Total cholesterol to high-density lipoprotein ratio and nonalcoholic fatty liver disease in a population with chronic hepatitis B
2022-07-02YuGeZhouNingTianWeiNingXie
Yu-Ge Zhou, Ning Tian, Wei-Ning Xie
Yu-Ge Zhou, Affiliated Guangdong Hospital of Integrated Traditional Chinese and Western Medicine, Guangzhou University of Chinese Medicine, Foshan 528200, Guangdong Province, China
Ning Tian, Preventive Healthcare Center, Guangdong Provincial Hospital of Integrated Traditional Chinese and Western Medicine, Foshan 528200, Guangdong Province, China
Wei-Ning Xie, Department of Scientific Research, Guangdong Provincial Hospital of Integrated Traditional Chinese and Western Medicine, Foshan 528200, Guangdong Province, China
Abstract BACKGROUND Nonalcoholic fatty liver disease (NAFLD) is characterized by hypertriglyceridemia, increased low-density lipoprotein cholesterol levels, and reduced highdensity lipoprotein cholesterol (HDL-C) particles. Previous studies have shown that the total cholesterol to high-density lipoprotein cholesterol ratio (TC/HDL-C) was superior to other lipid metabolism biomarkers for predicting NAFLD risk and could be a new indicator of NAFLD. However, the association between TC/HDL-C and NAFLD in patients with hepatitis B virus (HBV) has not yet been determined.AIM To investigate the association between TC/HDL-C and NAFLD in a population with chronic hepatitis B (CHB).METHODS In this study, 183 HBV-infected patients were enrolled. All participants underwent blood chemistry examinations and abdominal ultrasound. Univariate and multivariate logistic regression models, curve fitting analysis, and threshold calculation were used to assess the relationship between TC/HDL-C and NAFLD.RESULTS The overall prevalence of NAFLD was 17.49% (n = 32) in the 183 CHB participants. The TC/HDL-C of non-NAFLD and NAFLD patients were 3.83 ± 0.75 and 4.44 ± 0.77, respectively (P < 0.01). Logistic regression analysis showed that TC/HDL-C was not associated with NAFLD after adjusting for other pertinent clinical variables. However, at an optimal cutoff point of 4.9, a non-linear correlation between TC/HDL-C and NAFLD was detected. The effect size of the left and right sides of the inflection point were 5.4 (95% confidence interval: 2.3-12.6, P < 0.01) and 0.5 (95% confidence interval: 0.1-2.2, P = 0.39), respectively. On the left side of the inflection point, TC/HDL-C was positively associated with NAFLD. However, no significant association was observed on the right side of the inflection point.CONCLUSION This study demonstrated a non-linear correlation between TC/HDL-C and NAFLD in a population with CHB. TC/HDL-C was positively associated with NAFLD when TC/HDL-C was less than 4.9 but not when TC/HDL-C was more than 4.9.
Key Words: Cholesterol; Lipoprotein cholesterol ratio; Nonalcoholic fatty liver disease; Chronic hepatitis B population; Correlation
INTRODUCTION
Chronic hepatitis B (CHB) is a common disease threatening public health and is a leading cause of multitudinous liver-related morbidity and mortality[1]. In 2016, about 257 million people were affected by hepatitis B virus (HBV) infection worldwide, with an estimated prevalence of 3.5%[2]. Over the past decades, with the implementation of nucleoside analogs (NAs) and hepatitis B vaccine, the risk of liver cirrhosis complications and hepatocellular carcinoma (HCC) have been substantially reduced in CHB patients[3]. However, since approximately 25% of the CHB population with nonalcoholic fatty liver disease (NAFLD) have hepatic steatosis, the effects of CHB on hepatosteatosis have recently been garnering attention[4].
NAFLD is a common chronic hepatic disease worldwide that is closely associated with cardiovascular disease, metabolic disorders, and end-stage liver diseases such as cirrhosis and HCC[5]. The prevalence of NAFLD has been increasing, and in the past few years it has reached alarming proportions (29.1%) in China due to changes in lifestyle habits and rapid socio-economic growth[6]; therefore, increased awareness to recognize NAFLD as a chronic liver disease is urgently needed.
