Anti-fibrotic effect of adipose-derived stem cells on fibrotic scars
2022-06-02SophieVandersticheleJanJeroenVranckx
Sophie Vanderstichele,Jan Jeroen Vranckx
Sophie Vanderstichele,Master in Medicine,KUL Leuven University,Leuven 3000,Belgium
Jan Jeroen Vranckx,Department of Plastic,Reconstructive Surgery,KU-Leuven University Hospitals,Leuven 3000,Belgium
Abstract BACKGROUND Sustained injury,through radiotherapy,burns or surgical trauma,can result in fibrosis,displaying an excessive deposition of extracellular matrix(ECM),persisting inflammatory reaction,and reduced vascularization.The increasing recognition of fibrosis as a cause for disease and mortality,and increasing use of radiotherapy causing fibrosis,stresses the importance of a decent anti-fibrotic treatment.AIM To obtain an in-depth understanding of the complex mechanisms underlying fibrosis,and more specifically,the potential mechanisms-of-action of adiposederived stomal cells(ADSCs)in realizing their anti-fibrotic effect.METHODS A systematic review of the literature using PubMed,Embase and Web of Science was performed by two independent reviewers.RESULTS The injection of fat grafts into fibrotic tissue,releases ADSC into the environment.ADSCs’ capacity to directly differentiate into key cell types(e.g.,ECs,fibroblasts),as well as to secrete multiple paracrine factors(e.g.,hepatocyte growth factor,basis fibroblast growth factor,IL-10),allows them to alter different mechanisms underlying fibrosis in a combined approach.ADSCs favor ECM degradation by impacting the fibroblast-to-myofibroblast differentiation,favoring matrix metalloproteinases over tissue inhibitors of metalloproteinases,positively influencing collagen organization,and inhibiting the pro-fibrotic effects of transforming growth factor-β1.Furthermore,they impact elements of both the innate and adaptive immune response system,and stimulate angiogenesis on the site of injury(through secretion of pro-angiogenic cytokines like stromal cell-derived factor-1 and vascular endothelial growth factor).CONCLUSION This review shows that understanding the complex interactions of ECM accumulation,immune response and vascularization,is vital to fibrosis treatments’ effectiveness like fat grafting.It details how ADSCs intelligently steer this complex system in an anti-fibrotic or pro-angiogenic direction,without falling into extreme dilation or stimulation of a single aspect.Detailing this combined approach,has brought fat grafting one step closer to unlocking its full potential as a non-anecdotal treatment for fibrosis.
Key Words: Fibrosis;Fat grafting;Adipose-derived stem cells;Angiogenesis;Anti-fibrotic effect;Immunomodulation
lNTRODUCTlON
Fibrosis,or scarring,is a potential consequence of a dysregulated wound-healing process.Tissue injury triggers wound-healing,a complex dynamic process characterized by four distinct but overlapping phases,all limited in time:homeostasis,inflammation,proliferation and remodeling.Interference of the immune system,deposition of the extracellular matrix(ECM)and alteration of the vascularization are indispensable and,typically,reversible elements of the wound-healing.However,sustained injury results in reduced vascularization,persisting inflammatory reaction and excessive deposition of ECM,inducing fibrosis[1].Radiotherapy-induced skin fibrosis(RISF),a late cutaneous side effect of external radiation,is an example of chronic tissue injury leading to fibrosis.RISF is often characterized by pain,limited range of motion,tissue contraction and aesthetic deformation.All result in a significant loss of quality of life for patients.
Fibrosis can affect nearly every tissue in the body leading to common diseases such as idiopathic pulmonary fibrosis,cirrhosis,renal fibrosis,myocardial fibrotic remodeling,fibrotic stricture as a common complication of Crohn’s disease,and scar contractions after surgery,burns,trauma and radiotherapy.The increasing recognition of fibrosis as a cause for disease and mortality and the increasing use of radiotherapy,stresses the importance of a decent anti-fibrotic treatment[2].
