Late polymicrobial transjugular intrahepatic portosystemic shunt infection in a liver transplant patient: A case report
2022-07-02IreneDeLaCaridadPerezZivHaskalJohnHoganCurtisArgo
Irene De La Caridad Perez, Ziv J Haskal, John I Hogan, Curtis K Argo
Irene De La Caridad Perez, Department of Medicine, University of Virginia Medical Center, Charlottesville, VA 22903, United States
Ziv J Haskal, Department of Radiology and Medical Imaging, Division of Vascular and Interventional Radiology, University of Virginia Medical Center, Charlottesville, VA 22903, United States
John I Hogan, Department of Medicine, Division of Infectious Diseases and International Health, University of Virginia Medical Center, Charlottesville, VA 22903, United States
Curtis K Argo, Department of Medicine, Division of Gastroenterology and Hepatology, University of Virginia Medical Center, Charlottesville, VA 22903, United States
Abstract BACKGROUND Infection of a transjugular intrahepatic portosystemic shunt (TIPS) stent is a rare and serious complication that most commonly occurs during TIPS creation and revision. Patients typically present with recurrent bacteremia due to shunt occlusion or vegetation. To date there are approximately 58 cases reported. We present a patient diagnosed with late polymicrobial TIPS infection five years following TIPS creation.CASE SUMMARY A 63-year-old female status-post liver transplant with recurrent cirrhosis and portal hypertension presented with sepsis and recurrent extended-spectrum betalactamase Escherichia coli bacteremia. Computed tomography of the abdomen revealed an occluded TIPS with thrombus extension into the distal right portal vein, and focal thickening of the cecum and ascending colon. Colonoscopy revealed patchy ulcers in these areas with histopathology demonstrating ulcerated colonic mucosa with fibrinopurulent exudate. Shunt thrombectomy and revision revealed infected-appearing thrombus. Patient initially cleared her infection with antibacterial therapy and TIPS revision; however, soon after, she developed Enterobacter cloacae bacteremia and Candida glabrata and C. albicans fungemia with recurrent TIPS thrombosis. She remained on antifungal therapy indefinitely and later developed vancomycin-resistant Enterococcus faecium with recurrent TIPS thrombosis. The option of liver re-transplant for removal of the infected TIPS was not offered given her critical illness and complex shunt anatomy. The patient became intolerant to linezolid and elected hospice care.CONCLUSION Clinicians should be aware that TIPS superinfection may occur as long as five years following TIPS creation in an immunocompromised patient.
Key Words: Transjugular intrahepatic portosystemic shunt; Endotipsitis; Colitis; Liver cirrhosis; Liver transplantation; Case report
INTRODUCTION
Transjugular intrahepatic portosystemic shunt (TIPS) creation is a routine therapy for patients with complications of portal hypertension such as refractory ascites or variceal hemorrhage[1]. Endotipsitis is a rare endovascular infection of a TIPS with a prevalence of approximately 1% and mortality rate of approximately 32%[2-4]. A rare but challenging complication of endotipsitis is persistent bacteremia following TIPS creation and revision. Early cases of TIPS infection, categorized as an infection within 120 days of TIPS creation, are commonly associated with gram-positive bacteria[4]. In the USA the use of prophylactic antibiotics prior to TIPS creation is routinely practiced, and according to the American Society of Interventional Radiology is considered a class IIB recommendation[2,5]. However, there are strict indications based on the guidelines by the British Society of Gastroenterology, which strongly recommend prophylactic antibiotics only for TIPS shunt for variceal bleeding, long/complex procedures, or in a patient with a previous biliary surgery or instrumentation[6].
TIPS stent colonization is believed to be secondary to lack of graft endothelization with the highest mortality rates associated withStaphylococcusandCandidaspecies[2-4,7]. These microorganisms are difficult to treat given their ability to form biofilms, as can be seen in other endovascular infections such as prosthetic valve endocarditis[7,8]. Tacrolimus, a immunosuppressive medication prescribed to this patient, has been associated with decreased epithelization in animal andin vivostudies and therefore may further increase the risk of TIPS stent colonization in a patient[9,10]. This case report presents a rare event of polymicrobial TIPS infection occurring five years following TIPS creation in an immunosuppressed patient status post liver transplantation for hepatitis C cirrhosis. Additionally, polymicrobial endotipsitis cases were identified through PubMed to provide an updated overview of treatment courses and associated health outcomes.
CASE PRESENTATION
Chief complaints
A 63-year-old female presented with sepsis and recurrent extended-spectrum beta-lactamaseEscherichia coli(E. coli) bacteremia.
