Stress cardiomyopathy in critical care: A case series of 109 patients
2022-06-16ParthPancholiNaderEmamiMelissaFazzariSumitKapoor
Parth Pancholi, Nader Emami, Melissa J Fazzari, Sumit Kapoor
Parth Pancholi, Department of Medicine, Montefiore Medical Center, Albert Einstein College of Medicine, Bronx, NY 10467, United States
Nader Emami, Division of Critical Care Medicine, Department of Medicine, Montefiore Medical Center, Albert Einstein College of Medicine, Bronx, NY 10467, United States
Melissa J Fazzari, Department of Epidemiology and Population Health, Albert Einstein College of Medicine, Bronx, NY 10461, United States
Sumit Kapoor, Division of Critical Care Medicine, Department of Medicine, Montefiore Medical Center, Albert Einstein College of Medicine, Bronx, NY 10467, United States
Abstract BACKGROUND Critically ill patients are at risk of developing stress cardiomyopathy (SC) but can be under-recognized.AIM To describe a case series of patients with SC admitted to critical care units.METHODS We conducted a retrospective observational study at a tertiary care teaching hospital. All adult (≥ 18 years old) patients admitted to the critical care units with stress cardiomyopathy over 5 years were included.RESULTS Of 24279 admissions to the critical care units [19139 to medical-surgical intensive care units (MSICUs) and 5140 in coronary care units (CCUs)], 109 patients with SC were identified. Sixty (55%) were admitted to the coronary care units (CCUs) and forty-nine (45%) to the medical-surgical units (MSICUs). The overall incidence of SC was 0.44%, incidence in CCU and MSICU was 1.16% and 0.25% respectively. Sixty-two (57%) had confirmed SC and underwent cardiac catheterization whereas 47 (43%) had clinical SC, and did not undergo cardiac catheterization. Forty-three (72%) patients in the CCUs were diagnosed with primary SC, whereas all (100%) patients in MSICUs developed secondary SC. Acute respiratory failure that required invasive mechanical ventilation and shock developed in twenty-nine (59%) MSICU patients. There were no statistically significant differences in intensive care unit (ICU) mortality, in-hospital mortality, use of inotropic or mechanical circulatory support based on type of unit or anatomical variant.CONCLUSION Stress cardiomyopathy can be under-recognized in the critical care setting. Intensivists should have a high index of suspicion for SC in patients who develop sudden or worsening unexplained hemodynamic instability, arrhythmias or respiratory failure in ICU.
Key Words: Stress cardiomyopathy; Critical care; Shock; Respiratory failure
INTRODUCTION
Stress cardiomyopathy (SC) or Takotsubo cardiomyopathy or broken heart syndrome, was first described three decades ago in Japan[1]. It is characterized by acute and transient (< 21 d) left ventricular systolic and diastolic dysfunction, often precipitated by emotional or physical stress[1-6]. The diagnosis is usually made by modified Mayo Clinic criteria comprising of echocardiographic pattern of left ventricular apical hypokinesia, akinesia, or dyskinesia (apical ballooning) and basal hyperkinesis, electrocardiogram (EKG) changes (ST segment elevation and/or T wave inversion), troponin elevation and clean coronaries during cardiac catheterization[7].
Primary or classic SC has a reported incidence of around 1%-2% in patients with a suspicion of acute coronary syndrome (ACS) and is usually precipitated by physical or psychological stress[1]. Secondary SC, on the other hand, usually develops in hospitalized medical, surgical and neurological patients who may be under the major stress of critical illness in the medical-surgical intensive care unit (MSICU) setting[2,3,6,8-24].
