Ball-shaped right atrial mass in renal cell carcinoma: A case report
2022-06-16SohilPothiawalaSavandeSilvaKunzangNorbu
Sohil Pothiawala, Savan deSilva, Kunzang Norbu
Sohil Pothiawala, Department of Emergency Medicine, Woodlands Health, Singapore 768024,Singapore
Savan deSilva, Kunzang Norbu, Department of Emergency Medicine, Sengkang General Hospital, Singapore 544886, Singapore
Abstract BACKGROUND Renal cell carcinoma (RCC) is an aggressive tumor, with an incidental discovery in most patients. Classic presentation is rare, and it has a high frequency of local and distant metastasis at the time of detection.CASE SUMMARY We present a rare case of a 58-year-old man with a ball-shaped thrombus in the right atrium at the time of first incidental identification of RCC in the emergency department. Cardiac metastasis, especially thrombus in the right atrium, is rare. It could either be a bland thrombus or a tumor thrombus, and physicians should consider this potentially fatal complication of RCC early at the time of initial presentation.CONCLUSION Ball-shaped lesions in the right atrium are rare, and bland thrombus should be differentiated from tumor thrombus secondary to intracardiac metastasis.
Key Words: Renal cell carcinoma; Metastasis; Tumor thrombus; Bland thrombus; Right atrium; Case report
INTRODUCTION
Renal cell carcinoma (RCC) is an aggressive tumor constituting about 3% of all adult malignancies, with a peak incidence in the sixth and seventh decades of life. The classic triad of flank pain, abdominal mass and hematuria is seen in 10% of the cases. Most cases have an incidental discovery[1,2] with local or distant metastases in 25% of the cases at the time of detection. About 10% of these patients have tumor extension into the renal vein and inferior vena cava[3], while only 1% of the total cases have the tumor extending into the right atrium[4]. We present a rare case of a 58-year-old man with a right atrial ball thrombus secondary to metastasis at the time of first incidental identification of RCC in the emergency department (ED).
CASE PRESENTATION
Chief complaints
A 58-year-old man presented to the ED with complaints of breathlessness and reduced effort tolerance for 1 wk.
History of present illness
A 58-year-old man presented to the ED with complaints of breathlessness and reduced effort tolerance for 1 wk. He denied chest pain, orthopnea or paroxysmal nocturnal dyspnea. He also noted a 10 kg weight loss over the last 2 mo. He went to a family physician where he was found to have hematuria and proteinuria on urine examination, and hence referred to the ED. He denied hematuria, lower urinary tract symptoms or fever.
History of past illness
He had no past medical history and was not on any long-term medication.
Physical examination
On presentation, his vital signs were stable but he appeared pale and had bilateral pitting lower limb edema up to the knees. Abdominal examination revealed a left sided large, palpable abdominal mass, but there was no rectal bleeding or melena. Examination of respiratory, cardiac and neurological systems was normal.
Laboratory examinations
His electrocardiogram showed normal sinus rhythm with T-wave inversions and ST-segment flattening in all leads, along with deep T inversions in leads V2-V4. Bedside ultrasound showed a large heterogeneous mass arising from the left kidney suspicious of RCC. Bedside echocardiogram showed a balllike structure in the right atrium (Figure 1), oscillating between the right atrium and right ventricle intermittently during cardiac cycles, suspicious for a tumor thrombus. There was no pericardial effusion but the right ventricle appeared larger than the left ventricle, suggestive of signs of right heart strain. Blood investigations showed hemoglobin 7.3 g/dL, elevated serum creatinine 155 mol/L (1.75 mg/dL) and N-terminal pro-B type natriuretic peptide 7325 pg/mL. The remaining blood tests, including liver panel, troponin-T, prothrombin time/activated partial thromboplastin time and severe acute respiratory syndrome coronavirus 2 polymerase chain reaction, were normal.

Figure 1 Bedside ultrasound showing ball-shaped thrombus in the right atrium (arrow).
Imaging examinations
Chest X-ray revealed mild pulmonary venous congestion. Computed tomography (CT) of the abdomen and pelvis (Figure 2) revealed a 13.9 cm × 15.8 cm × 16 cm irregular, heterogeneous left renal mass, suspicious of RCC, with extension of tumor into left renal vein and inferior vena cava (IVC) and metastasis to the liver. CT pulmonary-angiogram showed extensive right pulmonary embolism (Figure 3) with evidence of right heart strain and pulmonary arterial hypertension, as well as pulmonary metastasis (Figure 4). A thrombus was noted in the enlarged right ventricle and right atrial appendage.