Due to the growing prevalence of NAFLD, the coexistence of HBV infection and NAFLD is commonly observed around the world. However, a clear association between these two diseases remains questionable. Previous studies indicated that NAFLD could be inversely associated with the levels of HBV seromarkers[7,8], but interestingly, there is substantial evidence indicating an association between HBV infection and reduced incidence of hyperlipidemia or NAFLD[9,10].
Alterations in lipid metabolism are central drivers of disease progression, for instance, the progression of hepatic steatosis to nonalcoholic steatohepatitis (NASH) and hepatic fibrosis[11]. Therefore, deciphering the lipid metabolism characteristic of NAFLD is the crucial for disease treatment and prevention. NAFLD is characterized by hypertriglyceridemia, increased low-density lipoprotein cholesterol (LDL-C) levels, and reduced high-density lipoprotein cholesterol (HDL-C) particles[12,13]. A recent study showed that the total cholesterol to high-density lipoprotein cholesterol ratio (TC/HDL-C) was better at predicting NAFLD risk than other markers such as total cholesterol (TC), HDL-C, and the ratio of apolipoprotein B (ApoB) to apolipoprotein A1 (ApoA1) and might be a new indicator of NAFLD[14]. However, the association between TC/HDL-C and NAFLD in an HBV-infected population has not yet been investigated. Therefore, the objective of this study was to assess the correlation between TC/HDL-C and NAFLD in a population with CHB.
MATERIALS AND METHODS
Study population and criteria
This was a retrospective, observational study comprising of HBV-infected patients who were treated at the Integrated Traditional Chinese and Western Medicine Hospital of Foshan (Guangdong, China) from January 2019 to December 2020. The study flow chart is illustrated in Figure 1. Chronic HBV infection was defined by hepatitis B surface antigen (HBsAg) positive for more than 6 mo[1]. All participants underwent abdominal ultrasonography for NAFLD and blood tests for assessing lipid metabolism and hepatic and renal function. Each participant completed a detailed questionnaire concerning information on their sex, age, alcohol consumption history, disease history, and medication history. Patients were excluded if they had (1) a daily alcohol intake ≥ 30g (for men) or 20 g (for women); (2) history of cancer; (3) history of chronic renal insufficiency; (4) history of hepatobiliary surgery; and (5) missing data on the key clinical variables required for study analysis.

Figure 1 Flow chart of participant selection. NAFLD: Nonalcoholic fatty liver disease.
Laboratory investigations
Blood samples were collected from all patients after an overnight fasting of at least 8 h. Peripheral venous blood was drawn from their cubital vein. Blood test parameters, including aspartate aminotransferase (AST), alanine aminotransferase (ALT), γ-glutamyl transpeptidase (γ-GT), creatinine (CRE), uric acid (UA), triglyceride (TG), TC, HDL-C, LDL-C, ApoA1, and ApoB, were measured using an Olympus AU-640 autoanalyzer (Olympus, Tokyo, Japan). Platelets (PLT) were measured using the Sysmex 2100 whole blood cell analyzer (Sysmex, Kobe, Japan). Hepatitis B serum examinations included the detection of HBV-DNA level, HBsAg, and hepatitis B e antigen (HBeAg) using polymerase chain reaction. HBV-DNA(+) was defined as a level of serum HBV-DNA over 100 IU/mL. TC/HDL-C was defined as TC divided by HDL-C. The patient's height and weight were measured while wearing light clothing without shoes. Body mass index (BMI) was calculated by dividing a person’s weight in kilograms by the square of their height in meters. Abdominal ultrasound was used to detect the presence of NAFLD. NAs therapy was defined as the use of oral NAs antiviral drugs for more than 3 mo. All the above data were obtained from the Clinical Laboratory of the Guangdong Provincial Hospital of Integrated Traditional Chinese and Western Medicine.
Ethics and consent
The research project was submitted to and approved by the Ethics Committee of Guangdong Provincial Hospital of Integrated Traditional Chinese and Western Medicine (Approval number: 2018-1254). No informed consent was required because this was a retrospective observational study.
Definition of NAFLD based on abdominal ultrasonography
Ultrasonography was the most commonly used examination for fatty liver screening due to its noninvasiveness, low cost, and easy operability[15]. Abdominal ultrasonography was performed on all enrollees by two trained ultrasound physicians using the ACUSON X150 ultrasound system (Siemens, Munich, Germany). The presence of at least two of the following criteria was required for considering fatty liver: (1) More than 5% of hepatocytes had excessive hepatic fat accumulation and steatosis[16]; (2) Diffuse echo enhancement of the liver relative to the kidney; (3) Occurrence of ultrasonic beam attenuation; and (4) Poor visualization of intrahepatic structures. After excluding alcohol abuse and other hepatic diseases, NAFLD was then formally diagnosed by abdominal ultrasonography[17].