The diagnosis of secondary stress cardiomyopathy in critically ill intensive care unit (ICU) patients can be challenging, requires a high degree of clinical suspicion, and is often under-recognized and under-reported for a myriad of reasons[8]. First, ICU patients do not always present with or report typical cardiac symptoms such as chest pain, shortness of breath, and syncope as patients presenting from the community do[8]. Second, there are no established diagnostic criteria for secondary stress cardiomyopathy in ICU patients and extrapolation of 2008 modified Mayo criteria may not be ideal[8]. Third, cardiac catheterization cannot be routinely performed in critically ill patients to confirm the diagnosis[8]. Fourth, patients can present with atypical morphologic variants of stress cardiomyopathy and there can be overlap with other diagnoses like sepsis induced cardiomyopathy[25]. Lastly, various multicenter international registries’ data did not include critically ill patients, thereby limiting understanding of the clinical presentation and outcomes of this disease in the ICU population[8].
Very few studies have reported the incidence, clinical features and outcomes of stress cardiomyopathy in the intensive care setting[3,9,10,12-19,25-27]. None of them compared characteristics and outcomes based on critical care unit [MSICUvscoronary care unit (CCU)]. The reported incidence of secondary stress cardiomyopathy in the ICU varies from 0.37% to as high as 28%[3,13,14,16,18,19]. Joet al[15] described underlying malignancy, male sex, old age and high APACHE2 score as the predictors of in-hospital mortality in patients with stress cardiomyopathy.
The aim of our research was to describe the case series of patients with stress cardiomyopathy admitted to the critical care units (CCUs and MSICUs) and study their clinical presentation, complications, and outcomes.
MATERIALS AND METHODS
Study design
We performed a retrospective case series study where all adult (≥ 18 years old) patients with the diagnosis of Stress cardiomyopathy or Takotsubo cardiomyopathy admitted to the critical care units of three hospitals in the Montefiore Healthcare System were included. Electronic health records for the 5-year period from January 1, 2015, to December 31, 2019, were retrospectively analyzed incorporating Looking Glass Clinical Analytics (Streamline Health, Atlanta, GA) to identify the target population. Critical care units included two coronary care units (CCUs) and five medical surgical units (medical, surgical or neurosurgical ICUs). The study was approved by the Institutional Review Board of the Albert Einstein College of Medicine (IRB# 2019-10754) and waiver of informed consent was granted due to minimal risk. Data about patient demographics, baseline characteristics, laboratory values, hospital course, complications and outcomes were collected for patients admitted to the critical care units.
Study definitions
The diagnosis of stress cardiomyopathy was made by the ICU teams collectively using a combination of 2-dimensional echocardiography, cardiac enzymes, EKG changes, and in some cases, coronary angiography.
Confirmed SC:Patients with SC who underwent cardiac catheterization to prove the absence of underlying coronary artery disease.
Clinical SC:Patients with SC who did not undergo cardiac catheterization and diagnosis was made clinically using 2D-echocardiography, cardiac enzymes and EKG changes only.
Primary SC:Patients with SC presenting from the community with cardiac symptoms like angina, dyspnea or palpitations. Clinical presentation mimics ACS, often precipitated by physical or mental stress.
Secondary SC:Patients developing SC during the course of hospitalization with critical medical, surgical or neurosurgical illness.
Typical variant of SC:Echocardiography regional wall motion abnormality pattern showing apical akinesis with basal hyperkinesis (apical ballooning).
Atypical variant of SC:Echocardiography regional wall motion abnormality pattern showing midventricular, basal, focal, or global hypokinesia.
Statistical analysis
Continuous variables were reported as median and interquartile range (IQR), whereas categorical variables were reported as counts and percentages. Associations between categorical variables and unit were testedviachi-square or Fisher’s exact test, as appropriate. Distributional differences between critical care units (CCUvsMS/ICU) with respect to continuous variables were assessedviaWilcoxon Mann-Whitney tests. Cumulative incidence functions for hospital discharge from the time of SC diagnosis stratified by critical care unit to allow for the competing risk of in-hospital death were estimated and differences tested using Grey’s test[28]. Cumulative incidence functions for in-hospital death from the time of SC diagnosis with a competing risk of hospital discharge alive were computed similarly. All analyses were performed using SAS software, version 9.4 (SAS Institute Inc., Cary, NC, United States) by the biomedical statistician. A two-sidedPvalue of 0.05 or less was considered statistically significant.
