Presentation and outcome of myocardial infarction with nonobstructive coronary arteries in coronavirus disease 2019
2022-06-16KevinJohnAmosLalNitishSharmaAmrElMeligyAjayMishra
Kevin John, Amos Lal, Nitish Sharma, Amr ElMeligy, Ajay K Mishra
Kevin John, Department of Critical Care, Believers Church Medical College Hospital,Thiruvalla 689103, Kerala, India
Amos Lal, Division of Pulmonary & Critical Care Medicine, Mayo Clinic, Rochester, MN 55905, United States
Nitish Sharma, Division of Cardiology, Saint Vincent Hospital, Worcester, MA 01608, United States
Amr ElMeligy, Division of Interventional Cardiology, Saint Vincent Hospital, Worcester, MA 01608, United States
Ajay K Mishra, Department of Cardiovascular Medicine, Saint Vincent Hospital, Worcester, MA 01608, United States
Abstract Among the cardiac complications of coronavirus disease 2019 (COVID-19), one increasingly reported in the literature is myocardial infarction with nonobstructive coronaries (MINOCA). We reviewed all reported cases of MINOCA in COVID-19 patients to summarize its clinical features, evaluation, and treatment. We performed a literature search in Pubmed using the search terms ‘COVID-19’ and ‘MINOCA’ or ‘non-obstructive coronaries’. Among the reported cases, the mean age was 61.5 years (SD ± 13.4), and 50% were men. Chest pain was the presenting symptom in five patients (62.5%), and hypertension was the most common comorbidity (62.5%). ST-elevation was seen in most patients (87.5%), and the overall mortality rate was 37.5%. MINOCA in COVID-19 is an entity with a broad differential diagnosis. Therefore, a uniform algorithm is needed in its evaluation to ensure timely diagnosis and management.
Key Words: COVID-19; Myocardial infarction with non-obstructive coronary arteries;Outcome
INTRODUCTION
Myocardial infarction with non-obstructive coronaries (MINOCA) is defined as a rise or fall of cardiac troponin, with at least one value above the 99thpercentile of the upper reference limit, corroborative clinical evidence of infarction (classic symptoms, electrocardiogram changes, or new wall motion abnormality), non-obstructive coronary arteries on angiography (< 50% obstruction), and lack of an alternative diagnosis[1]. MINOCA is seen in 5%-6% of patients with acute myocardial infarction (AMI)[2]. However, this number may be as high as 15% in certain subgroups[2]. Compared to patients with AMI due to obstructive coronary artery disease (CAD), patients with MINOCA are younger, consist of more women, and have a lesser prevalence of traditional risk factors such as dyslipidemia, diabetes mellitus, hypertension, tobacco use, and family history of AMI[1].
The coronavirus disease 2019 (COVID-19) pandemic, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has led to more than 4,250,000 deaths worldwide. Although primarily a respiratory illness, it is becoming increasingly clear that COVID-19 is a multi-system disease. How COVID-19 affects the cardiac system has been well documented. However, as more cases are reported, uncommon presentations and complications of COVID-19 are surfacing. Although there have been many reports of MINOCA in COVID-19 patients, a unified approach to evaluate such patients is lacking. In this paper, we review cases of MINOCA reported in patients with COVID-19 and provide a summary of its clinical features, evaluation, and treatment.
METHODS
In this review, we included articles on COVID-19 and MINOCA published in PubMed until January 2022. We used the search terms ‘COVID-19’ and ‘MINOCA’ or ‘non-obstructive coronaries’. Case reports, case series, retrospective, and prospective observational studies on adult patients with COVID-19 were eligible to be included. We excluded opinions, recommendations, and reviews that did not have clinical details of patients. Patients whose initial diagnosis of MINOCA was modified after further evaluation were also excluded. Studies in languages other than English were translated using Google Translate. Two independent clinicians were involved in the screening of the articles.
RESULTS
We found five cases and one case series of three patients with MINOCA and COVID-19[3-8] (Table 1). We also found five observational studies of MINOCA in COVID-19 patients, which are discussed seperately[9-13] (Table 2). Among the reported cases, the mean age of patients was 61.5 years (SD ± 13.4), and 50% were men.