Statistical analysis
All statistical analyses were conducted using SPSS (version 23.0, IBM, Armonk, NY, United States) and EmpowerStats (http://www.empowerstats.com, X&Y solutions, Inc. Boston, MA, United States) software. Normal distribution continuous variables are expressed as mean ± standard deviation, andttest was used for group comparison. Non-normal distribution variables are described as median [interquartile range (IQR)], and the Mann-WhitneyUtest was used to compare the groups. Categorical variables were presented as their corresponding number and percentage (n, %) and compared using the chi-squared test. All enrollees were stratified into two groups based on the presence or absence of NAFLD on ultrasonography. Then, the demographic characteristics of the study participants of the two groups were assessed. Univariate analyses of all variables were conducted using a binary logistic regression analysis model. Based on their TC/HDL-C, the patients were also divided into three groups according to TC/HDL-C tertiles: TC/HDL-C ≤ 3.5, 3.5 < TC/HDL-C ≤ 5, and TC/HDL-C > 5. Multivariable models were constructed as follows: Model 1 was not adjusted for other pertinent clinical variables; Model 2 was adjusted for sex and age; Model 3 was adjusted for sex, age, BMI, AST, ALT, γ-GT, PLT, HBsAg, CRE, UA, TG, TC, HDL-C, LDL-C, ApoA1, ApoB, HBV-DNA (+), HBeAg(+), and NAs. Lastly, a non-linear relationship between TC/HDL-C and NAFLD was investigated, and smooth curve fitting was also used.Pvalues (two-tailed) less than 0.05 were considered statistically significant.
RESULTS
Demographic characteristics
The demographic characteristics of the study participants with and without NAFLD are shown in Table 1. In the whole study population, the overall prevalence of NAFLD was 17.49% (n= 32). A total of 183 patients (70.5% males) were included in this study. Their mean age was 45.41 ± 11.59 years, and their average BMI was 23.14 ± 2.63 kg/m2. The TC/HDL-C of the non-NAFLD and NAFLD groups were 3.83 ± 0.75 and 4.44 ± 0.77, respectively (P< 0.01). Compared with the non-NAFLD group, patients from the NAFLD group had higher levels of BMI, ALT, γ-GT, PLT, UA, TG, TC, LDL-C, ApoB, and TC/HDLC (P< 0.05). Conversely, age, HBV-DNA (+) levels, and usage of NAs were significantly lower in the NAFLD group than in the non-NAFLD group (P< 0.01). However, there was no statistically significant difference between the two groups in terms of sex and levels of AST, HBsAg, CRE, HDL-C, ApoA1, and HBeAg (+) (P> 0.05).

Table 1 Demographic characteristics of the study participants with and without nonalcoholic fatty liver disease
Univariate analysis
Binary logistic regression of independent risk factors of NAFLD is shown in Table 2. Univariate analysis indicated that age, BMI, ALT, γ-GT, PLT, UA, TG, LDL-C, ApoB, TC/HDL-C, and HBV-DNA (+) were significantly positively correlated with NAFLD (P< 0.05), whereas age and NAs were negatively correlated with NAFLD. However, no significant association between NAFLD and sex, AST, HBsAg, CRE, TC, HDL-C, ApoA1, and HBeAg(+) were observed (P> 0.05).

Table 2 Binary logistic regression of independent risk factors of nonalcoholic fatty liver disease
Association between TC/HDL-C and NAFLD using logistic regression model
Logistic regression model was used to evaluate the association between TC/HDL-C and NAFLD. The unadjusted and adjusted models are shown in Table 3. In model 1, TC/HDL-C was positively correlated with NAFLD [odds ratio (OR) = 0.94, 95% confidence interval (CI): 1.55-4.19,P< 0.01). In model 2 (adjusted for sex and age), the relationship between TC/HDL-C and NAFLD were significant (OR = 0.96, 95%CI: 1.52-4.51,P< 0.01). However, this association was not detected in model 3 (OR = -2.27, 95%CI: 0.0001-79.91,P= 0.50). The same trend was observed for TC/HDL-C from 3.5 to 5 in model 1 and model 2 (P< 0.05).