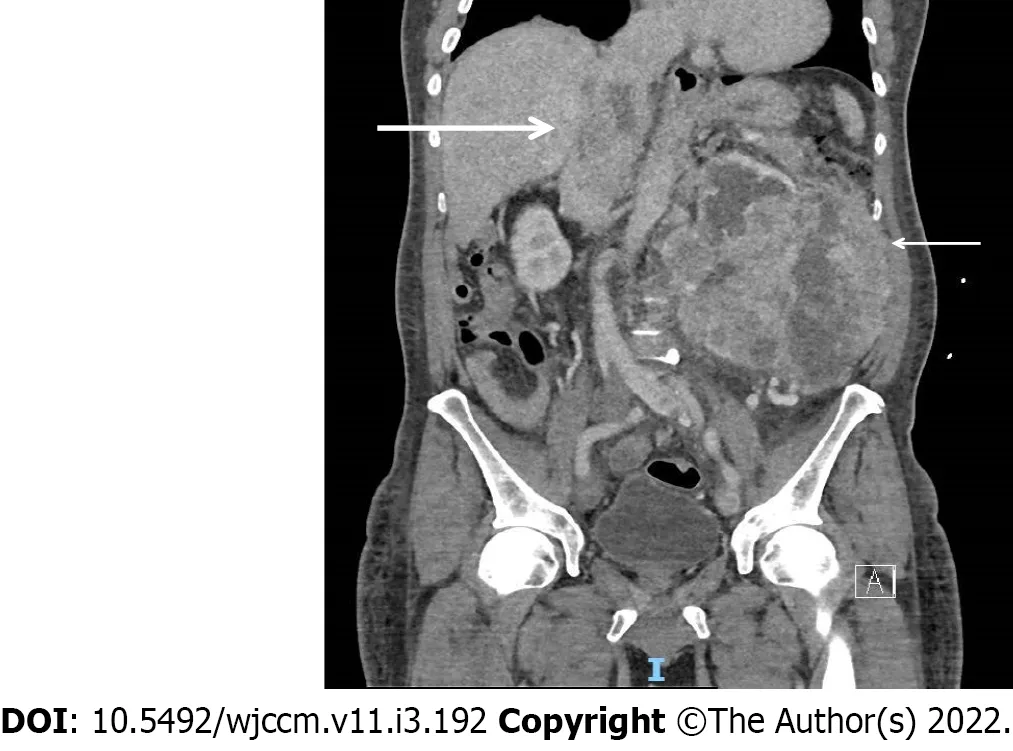
Figure 2 Computerized tomography scan of abdomen and pelvis showing left renal cell carcinoma (thin arrow) invading in to the hepatic portion of inferior vena cava (thick arrow).
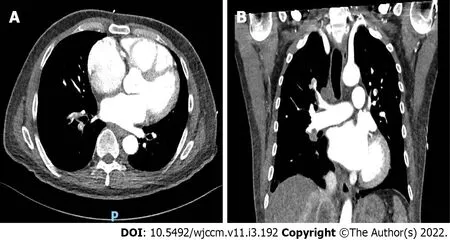
Figure 3 Large filling-defects in the right segmental and subsegmental branches and right lobar and interlobar arteries suggestive of right-sided pulmonary embolism. A: Right segmental and subsegmental branches; B: Right lobar and interlobar arteries suggestive of right-sided pulmonary embolism.
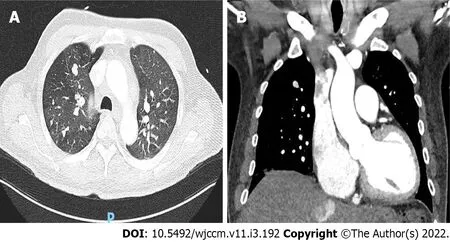
Figure 4 Multiple pulmonary nodules of varying sizes in the lungs suggestive of pulmonary metastasis. A: Multiple bilateral pulmonary nodules; B: Prominent right sided pulmonary metastasis.