RESULTS
Incidence and baseline characteristics
Of 24279 admissions to the critical care units (19139 MSICU and 5140 in CCU) over the five-year study period, 109 patients with SC were identified. Sixty (55%) of them were admitted to the coronary care units and forty-nine (45%) to the medical-surgical units. The overall incidence of SC was 0.44%, incidence in CCU and MSICU was 1.16% and 0.25% respectively. Sixty-two (57%) had confirmed SC and underwent cardiac catheterization whereas 47 (43.1%) had clinical SC and did not undergo cardiac catheterization. Forty-three (72%) patients in the CCUs were diagnosed with primary SC, whereas all (100%) patients in MSICUs developed secondary SC.
Overall, the mean (SD) age was 67.2 (14.2) years and 72% were females. Hypertension and Diabetes Mellitus were the most common comorbidities seen in 65 (60%) and 40 (37%) patients respectively. Patients in the CCUs had more hypertension compared to those in MSICUs (70%vs47%,P= 0.01). Table 1 lists the baseline characteristics of the study patients, both overall and stratified by critical care unit (CCUvsMSICU).
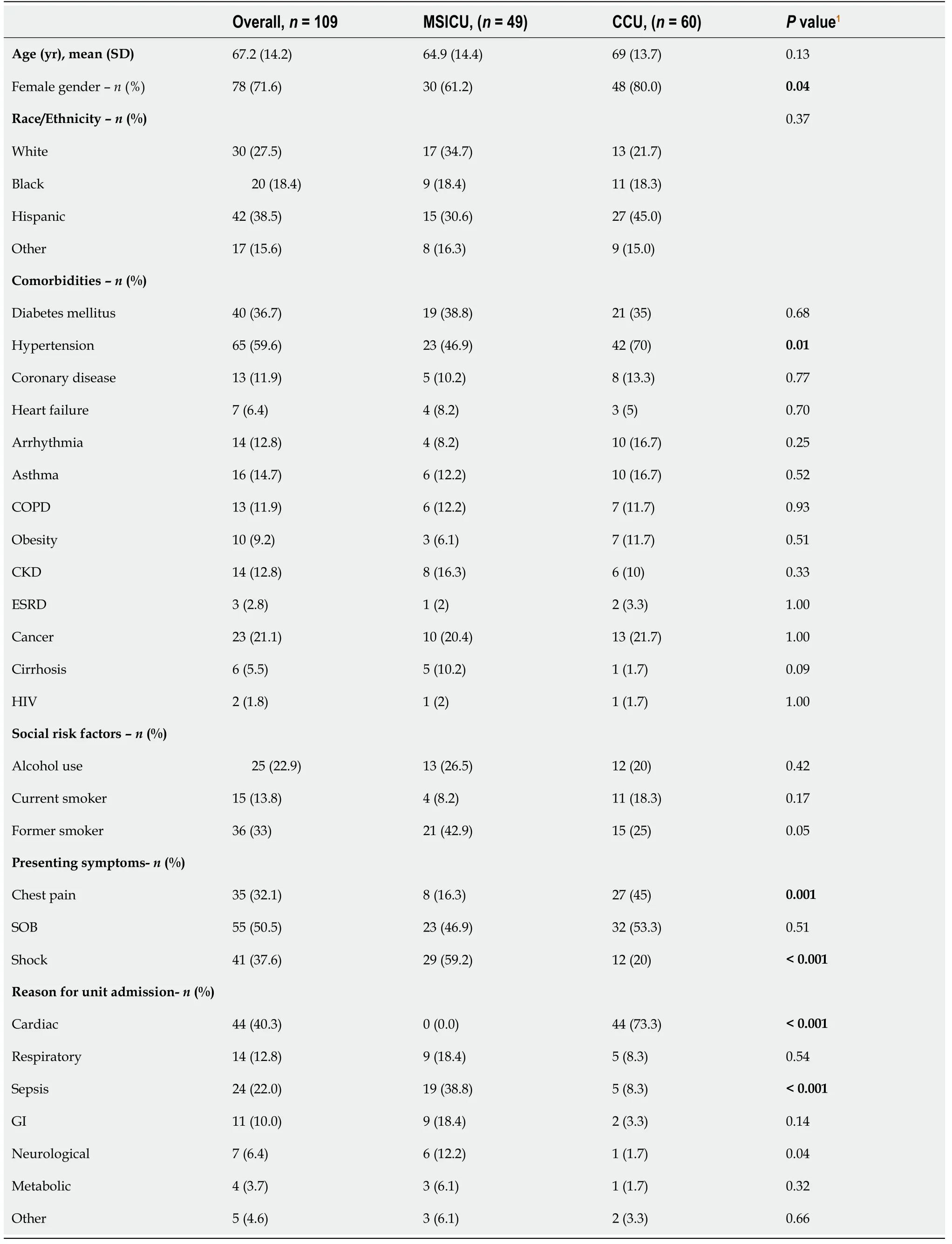
Table 1 Patient baseline characteristics and presentation by unit
Unit course, complications and outcomes
Shortness of breath was the most common presenting symptom seen in 55 (50%) of the patients overall. Twenty-seven (45%) patients in the CCU complained of chest pain compared to only eight (16%) in MSICUs. Acute respiratory failure that required invasive mechanical ventilation was seen in twentynine (59%) MSICU patients, as opposed to only fifteen (25%) in CCU. Twenty-nine (59%) of patients in medical-surgical units also developed shock compared to twelve (20%) of the cardiac patients. Septic shock was the most common type of shock in MSICUsvscardiogenic shock in CCUs (47%vs8%,P< 0.001).