Demographic details and presentations
Chest pain was the presenting symptom in five patients (62.5%), two patients (25%) had dyspnea without chest pain, and one patient (12.5%) was found unresponsive at the time of presentation. Hypertension was the most common comorbidity and was present in 62.5% of the patients. Other comorbidities included diabetes mellitus, chronic obstructive pulmonary disease, non-ischemic heart failure with reduced ejection fraction, past ST-elevation myocardial infarction (STEMI), hypercholesterolemia, and motor-neuron disease.
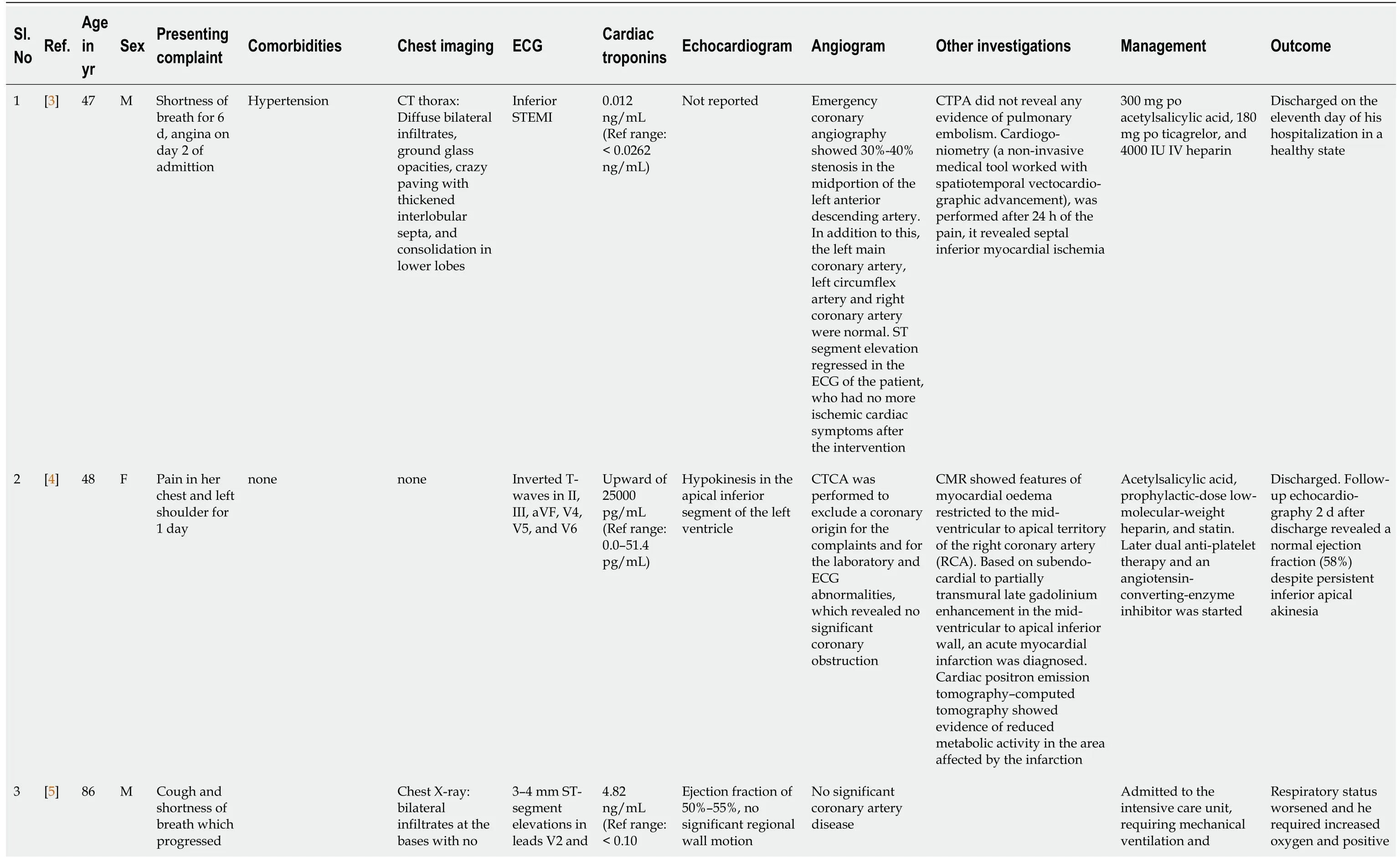
Table 1 Case reports of myocardial infarction with non-obstructive coronary arteries in coronavirus disease 2019

to acute hypoxemic respiratory failure requiring intubation other abnormalities V3 ng/mL abnormalities, and no signs of cardiac tamponade vasopressor support end-expiratory pressure, renal function worsened, as did lymphopenia and inflammatory biomarker abnormalities. Died on day 8 4[6]61 M Shortness of breath, respiratory failure requiring intubation Hypertension, diabetes mellitus 2 mm of anterolateral STelevation without reciprocal depression 6283 ng/L (Ref range: < 40 ng/L)Moderate left ventricular systolic dysfunction No luminal stenosis or thrombosis, with preserved TIMI 3 flows in all coronary arteries Left ventriculography: Mild apical hypokinesis Loading dose of ticagrelor and IV heparin On day 13, he was anuric and CVVH was started. Continued to worsen and died 5[6]59 F Found minimally responsive on the ground. Intubated by paramedics Hypertension, COPD CT thorax: Bilateral lower lung lobe infiltrates and pulmonary oedema with moderate calcification in the mid-left anterior descending artery ST-segment elevations in V1-V4 and reciprocal STdepressions in leads II, III, and aVF 2390 ng/L reduced left ventricular ejection fraction of 40% with antero-apical wall hypokinesis Moderate diffuse atherosclerotic disease was observed in the left system with no significant luminal obstruction elsewhere Not specified Extubated on Day 3. Discharged home subsequently 6[6]69 F acute onset chest tightness and dyspnea Non-ischemic heart failure with reduced ejection. Implantable cardioverterdefibrillator was placed in 2004. Motor neurone disease, diagnosed 4 yr previously Chest X-ray: Bilateral infiltrates Left bundle branch block. On day 3 progressive dynamic concordant ST-elevation in V1-V2 and STdepression in V3-V5 504 ng/L Impaired left ventricular function which was similar to baseline No obstructive atheroma or thrombus Loading dose dual antiplatelets, therapeutic low molecular