MULTIDISCIPLINARY EXPERT CONSULTATION
The patient was commenced on subcutaneous enoxaparin 80 mg and admitted to a high dependency unit. Histopathology after imaging-guided biopsy of the left renal tumor revealed clear cell RCC. After discussion at the multidisciplinary tumor board meeting, he was not scheduled for cytoreductive nephrectomy and thrombectomy in view of metastatic burden.
FINAL DIAGNOSIS
He was diagnosed to have left RCC with ball-shaped thrombus in the right atrium, with associated right pulmonary embolism as well as pulmonary metastasis.
TREATMENT
He was treated with enoxaparin 80 mg twice daily and tyrosine kinase inhibitor (TKI) pazopanib 800 mg once daily.
OUTCOME AND FOLLOW-UP
He was discharged and scheduled for outpatient follow-up with a hematologist and oncologist (Figure 5).
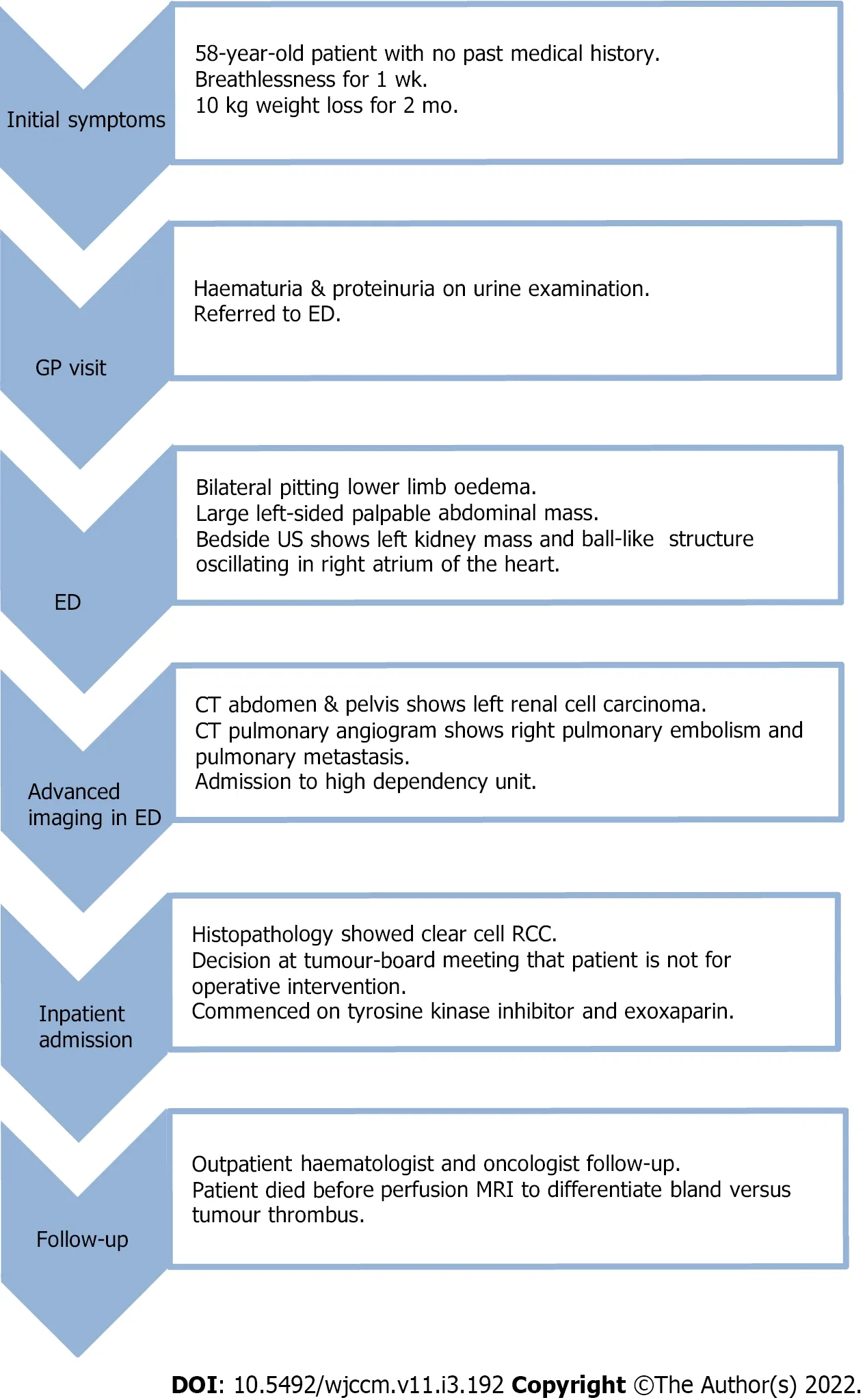
Figure 5 Timeline following case report guidelines. ED: Emergency department; CT: Computerized tomography; RCC: Renal cell carcinoma; MRI: Magnetic resonance imaging.