Table 3 Correlation between cholesterol to high-density lipoprotein cholesterol and nonalcoholic fatty liver disease in different models
Analysis of non-linear relationships between TC/HDL-C and NAFLD
Since TC/HDL-C was a continuous variable, we analyzed the non-linear relationship with NAFLD. After adjusting for all variables and conducting smooth curve fitting, we found that the relationship between TC/HDL-C and NAFLD was non-linear (Figure 2). The inflection point was calculated as 4.9 by a piecewise linear regression model. On the left side of the inflection point, TC/HDL-C was found to be positively correlated with NAFLD (β = 5.4, 95%CI: 2.3-12.6,P< 0.01). However, no significant correlation was observed between TC/HDL-C and NAFLD on the right side of the inflection point (β = 0.5 95%CI: 0.1-2.2,P =0.39) (Table 4).
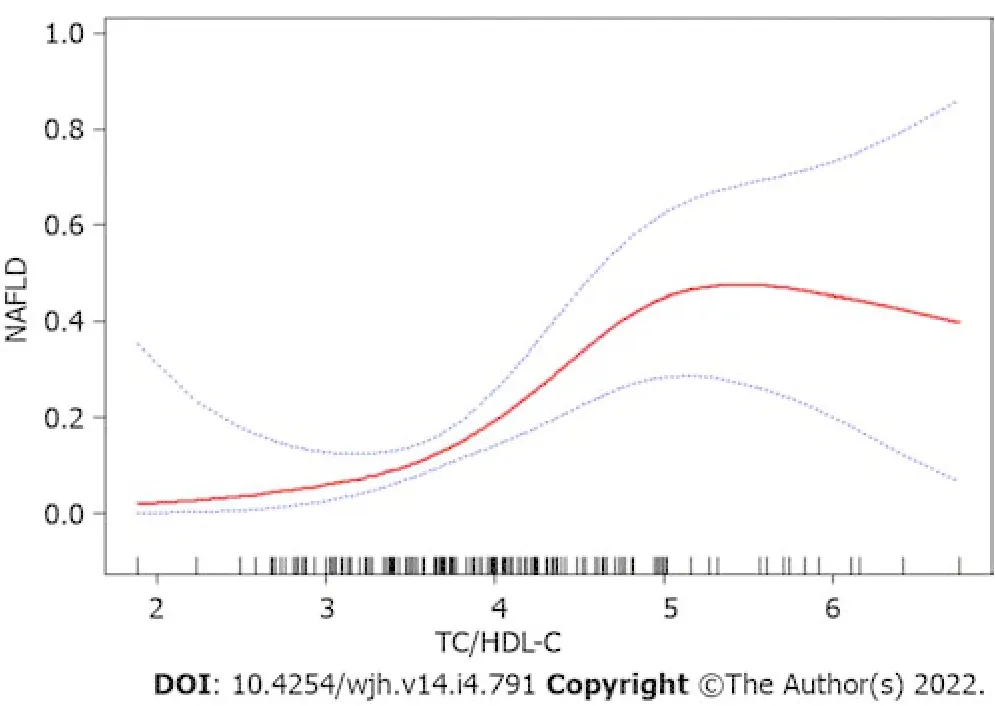
Figure 2 Relationship between total cholesterol to high-density lipoprotein cholesterol ratio and nonalcoholic fatty liver disease by smooth curve fitting. Adjustment variables: Sex, age, body mass index, aminotransferase, aminotransferase, γ-glutamyl transpeptidase, platelets, hepatitis B surface antigen, creatinine, uric acid, triglyceride, total cholesterol, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, apolipoprotein A1, apolipoprotein B, hepatitis B virus DNA (+), Hepatitis B e antigen (+), nucleoside analogs. TC/HDL-C: Total cholesterol to high-density lipoprotein cholesterol ratio; NAFLD: Nonalcoholic fatty liver disease.