History of present illness
Our patient initially presented to her local hospital with hypotension and sepsis in late August 2019 and completed a 10-d course of ertapenem while hospitalized forE. colibacteremia. She presented locally with similar symptoms a few days after discharge from the initial admission and was found to have recurrentE. colibacteremia with the identical susceptibility pattern. Imaging demonstrated TIPS occlusion, and the patient was transferred to our institution with recurrentE. colibacteremia from an unidentified source.
History of past illness
Our patient with a MELD-Na score of 23 underwent orthotopic liver transplantation in 2009 for hepatitis C cirrhosis. Her transplant course was complicated by recurrent hepatitis C infection resulting in bridging fibrosis/early cirrhosis despite viral eradication in 2011. She eventually developed portal hypertension related to a non-occlusive portal vein thrombosis and anastomotic stenosis of the hepatic vein and inferior vena cava. In 2014, she suffered acute gastric variceal bleeding and underwent semiurgent treatment with balloon-occluded anterograde obliteration of a gastrorenal shunt and TIPS creation with a self-expanding poly-tetrafluoroethylene (ePTFE)-covered stent-graft.
Personal and family history
Medical history included hepatitis C, gastric varices, hypertension, well-controlled diabetes mellitus type 2, iron deficiency anemia and fibromyalgia. Family history included hypertension, lung cancer, and prostate cancer.
Physical examination
The patient was afebrile and displayed right upper abdominal tenderness.
Laboratory examinations
Laboratory findings included hemoglobin 8.6 (12-16 g/dL) (baseline of approximately 9-10), white blood cell (WBC) 5.39 (4-11 × 103/µL), platelets 89 (150-450 × 103/µL), alanine transferase 16 (< 55 U/L), aspartate transferase 19 (< 35 U/L), total bilirubin 0.5 (0.3-1.2 mg/dL), alkaline phosphatase 88 (40-150 U/L) and creatinine 1.2 (0.7-1.3 mg/dL). Gastrointestinal pathogens panel polymerase chain reaction was negative for enteroaggregativeE. coli, enteropathogenicE. coli, enterotoxigenicE. coli, shiga-like toxin-producingE. coli,E. coliO157, and shigella/enteroinvasiveE. coli.Histopathology of cecum and ascending colon biopsies obtained a few days prior revealed extensive ulcerated colonic mucosa with fibrinopurulent exudates, consistent with active colitis. There was no evidence of cytomegalovirus associated inclusion bodies, microorganisms, granulomas, or malignancy. Bacterial culture of the extracted thrombus (Figure 1) during thrombectomy did not grow any organisms. Urine analysis showed no bacteria and rare white blood cells per high power field with no growth on culture.

Figure 1 Transjugular intrahepatic portosystemic shunt thrombectomy. Thrombus extracted during first transjugular intrahepatic portosystemic shunt thrombectomy was notable for size and infected appearance.
Imaging examinations
Thickening of the cecum and ascending colon, and TIPS occlusion that extended into the distal right portal vein were noted on abdominal computed tomography (CT) (Figure 2A). Magnetic resonance imaging did not show significant hepatic biliary dilatation or biliary leak. Chest CT suggested multiple pulmonary septic emboli. Transthoracic echocardiography (TTE) obtained a few days prior showed mild reduced systolic ejection fraction and no obvious vegetations, though aortic, tricuspid, and pulmonic valves were not well visualized due to restricted patient mobility and excessive abdominal air.
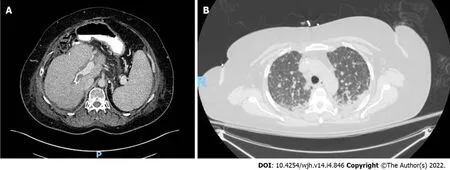
Figure 2 Computed tomography images. A: Computed tomography of upper abdomen. An axial-contrast enhanced computed tomography of the upper abdomen showing an occluded (hypodense area) transjugular intrahepatic portosystemic shunt; B: Computed tomography of chest. An axial non-enhanced computed tomography of the chest showing diffuse bilateral ground-glass and interstitial opacities with innumerable bilateral pulmonary nodules and small bilateral pleural effusions.
FINAL DIAGNOSIS
The patient was diagnosed with a late TIPS infection.
TREATMENT
She underwent TIPS thrombectomy, venoplasty, and placement of a new Wallstent coaxial uncovered metallic stent at the portal end of the TIPS to extend the intraportal leading end of the shunt into a larger caliber portal vein, as the originally entered portal vein was small in caliber and formed an inflow narrowing into the TIPS at the leading edge of the PTFE-coated self-expanding stent. Anticoagulation after TIPS revision was not considered in this patient as she did not have a primary hypercoagulable disorder, and the flow in the shunt was brisk and was rendered clean by thrombectomy and clot extraction. She was discharged on a 6-wk course of IV ertapenem (1 g once daily). Patient successfully cleared herE. colibacteremia.