weight heparin, high-dose IV diuretics, and IV nitrates The patient died on Day 7 of admission Chest X-ray: Bilateral interstitial prominenceCT chest: perihilar ground glass opacities, thickening of interlobular septa, and minimal bilateral Admitted to Cardiac Intensive Care Unit and started on supportive measures. Treated with lopinavir/ritonavir 400 mg/100 mg tablet every 12 h for 4 d and hydroxychloroquine 500 mg every 12 h, then hydroxy-7[7]51 M Left sided chest pain, diaphoresis, syncope Hypertension and hypercholesterolemia 3.5 mm ST elevation in I and avL, 5 mm isolated ST elevation in lead V2, with deep reciprocal depressions in III, avF and avR Not reported Preserved left ventricular ejection fraction (LVEF) of 55% and anteroapical hypokinesis on ventriculography Patent coronary arteries The patient recovered and was discharged home on day 26 on aspirin, statin and metoprolol

M: Male; F: Female; ECG: electrocardiogram; CT: Computed tomography; STEMI: ST-elevation myocardial infarction; CTPA: Computed tomographic pulmonary angiography; CTCA: Computed tomography coronary angiography; CMR: Cardiac Magnetic Resonance Imaging; TIMI: Thrombolysis in myocardial infarction; CVVH: Continuous veno-venous hemofiltration; COPD: Chronic Obstructive Pulmonary Disease.
Investigations
ST-elevation was seen in most patients (87.5%), while one patient (12.5%) had only T-wave inversion. In addition, a new-onset left bundle branch block was seen in one patient (12.5%)[6]. Three-quarters of all patients had elevated troponin levels. On echocardiography, three patients (37.5%) had reduced ejection fraction, and four (50%) had preserved ejection fraction. One case report did not include echocardiography findings. Non-obstructive coronary arteries were demonstrated by invasive angiography in all patients, except one who underwent computed tomography coronary angiography (CTCA)[4]. Cardiac magnetic resonance imaging (CMR) was performed on one patient. It showed myocardial edema restricted to the mid-ventricular to apical territory of the right coronary artery, and subendocardial-topartially transmural late gadolinium enhancement in the mid-ventricular to apical inferior wall. These findings were suggestive of acute myocardial infarction[4]. The same patient underwent cardiac positron emission tomography-computed tomography (PET-CT), which showed reduced metabolic activity in the area affected by the infarction. Another patient underwent computed tomographic pulmonary angiography, which ruled out pulmonary embolism, and cardiogoniometry, which revealed septal inferior myocardial ischemia[3].