All SC patients had transthoracic echocardiography performed, with only 12 (24.5%) in MSICU getting cardiac catheterization, compared to 50 (83.3%) CCU patients. The majority (n= 87, 80%) of the cases were of typical anatomical type with apical akinesia/hypokinesia and basal hyperkinesia (apical ballooning). Inotropic support was required in ten patients and mechanical circulatory support in three patients. Follow up echocardiogram was performed in sixty-nine (63.3%) patients, all of them had complete reversibility of cardiac function. Of 47 patients with clinical SC, 27 had follow up echocardiography; all of them showed return to baseline cardiac function. Table 2 presents the complications and outcomes of SC by type of unit (MSICUvsCCU).

Table 2 Stress cardiomyopathy diagnosis, complications and outcomes by unit

1n = 3 patients diagnosed prior to intensive care unit admission, corresponds to chi-square or Fisher’s exact test for association for categorical variables, Wilcoxon Mann-Whitney test for continuous variables.27 patients with clinical SC got follow up echocardiogram, reversibility seen in all of them. Data are summarized as median (IQR) or n (%), where n = available sample size. SC: Stress cardiomyopathy; MSICU: Medical surgical intensive care unit; CCU: Coronary care unit; EKG: Electrocardiogram; ECMO: Extracorporeal membrane oxygenation; IABP: Intraaortic balloon pump; AKI: Acute kidney injury; RRT: Renal replacement therapy; NIPPV: Non invasive positive pressure ventilation.
There was a statistically significant difference in the cumulative incidence function of hospital discharge stratified by critical care unit (0.56vs0.24 at 7 d,P= 0.01) but non-significant for in-hospital deaths stratified by critical care unit (P= 0.33) (Figure 1). Median length of stay from time of SC diagnosis to unit discharge was 1 d (range, 0-14) in CCUvs5 d (range, 1-24) in MSICU.