Table 4 The independent correlation between cholesterol to high-density lipoprotein cholesterol and nonalcoholic fatty liver disease by multivariate piecewise linear regression
DISCUSSION
In epidemiologic studies, the highest incidences of NAFLD were reported in the Middle East (32%) and South America (31%), followed by Asia (27%) and the United States (24%)[18]. However, in a study involving 810 northern Japanese children, the prevalence of fatty liver was observed to be only 2.6% based on ultrasonographic criteria[19], but the prevalence of NAFLD was increased to 77% among obese children[20]. In our previous study, we found that the incidence rate of NAFLD in the general population was 35.92%[21]. The above studies only focused on the prevalence of NAFLD in the general population. In this present study, the overall prevalence of NAFLD in the investigated CHB population was 17.49%. Consistent with our findings, previous studies indicated that the prevalence of NAFLD with and without HBsAg positivity was 14.3% and 28.6%, respectively (P< 0.01)[22]. A prior study observed a low incidence of NAFLD in their investigated CHB population and hypothesized that such could be mainly because HBV infection influences the secretion of a variety of adipokines and alterations in lipid profiles[23].
Substantial evidence indicated an association between HBV infection and reduced incidence of hyperlipidemia or NAFLD risk[9,10]. In a large cross-sectional study, the researchers observed that HBsAg-positive subjects had a significantly lower risk of NAFLD (OR = 0.42)[22]. Adiponectin may be central to this observed association. Adipokine may attenuate hepatic steatosis and the degree of its decline was shown to correlate with the severity of NAFLD[24]. Moreover, adiponectin levels were also shown to be positively correlated with HBV-DNA viral load in CHB patients[24,25].
However, the cross-talk between CHB and NAFLD remained controversial. There are studies indicating that NAFLD was inversely associated with the levels of HBV seromarkers[7,8]. In this present study, the proportion of HBV-DNA positivity in the NAFLD group (n= 15, 46.9%) was significantly lower than that in the non-NAFLD group (n= 116, 76.8%). Further, a large cohort study demonstrated that HBsAg clearance was significantly higher in CHB patients with hepatic steatosis than in those without[26], and these results were in agreement with animal experiments[27,28].
In regards to treatment, long-term oral use of NAs drugs such as entecavir and tenofovir were the main anti-HBV treatment as they are simple and safe to use, which is recognized all over the world[1]. Thus, oral NAs therapy alone was the first option for patients with CHB. However, CHB patients with NAFLD needed additional treatment besides antiviral drugs. Lifestyle intervention was a basic method for losing weight. For severe cases, pharmacological treatment was required to regulate the patients’ lipid metabolism disorders[29].
Metabolic alterations in NAFLD may directly or indirectly affect the HBV-DNA levels of CHB patients[30]. Due to the common immune pathways of NAFLD and CHB, NAFLD-related metabolic stress may activate the suppressed innate immunity to restore the production of antiviral substances, which ultimately accelerates the clearance of HBV-DNA and HBsAg[31,32].
Metabolic syndrome is a highly prevalent concern in patients with NAFLD[17,33]. The typical characteristics of NAFLD are abnormal lipid accumulation in hepatocytes, hypertriglyceridemia, increased LDL-C levels, and reduced HDL-C particles. Metabolic perturbations promote liver injury and inflammation, which can lead to increased risk for hepatic fibrosis[34]. A cohort study of Chinese people with normal lipid metabolism indicated that a low-density lipoprotein to high-density lipoprotein (LDL/HDL) ratio was superior to other lipoproteins in identifying people at risk of NAFLD[35]. Studies from the Framingham Cardiovascular Institute also showed that a ratio of TC/HDL-C greater than 4 was a major risk factor for cardiovascular thrombosis[36]. In this present study, our results showed that TG, TC, LDL-C, ApoB, and TC/HDL-C had a significant increment in CHB patients combined with NAFLD. Concordant with the results of previous studies, we observed that although the levels of HDLC and ApoA1 were decreased, no significant statistical difference was observed[12].
In our study, TC/HDL-C was a positive risk factor for NAFLD (P< 0.01) in univariate analysis. Previous studies suggested that there was a linear relationship between TC/HDL-C and NAFLD in the general population[14]. However, in this study, curve fitting analysis model showed that the association between TC/HDL-C and NAFLD was non-linear in the CHB population for an inflection point of 4.9. Thus, we speculated that TC/HDL-C was positively associated with NAFLD when the ratio of TC/HDL-C was less than 4.9 in the CHB population.