OUTCOME AND FOLLOW-UP
Two and a half months later, our patient presented with a headache and was treated forEnterobacter cloacaeandCandida glabratasepticemia. Vital signs were notable for fever (38.2℃) and tachycardia (114 bpm). Labs included hemoglobin 9.2 g/dL, WBC 4.34 × 103/µL, platelets 70 × 103/µL, alanine transferase < 6 U/L, aspartate transferase 33 U/L, and creatinine 0.9 mg/dL. Abdominal CT showed a new non-occlusive thrombus in the mid-TIPS and a right ovarian vein clot. Repeat shunt thrombectomy and revision was performed. Histopathology of the extracted thrombus confirmedCandidaspecies, andC. glabrataandC. albicansgrew in blood cultures. Additional infectious workup included a TTE that was non-revealing. A 6-wk course of IV ertapenem (1 g once daily) and IV micafungin (150 mg daily) was initiated at discharge.
Four weeks later she developed acute dyspnea and pleuritic chest pain and was readmitted with hypoxemic respiratory failure. TTE revealed grade 1 diastolic dysfunction without vegetation. Chest CT revealed numerous bilateral pulmonary nodules with diffuse ground-glass and interstitial opacities (Figure 2B). Blood cultures once again grewC. glabrataandC. albicans, and bronchoalveolar lavage grewCandidaspecies. Given suspicion for refractory intravascular Candida infection, therapy was escalated to IV amphotericin (300 mg daily) and oral flucytosine (1000 mg twice a day). Balloon sweep of the TIPS was complicated by post-procedural shock and hypoxemia. In the setting of progressive acute kidney injury and pancytopenia, the patient was transitioned to IV micafungin (150 mg daily) and IV voriconazole (400 mg twice daily for one day followed by 300 mg twice daily). Due to the combination of respiratory failure, active infection, and location of the TIPS that extended into the base of the right atrium, re-transplantation (and removal of the TIPS) was not offered due to exceedingly high surgical risk. She remained on antifungal therapy indefinitely and over the subsequent three months developed recurrent vancomycin-resistantEnterococcus faeciumbacteremia. Newly identified thrombus along a peripherally inserted central catheter suggested the possibility of line associated septic thrombophlebitis as the source of herEnterococcusbacteremia. Bacteremia recrudesced despite line extraction, eventual resolution of her line associated clot, and an appropriate course of proactively dosed IV daptomycin (400-915 mg daily). Repeat TTE did not reveal signs of infective endocarditis and CT confirmed recurrent TIPS thrombosis as the likely source of her refractoryEnterococcus faeciumbacteremia that progressed to develop a daptomycin minimum inhibitory concentration > 256. Although the patient improved clinically and initially cleared her bacteremia with IV linezolid (600 mg daily), she developed severe thrombocytopenia and gastrointestinal bleeding that precluded further use of this agent. The patient elected to pursue hospice care and died shortly thereafter.
DISCUSSION
This case is a unique account of polymicrobial TIPS stent infection occurring five years after TIPS creation, the longest interval reported[4]. Shunt infection is most commonly reported during TIPS creation or revision, and infrequently with biliary-shunt fistulae that may form following TIPS creation[11]. Our patient presented with recurrentE. colibacteremia of unclear origin and ongoing active colitis. While it is possible that bacterial translocation into the portal vein blood in the setting of active colitis could lead toE. colibacteremia and seeding of the TIPS, it seems more likely that the colitis and occlusion of the TIPS occurred as a result of a low-flow state with seeding of the occlusive TIPS thrombus during ongoingE. colibacteremia. Evidence that supports colitis likely being ischemic during the second episode ofE. colibacteremia include the colonic biopsy results obtained during lower endoscopy that corresponded to areas of active colitis noted on CT imaging which did not show any microorganisms based on limited histopathological analysis (no gram staining performed). Alternative common sources ofE. colibacteremia were investigated during her second episode of bacteremia, including urinary infection, biliary leak, cholangitis, and bacterial gastroenteritis, and work-up was nonrevealing. Moreover, there was a very low suspicion for infective endocarditis given the respective organism involved and no history of IV drug use. This was confirmed on multiple TTEs which did not show any vegetation. In summary, the initial source of infection that may have seeded the TIPS was not clearly identified -- bacterial translocation due to confirmed, active colitis is a plausible explanation but an alternate source such as genitourinary or biliary are also possible given that records do not indicate a source of the initialE. colibacteremia. It is important to note that during this patient’s firstE. colibacteremia episode diagnostic imaging was delayed. Imaging was pursued during her second episode ofE. colibacteremia as the patient complained of right upper quadrant pain and this revealed an occluded TIPS that raised suspicion for endotipsitis. This patient continued to suffer from recurrent polymicrobial bacteremia and fungemia after multiple TIPS revisions likely from a chronically infected TIPS. The patient likely had incomplete stent endothelization given the use of tacrolimus, which increased her risk of stent colonization[9,10].