In the early 20thcentury Hedrick,Zuket al[3,4],reported the presence of adipose-derived stem cells(ADSCs),or adipose-derived stromal cells within adipose tissue obtained by lipoaspiration,the socalled stromal vascular fraction(SVF).Decades before,fat grafting was already used in reconstructive procedures as filler of defects,albeit without much confidence since this transfer of fat lobules occurred without intrinsic vascularization.Colemanet al[5]pioneered in making the fat graft aliquots soluble and performing the fat transfer as tiny liquid parcels of lipoaspirate,thus eliminating the need for vascularized transfer.
The discovery of ADSCs in ‘ordinary’ fat grafts was revolutionary in stem cell research,since it was assumed previously that stem cells resided mainly in embryonic tissues,placenta and bone marrow of the adult patient[3,4].The option of obtaining large numbers of mesenchymal stem cells from lipoaspirates meant a significant paradigm change.Moreover,nowadays ADSCs can be reprogrammed[6,7].Induced pluripotent stem cells,derived from skin or blood cells,that have been reprogrammed back into an embryonic-like pluripotent state,enable the development of an unlimited source of any type of human cell required for therapeutic strategies[8,9].
Considering the fact that the SVF from fat grafts is easily accessible by lipo-aspiration,multipotent ADSCs emerged as attractive alternatives for soft tissue restoration and regeneration by adding cells,growth factors and active molecules to the microenvironment of the wound[10,11].
Plastic surgeons observed that fat grafting had a smoothening effect on scars and even on radiationinduced fibrosis.The application of fat grafting extended on various types of fibrosis such as Parry-Romberg syndrome,sclerodermia,dupuytren,hypertrophic scarsetc.,A multitude of reports confirm these observations[12,13].However,the mechanisms underlying these fibrosis-reducing effects of fat grafts remain unclear so far.
The goal of this review is to elucidate the potential mechanisms of action of fat grafting,and more specifically of ADSCs,in hostile environment.Why can fat grafts turn the sclerotic environment after intense radiotherapy,burns or surgical trauma into a soft zone that can be further restored and reconstructed? In doing so,this review aims to complement existing literature by delivering an integrated approach to explain the positive effect of ADSCs on fibrosis,considering all 3 main fibrotic aspectsi.e.,ECM accumulation,innate and adaptive immune response and vascularization.It aims at acknowledging the complexity and reciprocal impact these aspects have,both from a clinical as well as a molecular point of view.While available literature so far only focused on a single one of these aspects,the question remains whether an integrated approach and explanation on these combined levels could improve the effectiveness and application areas of this treatment.
MATERlALS AND METHODS
A systematic review of the literature using PubMed,Embase and Web of Science was performed by two independent reviewers.Terms applied to the search included fat grafting,lipofilling,adipose tissue transplantation/transfer,adipose-derived stem cell,adipose-derived stromal cell,fibrosis,scar,keloid,radiation-induced skin fibrosis,myofibroblast,fibroblast,collagen,regenerative medicine,tissue engineering,immunomodulation,neovascularization and angiogenesis modulating agents.Inclusion criteria included animal studies,randomized controlled trials,case-control studies and reviews that were relevant for elucidating the anti-fibrotic effect of ADSCs,applied to multiple features of fibrosis(e.g.,dermal fibrosis after radiotherapy,hypertrophic scars,burns,sclerodermia)Exclusion criteria comprised of articles solely about clinical outcome measures,case reports,case series and literature focused on the technique of fat grafting.Language has been restricted to English.A structured summary of the review process is illustrated in Figure 1.
RESULTS
Mechanisms leading to fibrosis
Introduction and histology of fibrosis:Fibrosis is caused by a dysregulation of regular wound-healing(mostly through sustained injury),leading to an excessive deposition of ECM,persisting inflammatory reaction and reduced vascularization.