Treatment and outcome
While most patients were treated with supportive care, antiplatelets, statins, and anticoagulation, one patient received anti-viral therapy (lopinavir/ritonavir) with hydroxychloroquine[7]. The overall mortality rate was 37.5%.
Observational studies reporting outcomes of MINOCA in COVID-19
In the five observational studies included in this review, the incidence of MINOCA among COVID-19 patients with an acute coronary syndrome varied from 5.2% to 54.5%[9-13]. Demographic details were only reported in the study by Stefaniniet al[9]. The mean age of patients with MINOCA in that study was 69.27 years (SD ± 10.6), and 54.5% were male. Hypertension was the most common comorbidity (91.8%), followed by chronic kidney disease (45.4%), dyslipidemia (27.3%) and diabetes mellitus (9.1%). The proportion of patients with ST-elevation on ECG was between 81.8% and 100%, and the mortality rate ranged from 45.4% to 66%.
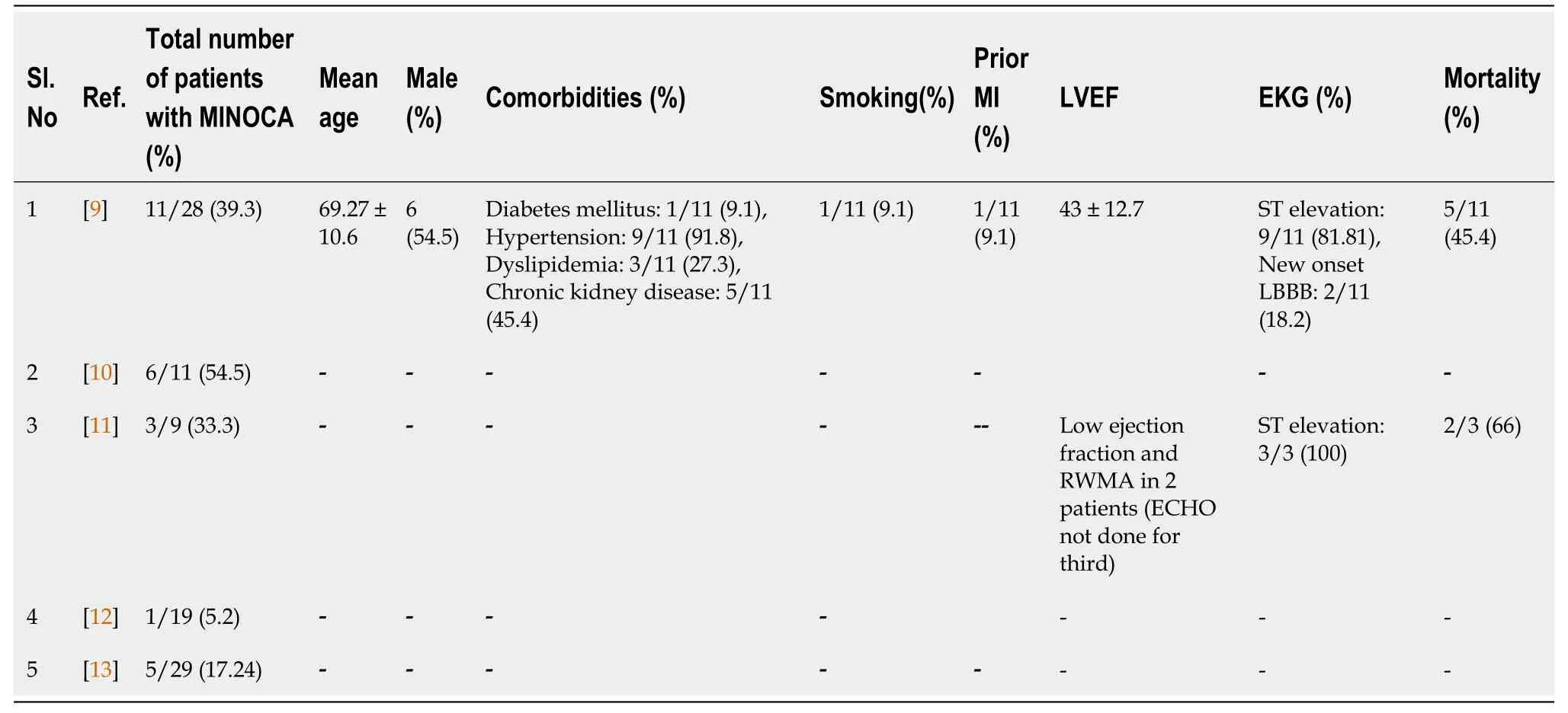
Table 2 Studies that reported myocardial infarction with non-obstructive coronary arteries in coronavirus disease 2019
DISCUSSION
Gross and Sternberg first described MINOCA in 1939[14]. Later, the term MINC or MINCA (myocardial infarction with normal coronary arteries) was coined, which was modified to MINOCA to be more inclusive. Other words that have been used in the literature to describe this pathology include ‘acute coronary syndromes with normal or near-normal coronary arteries’ (ACS-NNOCA) and ischemic syndromes with non-obstructive coronaries (INOCA). Strictly speaking, MINCA is a subset of MINOCA, which is a subset of ACS-NNOCA. The subtle differences between these terms have been confusing as these terms are often used interchangeably. Nevertheless, the term MINOCA provides a framework for evaluating such patients and is often used as a ‘working diagnosis’. Further evaluation may reveal secondary causes such as myocarditis, Takostubo cardiomyopathy, sepsis, cardiac contusion, spontaneous coronary artery dissection, microvascular disease, coronary artery spasm, or missed obstructive coronary artery disease. If a secondary cause is not found, a diagnosis of ‘unclassified MINOCA’ is made[1].