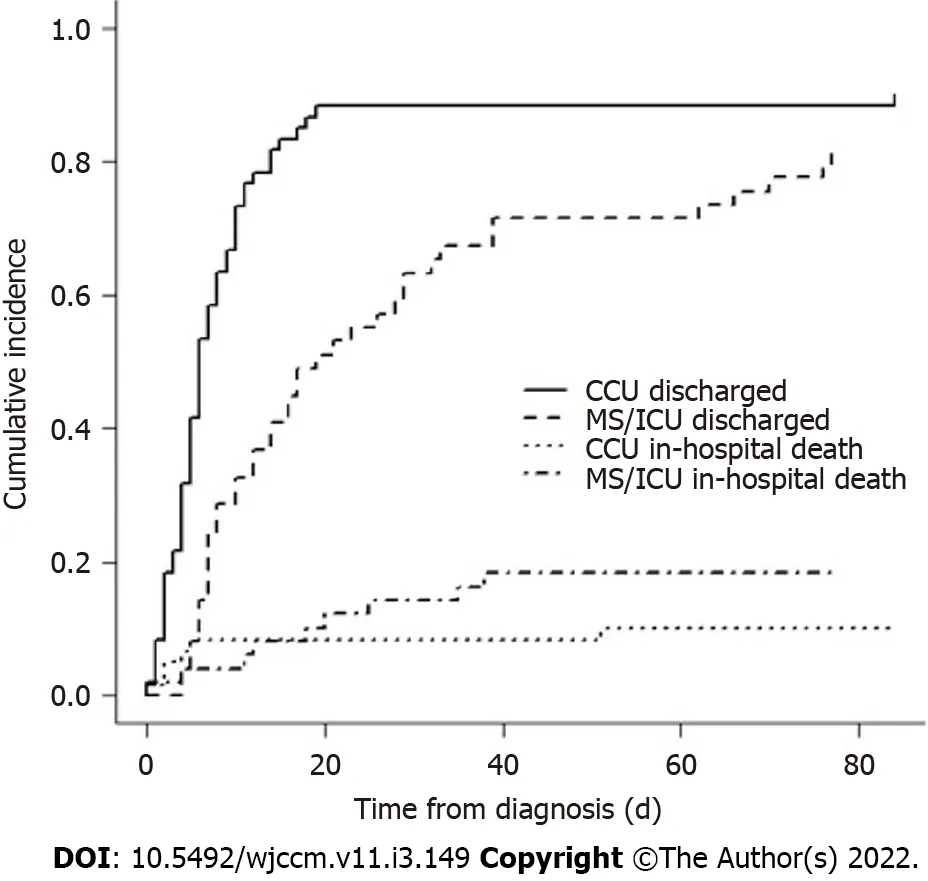
Figure 1 Cumulative incidence function curve for hospital discharge vs death. P = 0.01 for hospital discharge stratified by type of unit, P = 0.33 for in hospital death stratified by type of unit.
A total of fifteen patients died out of which eight deaths were in the critical care units. There were no statistically significant differences in the peak laboratory values of creatine phosphokinase (CPK), troponin and pro-BNP (pro-B-type natriuretic peptide) or outcomes like ICU mortality, in-hospital mortality, use of inotropic or mechanical circulatory support based on type of unit (MSICUvsCCU) or anatomical variant (typicalvsatypical) (Tables 3 and 4).
DISCUSSION
To our knowledge, this is the largest case series describing the clinical presentation, complications and outcomes of patients with stress cardiomyopathy admitted to the critical care units (MSICUs and CCUs). The overall incidence of SC in our patients was 0.44%, incidence in medical-surgical ICU was 0.25%, all of them having developed secondary SC. The incidence of SC in medical-surgical units varies per previous published reports. One of the earlier studies done by Parket al[13] in 2005 screened 92 consecutive critically ill patients admitted to medical ICU by serial echocardiography on day 1, 3, and 7. They observed a high incidence (28%) of left ventricular apical ballooning (LVAB) in medical ICU patients with no cardiac diseases. Patients with LVAB had higher prevalence of sepsis, hypotension upon ICU admission, use of inotropes, pulmonary edema, cardiomegaly and lower mean 2-month survival compared to patients without LVAB. The higher incidence of SC reported in the Parket al[13] study is likely because the diagnosis was solely made based on echocardiographic findings without integrating EKG, cardiac enzymes and coronary angiogram findings. An Australian study showed a much lower incidence of silent LVAB of around 3.5% in their medical ICU without any association of negative outcomes with silent LVAB[27]. Another prospective single center study by Doyenet al[14] in medical ICU patients found a high incidence of secondary SC of 4.6%. Our reported incidence of 0.25% in MSICUs is lower than the prior studies, because of the prospective nature of those studies, where all patients got echocardiographic screening for SC upon ICU admission. Muratsuet al[18] conducted a retrospective study on 5084 patients in Japan over a 5-year period and found a low incidence of clinical Takotsubo cardiomyopathy of 0.37%; a majority of their SC patients had the diagnosis of sepsis and subarachnoid hemorrhage. This demonstrates that there are likely many cases of SC which go underrecognized since formal echocardiography is not performed on every patient in the ICU. However, use of routine point of care ultrasound (POCUS) on critically ill ICU patients will likely identify many more cases of SC.