ECM is a non-cellular three-dimensional molecular network composed of proteins(e.g.,collagen,elastin,laminin,fibronectin)and ground substance(e.g.,glycosaminoglycans,such as hyaluronan and proteoglycans)[14-16].The ECM regulates tissue development and homeostasis and constantly undergoes remodeling.Excessive accumulation of ECM components,such as collagens,fibronectin,proteoglycans,glycosaminoglycans and laminin are the typical characteristics of fibrosis regardless of the etiology[17].Although all the beforementioned ECM components participate in the overall pathogenic process,collagen type I,collagen type III and fibronectin are the most dominating proteins found in fibrotic tissue[1,2].Despite the fact that there is an increase in the amount of ECM,some ECM components(such as decorin)are less abundant in scars[13].Besides the increase of ECM accumulation,fibrosis is also defined by a high amount of alfa-smooth muscle actin(α-SMA).
Microscopically,scar tissue(e.g.,after radiation)is characterized by flattening of the rete ridges,a thickened epidermis and dermis,and an irregular collagen organization(see Figure 2).Excessive proliferation of keratinocytes causes the epidermal thickening,while it is the excessive ECM that causes the thickened dermis.The abnormal collagen behavior displays itself in an increase in the number of collagens,altered fiber thickness,more cross-linking as well as a decreased degree of collagen organization[18].
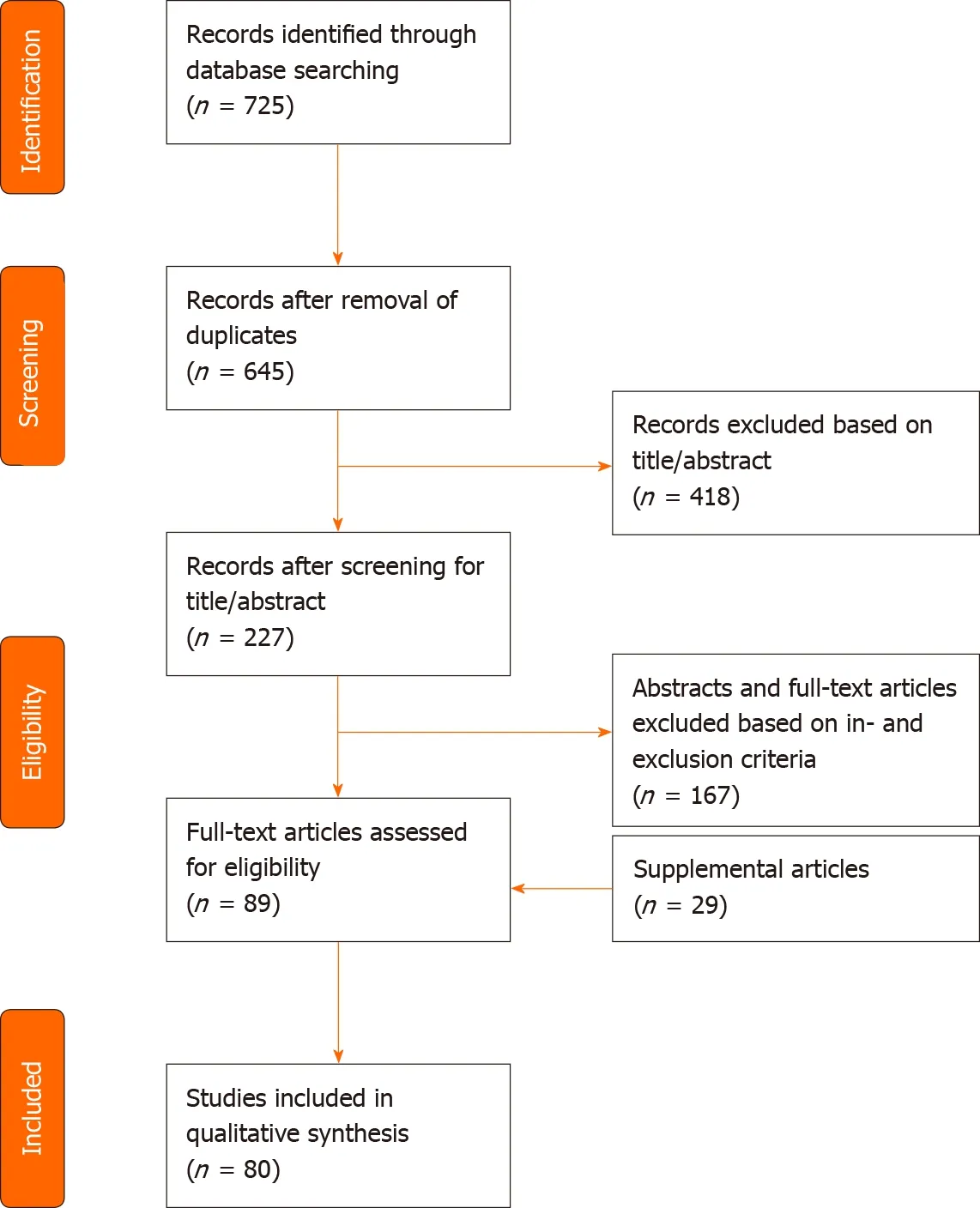
Figure 1 PRlSMA flow diagram of search strategy and study selection.