DISCUSSION
RCC can present as a solitary metastatic lesion or as a widespread systemic disease, but cardiac metastasis from RCC is extremely rare. The incidence of a thrombus in the right atrium is 0.75%, which is significantly lower than that that of a thrombus in the left atrium[5]. Thrombus in the right atrium is usually located at the atrial appendage or atrial wall. A ball thrombus in the right atrium is even rarer[5].
The ball-shaped lesion in our patient’s right atrium could either have been a bland thrombus or a tumor thrombus that spread along the IVC. In patients with malignancy, bland thrombus is usually a venous thrombus. Pathogenesis of ball thrombus is still unclear and it can be difficult to make a diagnosis. The challenge is to correctly differentiate bland thrombus from a tumor thrombus secondary to intracardiac metastasis, as it aids in appropriate therapeutic management as well as prognosis. On perfusion magnetic resonance imaging (MRI), heterogeneous enhancement of this ball-shaped lesion and presence of blood products within it suggests a tumor thrombus secondary to RCC metastases. On the contrary, a bland thrombus shows unrestricted diffusion and complete nulling of the mass on MR perfusion imaging[6]. Bland thrombus may resolve after thrombolytic and anticoagulant therapy, unlike tumor thrombus. Our patient unfortunately died before further evaluation could be conducted.
Combining cytoreductive nephrectomy and/or metastasectomy with chemotherapy helps in palliation. The possible surgical option for metastatic RCC extending into the right atrium and causing pulmonary embolism, in this patient, was cardiopulmonary bypass with deep hypothermic circulatory arrest, which is a safe and efficient method for removal of the tumor and thrombus[7]. Manual repositioning of the tumor thrombus out of the right atrium into the IVC on the beating heart is also a safe approach with low risk of tumor thrombembolization[8]. In recent times, the progression free survival has improved due to advances in chemotherapy, immunotherapy and TKI[9]. The overall long-term prognosis of patients with metastatic RCC is poor, with a median survival of 6-12 mo.
CONCLUSION
The classic presentation of RCC is rare, and patients can present with atypical symptoms and local or distant metastasis at the time of initial detection. Cardiac metastasis, especially thrombus in the right atrium, is rare and emergency physicians should consider it early at the time of presentation. Detection of a ball-shaped lesion in the right atrium is rare, and the patient should undergo appropriate evaluation with an aim to differentiate bland thrombus from a tumor thrombus secondary to intracardiac metastasis, as it aids in therapeutic management and prognosis.
FOOTNOTES
Author contributions:Pothiawala S lead conceptualization and wrote the original draft, reviewed and edited the draft; de Silva S and Norbu K wrote the original draft, reviewed and edited the draft.
Informed consent statement:Informed written consent was obtained from the patient for publication of this report and any accompanying images.
Conflict-of-interest statement:The authors declare that they have no conflict of interest.
CARE Checklist (2016) statement:The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Singapore
ORCID number:Sohil Pothiawala 0000-0002-4789-4326; Savan deSilva 0000-0002-3518-1740; Kunzang Norbu 0000-0002-2475-9578.
S-Editor:Guo XR
L-Editor:Kerr C
P-Editor:Guo XR
杂志排行

World Journal of Critical Care Medicine的其它文章
- Cough as a neurological sign: What a clinician should know
- Presentation and outcome of myocardial infarction with nonobstructive coronary arteries in coronavirus disease 2019
- Plasma D-dimer level in early and late-onset neonatal sepsis
- Stress cardiomyopathy in critical care: A case series of 109 patients
- Need for oxygen therapy and ventilatory support in premature infants in a hospital in Southern Brazil
- Critical care practices in the world: Results of the global intensive care unit need assessment survey 2020