Sepsis and acute respiratory failure were the most common ICU diagnoses of patients developing secondary SC in these studies, which is similar to our patients in the MSICUs[13,14,18]. Kleberet al[29] reported a 15% prevalence of stress cardiomyopathy in the setting of acute respiratory failure requiring mechanical ventilation.

Table 3 Peak laboratory values by unit
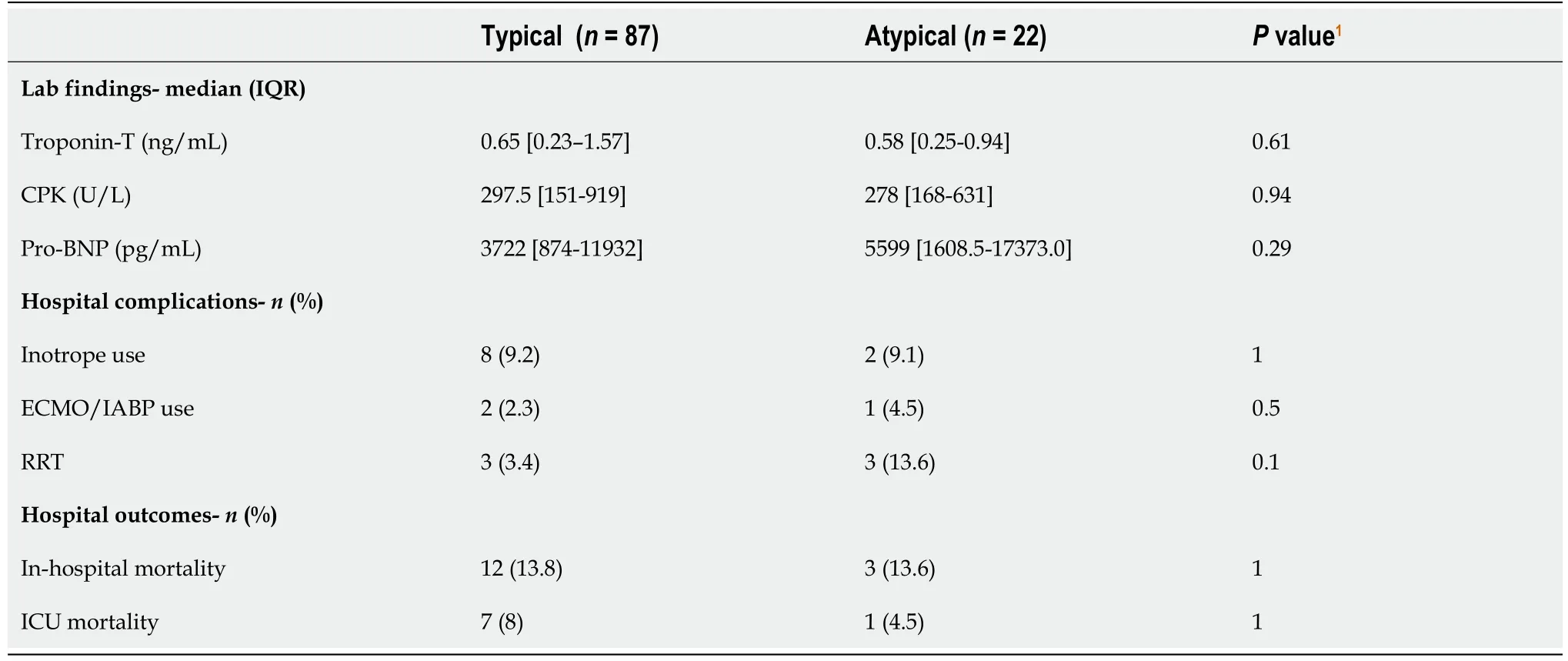
Table 4 Peak laboratory values and outcomes of stress cardiomyopathy by anatomical variant
We found that CCU patients mostly presented with primary SC from the community, many of them developing typical chest pain, shortness of breath and classic ST segment elevation on electrocardiogram.