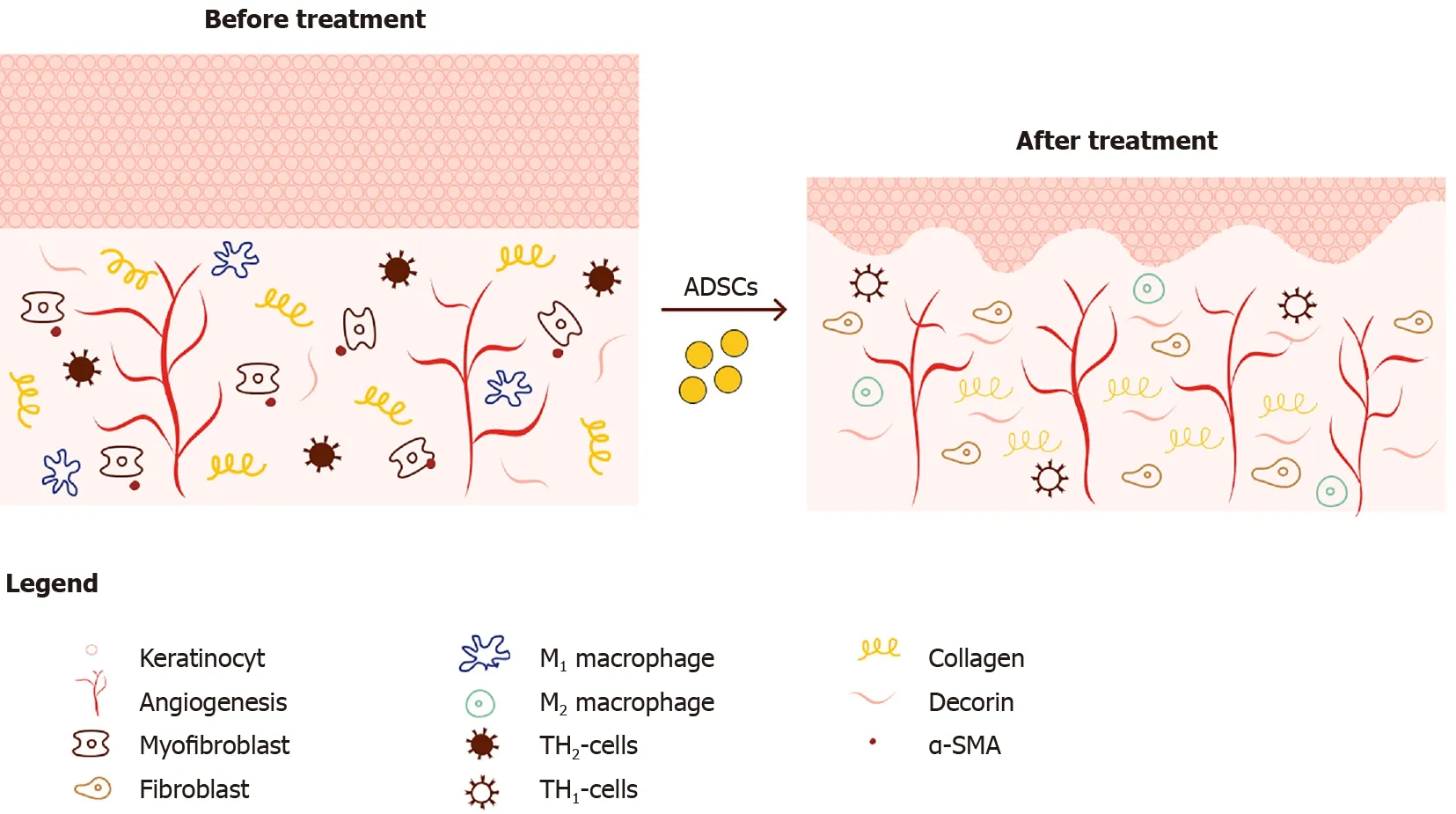
Figure 2 Schematic overview of histological changes in dermal scars before and after treatment with ADSC’s.