The proportion of MINOCA seems to be higher in COVID-19 patients. In the study by Popovicet al[10], there was a statistically significant increase in the proportion of MINOCA in COVID-19 patients compared to a historical cohort (54.5%vs1.4%,P< 0.001). Due to the heterogeneity in case definitions and evaluation protocols between centers, the actual proportion of MINOCA among COVID-19 patients is difficult to estimate. One can gauge the upper limit of this estimate from the proportion of COVID-19 patients with acute cardiac injury (ACI), which is one of the earliest measures of cardiac involvement reported during the COVID-19 pandemic. ACI, defined as cardiac-troponin elevation with values exceeding the 99thpercentile of the upper reference limit, was observed in 8%-62% of COVID-19 patients[15]. Also noteworthy was that any amount of cardiac injury was significantly associated with mortality (adjusted HR 1.75,P< 0.001)[16].
Some other characteristics of COVID-19 patients with MINOCA can be extrapolated from the results of a systematic review of 161 patients from 42 studies of COVID-19 patients with ST-elevation[17]. The authors observed that patients with non-obstructive CAD had more diffuse ST-segment elevation (13%vs1%,P= 0.03) and diffuse left ventricular wall-motion abnormality (23%vs3%,P= 0.02) when compared to those with obstructive CAD[17]. In the same review, the proportion of men in the group with obstructive CAD was higher than in the group with non-obstructive CAD (79%vs57%)[17].
Our literature review found that many patients with COVID-19 and MINOCA received alternative diagnoses such as Takotsubo cardiomyopathy, coronary vasospasm, myocarditis, and coronary vasculitis on further evaluation. This is consistent with the concept that MINOCA is a dynamic diagnosis, and patients who were initially diagnosed with MINOCA may receive a revised diagnosis on further evaluation. However, some patients were presumed to have myocarditis without objective evidence for the same[18-21]. A diagnosis of MINOCA or MINOCA under evaluation would better suit such patients. It must also be noted that the cases of MINOCA with COVID-19 that were included in this review are cases of ‘unclassified MINOCA.’