It is reported that patients with secondary SC usually have an atypical presentation in the ICU, with the majority of them developing sudden or worsening unexplained shock/hemodynamic instability and shortness of breath[9,13,14,18,19]. Fifty-nine (59%) percent of our MSICU patients developed shock compared to 20% of CCU patients. In the prospective study by Doyenet al[14], 53.8% medical ICU patients developed cardiogenic shock. This is different from our findings as the most common type of shock in our study was septic shock. The likely explanation for this discrepancy is that 47% of our population in medical surgical ICUs had the diagnosis of severe sepsis and septic shock compared to 38% in the Doyen study.
The 2008 modified Mayo Clinic criteria and European Society of Cardiology (ESC) Heart Failure Association diagnostic criteria for stress cardiomyopathy require that patients have the absence of obstructive culprit coronary artery disease[30,31].
However, there are many reasons for forgoing cardiac catheterization in the critically ill ICU patients, such as hemodynamic instability, multi-organ failure, risk of acute kidney injury (AKI) due to contrast induced nephropathy or established AKI amongst others.
Only 25% of our patients in medical-surgical units underwent cardiac catheterization, compared to 83% in the cardiac units. The mainstay of diagnosis of clinical SC in these critically ill patients was the combination of transthoracic echocardiography, cardiac enzymes and electrocardiogram findings.
Previous reports of SC in medical-surgical ICUs also relied mainly on transthoracic echocardiography along with cardiac enzymes and EKG changes for diagnostic purposes for similar reasons[13,14,18]. With the integration of POCUS as a routine diagnostic tool in the management of ICU patients, there will be an earlier recognition and an increase in the number of patients diagnosed with Stress cardiomyopathy at bedside by Intensivists, thereby improving care of these patients[32].
Patients with secondary SC in MSICUs also had longer ICU and hospital lengths of stay compared to CCU patients, primarily because MSICU patients were sicker with stressors such as acute respiratory failure, septic shock, neurologic disorders and multi system organ failure. Interestingly, we found that 11% (n= 12) of our cases developed SC in the perioperative setting. Agarwalet al[33] performed a systematic review of perioperative SC and found 102 cases in 93 articles. Management of our perioperative SC cases was similar to non-perioperative cases.
We report a low overall mortality for patients with SC. This is similar to prior studies that also report favorable outcomes of this patient population[3,9,10,13,14,18,19]. A relatively fast and complete recovery of cardiac function may explain this finding. Fifty-seven percent of our clinical SC patients had follow up echocardiogram, all showing reversibility of cardiac function, further supporting the diagnosis of SC. We also did not find any differences in mortality based on unit type (MSICUvsCCU) or anatomical type (typicalvsatypical).
The major strength of our study is that we describe a large case series of patients with stress cardiomyopathy over the five-year period. We report and compare for the first time, characteristics, complications and outcomes of stress cardiomyopathy stratified by the type of unit and anatomical type. Our study has few limitations that need to be acknowledged. First, it is a single center study. Second, it is retrospective in nature and hence some data elements may not be captured accurately. Third, we believe that our incidence is likely underestimated, as many cases of SC may have gone unrecognized. Fourth, our definition of clinical SC could include cases of myocardial ischemia, showing improvement with development of collateral circulation. Fifth, follow up echocardiograms were only available in only 69 (63.3%) patients.
