resolved and blood pressure was well controlled on Verapamil.
DISCUSSION
This case illustrates an unusual presentation of spontaneous diaphragmatic herniation of the liver secondary to ACE inhibitor associated cough. ACE inhibitors are common medications used for the management of hypertension and congestive heart failure. Approximately 5%-35% of patients develop ACE inhibitor associated dry cough with a reported onset within hours to months after initiation of therapy[9-11]. Coughing causes an opposing force on the diaphragm due to respiratory muscle discoordination. Abdominal muscle contraction causes an upward pushing force on the diaphragm against the downward and inward movement of the ribs[12]. Sustained cough increases the transdiaphragmatic pressure gradient that may cause trivial injury to the diaphragm. This phenomenon may result in spontaneous herniation of abdominal organs into the thoracic cavity through diaphragmatic defects.
Our patient had an ACE inhibitor associated cough that caused a sudden increase in transdiaphragmatic pressure and induced liver herniation through a diaphragmatic defect. The herniated liver closely mimicked a pleural mass leading to a diagnosis of suspected malignancy particularly in the setting of new onset of cough and shortness of breath. Our case was initially misdiagnosed as a pleural malignancy due to the rarity of the finding and confusing it with other causes of pulmonary origin. Investigation with chest CT scan ruled out pleural malignancy and revealed diaphragmatic defect with liver herniation. Patakaet al[13] presented a similar case of liver herniation which mimicked lung malignancy due to the gastrointestinal reflux associated with sustained cough.
The sensitivity of chest radiography to differentiate diaphragmatic liver herniation from the pulmonary mass is only 17% in right sided and 46% on left sided diaphragmatic defects[14]. Helical CT scan of the chest and abdomen is the radiological imaging of choice with a 73% sensitivity and a 90% specificity in the identification of diaphragmatic defects, herniated abdominal organs and differentiating them from pulmonary mass[15]. Small diaphragmatic defects may be difficult to locate on CT scan. In these cases, magnetic resonance imaging, diagnostic thoracoscopy or laparoscopy may assist in the identification of diaphragmatic defects and in the planning of surgical repair[8]. Surgical reduction of herniated abdominal contents and repair of the diaphragmatic defect is the treatment of choice. Laparoscopic and/or thoracoscopic repair is preferred over open laparotomy or thoracostomy because of less risk of morbidity and mortality with these minimally invasive modalities[8].
CONCLUSION
Spontaneous diaphragmatic herniation of the liver may mimic a pleural/pulmonary mass. A high index of clinical suspicion is required for early identification of non-traumatic diaphragmatic liver herniation particularly in individuals at risk of the increased transabdominal pressure gradient. ACE inhibitor associated cough is a known adverse reaction that rarely results in liver herniation. Early diagnosis with cross-sectional radiological imaging, surgical repair and addressing triggering factors improves patient outcome.
FOOTNOTES
Author contributions:Sethar S identified the abnormality and diagnosed the patient; Tebha SS and Zaidi ZA reviewed the literature, found relevant information, and wrote the manuscript; Virk MAA and Yousaf MN proofread, revisions and edits of the manuscript, and overall supervision in finalizing of the manuscript.
Informed consent statement:Informed consent was acquired from the patient before writing and publishing this case report and all accompanying images.
Conflict-of-interest statement:All the authors declare that there is no conflict of interest.
CARE Checklist (2016) statement:The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:United States
ORCID number:Sameer Saleem Tebha 0000-0001-8480-6148; Zain Ali Zaidi 0000-0001-5973-5827; Sehrish Sethar 0000-0003-2094-3594; Muhammad Asif Abbas Virk 0000-0002-8724-8775; Muhammad Nadeem Yousaf 0000-0002-7979-8929.
S-Editor:Liu JH
L-Editor:Filipodia
P-Editor:Liu JH
杂志排行

World Journal of Hepatology的其它文章
- Revolution in the diagnosis and management of hepatitis C virus infection in current era
- Evidence-based approach to management of hepatic encephalopathy in adults
- Direct oral anticoagulant administration in cirrhotic patients with portal vein thrombosis: What is the evidence?
- Noninvasive diagnosis of periportal fibrosis in schistosomiasis mansoni: A comprehensive review
- Review on hepatitis B virus precore/core promoter mutations and their correlation with genotypes and liver disease severity
- Assessment of periportal fibrosis in Schistosomiasis mansoni patients by proton nuclear magnetic resonance-based metabonomics models