Specific causes for MINOCA in COVID-19 patients
Myocarditis:Myocarditis is defined as an inflammatory disease of the myocardium diagnosed by histological, immunological, immunohistochemical, and molecular criteria[22]. There have only been a handful of COVID-19 patients with endomyocardial biopsy-proven myocarditis[23,24]. Even in these patients, the SARS-CoV-2 genome could not be isolated from the biopsy sample. Thus, there is no conclusive proof that SARS-CoV-2 infects the myocardium resulting in myocarditis. Instead, the mechanism is probably one of immune-mediated damage and would justify steroids for treatment. However, many COVID-19 patients who were diagnosed with myocarditis do not meet the strict diagnostic criteria for the same, and giving steroids to such patients may be harmful[18-21].
Takotsubo cardiomyopathy:Takotsubo cardiomyopathy is an intriguing disorder, and its mechanism is yet to be elucidated fully. Takotsubo cardiomyopathy has been well documented in COVID-19 patients and can be due to the infection or the emotional stress associated with the pandemic[25]. Whether Takotsubo cardiomyopathy should be included as a cause of MINOCA is debatable. This is because the ‘Fourth Universal Definition of Myocardial Infarction’ does not consider Takotsubo cardiomyopathy a form of myocardial infarction[26]. On the other hand, the elevation of cardiac troponins is well documented in Takotsubo cardiomyopathy[27]. In our opinion, Takotsubo cardiomyopathy must be included in the diagnostic algorithm of MINOCA as there seems to be an increased incidence in COVID-19. Such a diagnosis carries certain therapeutic and prognostic implications as well.
Coronary vasculitis:Although coronary vasculitis is a rare cause of MINOCA, it has been reported in patients with COVID-19. Feuchtneret al[27] described an interesting case of a 48-year-old COVID-19 patient who was evaluated for chest pain and was found to have non-obstructive coronaries suggestive of MINOCA. However, further evaluation with CMR confirmed subendocardial inferior zonal late enhancement, and CTCA showed diffuse irregular vessel wall thickening and perivascular edema suggestive of vasculitis. The patient was managed with acetylsalicylic acid and clopidogrel and was discharged after cardiac enzyme levels declined. Postmortem studies showed COVID-19 viral inclusion bodies in endothelial cells, supporting the possibility of endothelial cell infection and endarteritis[28]. Hence, COVID-19 induced coronary vasculitis may be more common than currently reported. This case also underscores the importance of identifying patients with MINOCA and evaluating them further, rather than giving a presumptive diagnosis of myocarditis.
Spontaneous coronary artery dissection:Multiple case reports in COVID-19 patients have documented spontaneous coronary artery dissection[29-32]. The obstruction is caused by the separation of the medial and adventitial walls, with an intramural hematoma protruding into the lumen. It is hypothesized that there is an intrinsic underlying vasculopathy, and the dissection is precipitated by stress, catecholamine surge, physical activity, or sympathetic stimulation[33]. The underlying endothelial dysfunction and thrombo-inflammation may be the reason for coronary artery dissection occurring in COVID-19.
Coronary vasospasm:Diagnosis of coronary vasospasm in COVID-19 patients with MINOCA is challenging, but possible, if a systematic approach is followed. This was demonstrated by Riveroet al[34] in their case report of a 66-year-old man who presented with bilateral COVID-19 pneumonia and chest pain. After angiography, optical coherence tomography showed a stable, mainly fibrotic atheromatous plaque. The diagnosis of coronary vasospasm was clinched by administering intracoronary ergonovine at increasing doses which led to severe chest pain and universal ST-segment elevation. Coronary angiography done at this time revealed nearly occlusive coronary vasospasm involving both the left anterior descending coronary artery and left circumflex coronary artery. Given how challenging it is to diagnose coronary vasospasm, it may be another under-reported cause of MINOCA in COVID-19.
Miscellaneous causes:Type 2 myocardial infarction refers to events that occur due to a mismatch between myocardial oxygen supply and demand[26]. This is a heterogeneous class that can include various causes such as sepsis, anemia, arrhythmia, and pulmonary embolism-all of which can be seen in the setting of COVID-19 infection.