CONCLUSION
Stress cardiomyopathy can be under-recognized in the critical care setting. Primary stress cardiomyopathy is commonly seen in the CCUs and the secondary form predominates in the MSICU setting. Presentation of secondary SC is often atypical and the majority of patients have simultaneous acute respiratory failure and sepsis. Intensivists should have a high index of clinical suspicion for SC in patients who develop sudden or worsening unexplained hemodynamic instability, arrhythmias, or respiratory failure. Many of the SC cases in MSICU may be diagnosed clinically as cardiac catheterization is not always feasible. Routine utilization of POCUS on all ICU patients will help identify more cases. The outcomes of these patients are excellent as majority of them show reversibility of cardiac function on follow up imaging.
ARTICLE HIGHLIGHTS
Research background
Critically ill patients are at risk of developing stress cardiomyopathy (SC) but can be under-recognized.
Research motivation
Our goal was to learn more about patients with SC in the intensive care unit (ICU) setting.
Research objectives
To study the patient characteristics, clinical course, and outcomes of critically ill patients with SC.
Research methods
We conducted a retrospective observational study at a tertiary care teaching hospital. All adult patients admitted to the critical care units with Stress cardiomyopathy over 5 years were included.
Research results
One hundred and nine patients were identified with SC, with 55% of them in the coronary care units(CCU) and 45% in the medical-surgical intensive care units (MSICUs). 57% of patients had SC confirmed by cardiac catherization while 43% were diagnosed clinically with echocardiography. 72% of CCU patients had primary SC whereas all MSICU patients had secondary SC. 59% of MSICU patients developed shock and acute respiratory failure that required mechanical ventilation. There were no statistically significant differences in ICU mortality, in-hospital mortality, use of inotropic or mechanical circulatory support based on type of unit or anatomical variant.
Research conclusions
Primary SC was commonly seen in the CCUs while secondary SC was seen more commonly in the MSICUs. Secondary SC often presents atypically and many patients have acute respiratory failure and sepsis. Many of the SC cases in the MSICU may be diagnosed clinically as cardiac catherization is not always feasible. Patients with SC in the ICUs have excellent outcomes with the majority of them showing reversibility of cardiac function.
Research perspectives
Stress Cardiomyopathy is often under-recognized in the critical care setting. In the MSICUs, secondary SC is the main form of SC encountered, where is it is often diagnosed clinically. Routine use of Point-ofcare ultrasound may help with early identification of these cases.
ACKNOWLEDGEMENTS
We would like to thank Dr. Peter Dicpinigaitis for reviewing our manuscript and providing valuable feedback.
FOOTNOTES
Author contributions:Pancholi P contributed with data acquisition, data analysis, and manuscript writing; Emami N contributed with data acquisition, analysis and manuscript editing; Fazzari MJ performed the data analysis; Kapoor S designed the study, contributed to manuscript writing, and provided overall supervision; all authors have read and approve the final manuscript.
Institutional review board statement:The study was approved by the Institutional Review Board of the Albert Einstein College of Medicine (IRB# 2019-10754) and waiver of informed consent was granted due to minimal risk.
Conflict-of-interest statement:The authors report no conflicts of interest.
Data sharing statement:Technical appendix, statistical code, and dataset available from the corresponding author. Participant consent was not obtained but the presented data are anonymized and risk of identification is low.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:United States
ORCID number:Parth Pancholi 0000-0002-1319-4882; Nader Emami 0000-0002-9001-9287; Melissa J Fazzari 0000-0002-5674 -3589; Sumit Kapoor 0000-0002-5683-3445.
S-Editor:Liu JH
L-Editor:A
P-Editor:Liu JH
杂志排行

World Journal of Critical Care Medicine的其它文章
- Cough as a neurological sign: What a clinician should know
- Presentation and outcome of myocardial infarction with nonobstructive coronary arteries in coronavirus disease 2019
- Plasma D-dimer level in early and late-onset neonatal sepsis
- Need for oxygen therapy and ventilatory support in premature infants in a hospital in Southern Brazil
- Critical care practices in the world: Results of the global intensive care unit need assessment survey 2020
- Diuretic combinations in critically ill patients with respiratory failure:A systematic review and meta-analysis