Determining treatment duration and whether liver transplantation should be considered in the clinical scenario of endotipsitis are challenging decisions. Available clinical care guidance derives from case reports and case series, hence underscoring the importance of reporting new cases. To date there are 59 cases[2,4,12-14] of TIPS stent infection with nine being polymicrobial (Tables 1 and 2)[15-19]. Initial treatment courses range from 2 to 6 wk of antimicrobial therapy, followed by long-term oral therapy and orthotopic liver transplantation when medical therapy fails (Table 2). Analysis of polymicrobial cases to date showed that infections resolved with liver transplantation (Table 2). If patients did not undergo transplantation they remained indefinitely on antifungal therapy. While TIPS thrombectomy and revision were not commonly undertaken, there should be consideration of early thrombectomy, as drug penetration and source control may be insufficient with only antimicrobial therapy. For instance, inadequate drug penetration has been noted with amphotericin forCandidainfective endocarditis[7]. Hence, surgical intervention is recommended for left sided infective endocarditis involving fungal organisms, as well as forS. aureus, or other highly resistant organisms[15]. Considering the high mortality rate of fungal TIPS infections[14,20-24], approximately 60% (Table 1), it is unclear whether antifungal prophylaxis should be considered prior to a TIPS revision. Justification for this step is lacking due to paucity of prospective studies (not surprising given the rarity of this infection) and the absence of guidelines to identify high-risk patients.

Table 1 Mortality rates associated with monomicrobial and polymicrobial endotipsitis

Table 2 Polymicrobial cases of endotipsitis
In summary, we present a case of recurrentE. colibacteremia due to a late TIPS infection and occlusion that later evolved to a polymicrobial, multidrug-resistant TIPS infection. The patient initially cleared her infection with antimicrobial therapy and TIPS thrombectomy. Unfortunately, the patient later developed recurrent polymicrobial bacteremia and fungemia from a chronically infected TIPS.
CONCLUSION
TIPS infection is a rare event that most commonly occurs following TIPS creation and revision, though as illustrated in this case report it may occur many years following TIPS creation. Clinicians should be aware of this clinical complication early in the course so a TIPS thrombectomy can be performed for source control and to improve antibiotic penetration of the TIPS. Moreover, literature review shows that the highest mortality rates with endotipsitis are withCandidaand polymicrobial infections. Given the refractory nature of these infections, liver transplantation should be considered to provide definitive treatment when feasible. Lastly, the rarity of a TIPS infection limits the development of research studies, and current understanding of this entity relies mainly on case reports and case series, hence highlighting the need to continue to report new cases.
FOOTNOTES
Author contributions:Perez IDLC was the internal medicine resident physician providing care during initial hospitalization; Perez IDLC also drafted and participated in the revision process and final submission of this manuscript; Haskal ZJ was the interventional radiologist that performed the procedures described in this case and participated in the whole revision process; Hogan JI was the infectious disease specialist overseeing her care and participated in the whole revision process; Argo CK was the outpatient and inpatient hepatologist who provided specialized care, participated in the revision process and final submission of this manuscript.
Informed consent statement:Consent was obtained verbally over the phone from the husband as the patient passed away.
Conflict-of-interest statement:Dr. Haskal disclosures include working with Varian, Boston Scientific, WL Gore and Associates, and Becton Dickinson. All other authors have no actual or potential conflicting interest in the submission of this manuscript.
CARE Checklist (2016) statement:The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: http://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:United States
ORCID number:Irene De La Caridad Perez 0000-0001-5873-5673; Ziv J Haskal 0000-0002-1469-3691; John I Hogan 0000-0001-9581-9753; Curtis K Argo 0000-0003-4262-6274.
Corresponding Author's Membership in Professional Societies:American Association for the Study of Liver Diseases; American College of Gastroenterology.
S-Editor:Liu JH
L-Editor:A
P-Editor:Liu JH
杂志排行

World Journal of Hepatology的其它文章
- Revolution in the diagnosis and management of hepatitis C virus infection in current era
- Evidence-based approach to management of hepatic encephalopathy in adults
- Direct oral anticoagulant administration in cirrhotic patients with portal vein thrombosis: What is the evidence?
- Noninvasive diagnosis of periportal fibrosis in schistosomiasis mansoni: A comprehensive review
- Review on hepatitis B virus precore/core promoter mutations and their correlation with genotypes and liver disease severity
- Assessment of periportal fibrosis in Schistosomiasis mansoni patients by proton nuclear magnetic resonance-based metabonomics models