There were some limitations observed in this study. First, the investigated population was relatively small and therefore, large-scale studies are needed to validate our findings. Second, the assessment of NAFLD was based on hepatic ultrasonography rather than liver biopsy, which was the traditional gold standard for the assessment of NAFLD[37]. Patients could be reluctant to undergo liver biopsy because of its high cost, invasiveness and risk of complications[38]. Furthermore, fibrosis indices such as hyaluronic acid, laminin, procollagen III peptide, collagen type IV, and transient elastography were not included in the analyses due to missing data on fibrosis indices and could have been conducive to evaluating the relationship between NAFLD and different stages of CHB. In future studies, we will assess the relationship between fibrosis indices and TC/HDL-C. Lastly, this cross-sectional study only explored the relationship between the TC/HDL-C and NAFLD and was unable to reveal the causal and effect relationship between them.
CONCLUSION
In conclusion, the study demonstrated that the relationship between TC/HDL-C and NAFLD was nonlinear in the CHB population. TC/HDL-C was positively correlated with NAFLD when TC/HDL-C was less than 4.9, but no such trend could be observed when the ratio of TC/HDL-C was more than 4.9.
ARTICLE HIGHLIGHTS
Research background
Due to the growing prevalence of nonalcoholic fatty liver disease (NAFLD), the coexistence of hepatitis B virus (HBV) infection and NAFLD is commonly observed around the world. However, the cross-talk between these two diseases remained questionable.
Research motivation
Previous studies showed that the total cholesterol to high-density lipoprotein cholesterol ratio(TC/HDL-C) was a better predictor of NAFLD than other lipid metabolism biomarkers and might be a new indicator of NAFLD. However, the association between TC/HDL-C and NAFLD in an HBVinfected population has not been previously investigated.
Research objectives
To investigate the association between TC/HDL-C and NAFLD in a CHB population.
Research methods
Univariate and multivariate logistic regression models, curve fitting analysis and threshold calculations were used to assess the relationship between TC/HDL-C and NAFLD.
Research results
A non-linear association was detected between TC/HDL-C and NAFLD in the CHB population at an inflection point of 4.9. The effect size on the left and right sides of inflection point were 5.4 (95%CI: 2.3-12.6, P < 0.01) and 0.5 (95%CI: 0.1-2.2, P = 0.39), respectively.
Research conclusions
In the CHB population, the relationship between TC/HDL-C and NAFLD was non-linear. TC/HDL-C was positively correlated with NAFLD when TC/HDL-C was less than 4.9.
Research perspectives
Further large-scale cohort studies are needed to validate whether TC/HDL-C is indeed a better predictor of NAFLD than other lipid metabolism biomarkers in the CHB population.
ACKNOWLEDGEMENTS
The authors appreciate all participants for their contribution to this study and the laboratory staff of the Guangdong Provincial Hospital of Integrated Traditional Chinese and Western Medicine.
FOOTNOTES
Author contributions:Xie WN designed the study, constructed the research ideas and interpreted the data; Zhou YG participated in the acquisition and analysis of the data and drafted the initial manuscript; Tian N supervised the project process and revised the article critically for important intellectual content.
Institutional review board statement:This research project was submitted to and approved by the Ethics Committee of Guangdong Provincial Hospital of Integrated Traditional Chinese and Western Medicine (Approval number: 2018-1254).
Informed consent statement:No informed consent was required because this was a retrospective observational study.
Conflict-of-interest statement:There were no conflicts of interest to report.
Data sharing statement:No additional data was available.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Yu-Ge Zhou 0000-0002-1687-5552; Ning Tian 0000-0002-3971-9245; Wei-Ning Xie 0000-0001-8377-4391.
S-Editor:Ma YJ
L-Editor:Filipodia
P-Editor:Ma YJ
杂志排行

World Journal of Hepatology的其它文章
- Revolution in the diagnosis and management of hepatitis C virus infection in current era
- Evidence-based approach to management of hepatic encephalopathy in adults
- Direct oral anticoagulant administration in cirrhotic patients with portal vein thrombosis: What is the evidence?
- Noninvasive diagnosis of periportal fibrosis in schistosomiasis mansoni: A comprehensive review
- Review on hepatitis B virus precore/core promoter mutations and their correlation with genotypes and liver disease severity
- Assessment of periportal fibrosis in Schistosomiasis mansoni patients by proton nuclear magnetic resonance-based metabonomics models