Evaluation of MINOCA
The differential diagnosis for MINOCA is broad, and therefore, a complete history and physical examination must remain at the core of its evaluation. It is also vital to re-take history and re-examine the patient multiple times at various stages of the evaluation process. This will ensure that investigations are directed appropriately and a ‘fishing-expedition’ approach is avoided. The initial set of investigations may give clues to the underlying diagnosis before more invasive tests are undertaken. In a prospective cohort of STEMI patients who underwent primary percutaneous coronary intervention (PPCI) during the COVID-19 outbreak, patients with COVID-19 and MINOCA had elevated markers of inflammation and abnormal coagulation parameters[10]. Moreover, anti-phospholipid antibodies were observed in three of these patients.
Once obstructive coronary artery disease has been ruled out, the most important investigation for evaluating the cause of MINOCA is CMR[35]. A large prospective multicenter observational study conducted from 2007 to 2011 included 152 patients with MINOCA. In this study, CMR showed that 19% of the patients had signs of myocardial necrosis, 7% had signs of myocarditis, and 7% had unrecognized hypertrophic cardiomyopathy or could not be classified[36]. A meta-analysis of 34 studies with 199 COVID-19 patients for whom CMR was performed showed abnormal results in 79% and myocarditis in 40.2%[37]. A caveat is that the absence of myocardial necrosis on CMR does not exclude MINOCA as they may have other findings that support the diagnosis[38].
Prognosis
While the prognosis of MINOCA depends on the underlying disease, most studies to date indicate a better prognosis for MINOCA when compared to patients with AMI due to obstructive CAD[2]. A review of ST-elevation in COVID-19 patients observed an overall in-hospital mortality of 30%, with no significant difference between obstructive and non-obstructive CAD[17]. This is comparable with the mortality rate of 37.5% in our review. The effect of anti-viral therapy for MINOCA on COVID-19 is debatable. While none of the patients who died received anti-viral therapy, the small sample size and study designs preclude us from drawing definite conclusions[39,40]. As more cases of MINOCA are reported, it may be feasible to conduct well-designed prospective studies to explore these questions further.
LIMITATIONS
There are several limitations to this review. Many cases of MINOCA may have been treated along the lines of COVID-19 associated myocarditis. Therefore, it is likely that MINOCA is grossly under-reported in the literature. The small sample size of this review, due to the under-reporting of cases and the rarity of this condition, limits the generalizability of our findings. The publication of challenging cases with a positive outcome may have led to publication bias. There is also a lack of uniformity in the evaluation and diagnosis of MINOCA in COVID-19[41].
CONCLUSION
This review highlights that MINOCA in COVID-19 has a broad differential diagnosis that must be evaluated with a systematic diagnostic algorithm. COVID-19 patients with MINOCA had a mean age of 61.5 years, and 50% of them were men. The most common presenting symptom was chest pain (62.5%), and ST-elevation was present in most patients (87.5%). The overall mortality rate was 37.5%. More studies are required to arrive at a reliable estimate of the true prevalence and prognostic relevance of MINOCA.
FOOTNOTES
Author contributions:John K and Mishra AK contributed to the conceptual design of the study; John K and Mishra AK independently screened the articles and extracted the data; John K, Mishra AK, and Lal A contributed to the write-up and submission of the study; Mishra AK and Lal A reviewed the final manuscript; All authors reviewed and agreed with the final content of the article.
Conflict-of-interest statement:The authors declare that they have no conflict of interest.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:United States
ORCID number:Kevin John 0000-0003-3382-0294; Amos Lal 0000-0002-0021-2033; Nitish Sharma 0000-0002-6221-3197;Amr ElMeligy 0000-0002-3053-0024; Ajay K Mishra 0000-0003-4862-5053.
S-Editor:Liu JH
L-Editor:A
P-Editor:Liu JH
杂志排行

World Journal of Critical Care Medicine的其它文章
- Cough as a neurological sign: What a clinician should know
- Plasma D-dimer level in early and late-onset neonatal sepsis
- Stress cardiomyopathy in critical care: A case series of 109 patients
- Need for oxygen therapy and ventilatory support in premature infants in a hospital in Southern Brazil
- Critical care practices in the world: Results of the global intensive care unit need assessment survey 2020
- Diuretic combinations in critically ill patients with respiratory failure:A systematic review and meta-analysis