Histological patterns do not only reflect the increased ECM deposition but also the enhanced inflammation and reduced vascularization,through decreased vessel density,microvascular obliteration and abnormal vascularization patterns[12].
ECM accumulation
The homeostasis of the ECM is a well-regulated process influenced by a variety of actors and is subject to four major delicate balances.In fibrosis these balances are dysregulated,favoring deposition over degradation which results in overproduction of ECM.
Imbalance between fibroblasts and myofibroblasts:Fibroblasts play a crucial role in tissue homeostasis by regulating the ECM,which is constantly being synthesized,degraded and remodeled[19].However,when fibroblasts can no longer coordinate this meticulous cross talk and interplay of cells and factors in an environment of chronic inflammation or repeated tissue damage,they transform into professional repair cellsi.e.,myofibroblasts.Myofibroblasts do not typically appear in healthy connective tissue[20].Myofibroblasts produce large amounts of ECM and are capable of contraction,due to the expression of α-SMA[21].Juhlet al[19]found that cytokines and growth factors such as interleukin 6(IL-6),platelet-derived growth factor,and transforming growth factor-beta 1(TGF-β1)facilitate a prolonged myofibroblast activation,which results in excessive ECM production manifested as fibrosis.
Imbalance between TIMPs and MMPs:Fibrotic tissue can be characterized by a decreased matrix metalloproteinase(MMP)/tissue inhibitors of metalloproteinases(TIMPs)ratio resulting in ECM accumulation.ECM degradation enzymes called MMPs,vstheir opposing tissue inhibitors known as TIMPs also play a role in ECM remodeling.MMPs are endopeptidases,mainly produced by macrophages(12),and are categorized by their substrates and structure,into collagenases,gelatinases(MMP-2 and MMP-9),stromelysins,membrane-type-MMPs and others.
Zhaoet al[2]show that fibrillar collagen,the pre-dominant structural protein in fibrotic tissue,is cleaved by MMP1,MMP8,MMP13,MMP14,MMP16,and MMP18,allowing other MMPs such as gelatinases(MMP2 and MMP9),to further degrade collagen(see Figure 3).Several mice studies confirm the relation of a certain MMP-deficiency or -stimulation with development of fibrosis or protection against fibrosis,respectively[12,22,23].The opposite is applicable for TIMPs;TIMP upregulation has been associated with fibrosis[24].This general classification however does not seem to be valid for all MMP and TIMP subtypes.The role of MMP-2 and MMP-9 is for example less clear,and MMP-9 has been associated with pro-fibrotic characteristics[25].
TGF-β1 and plasminogen activator inhibitor 1(PAI1)are major regulators of the MMP and TIMP expression[26,27].The persistent activation and/or production of PAI1,resulting in MMP inhibition,directly stimulates fibrosis(see Figure 3).TGF-β1 also decreases the MMP/TIMP ratio,as will be further detailed in ‘Imbalance between multiple functions of TGF-b1 in regular vs hypertrophic scarring’.Fibroblasts derived from several fibrotic conditions such as keloid scars and scleroderma have demonstrated elevated levels of PAI1[27,28].On the contrary,PAI1 deficiency protects mice from bleomycin induced lung fibrosis[27].Taken together,upregulation of PAI1 substantially contributes to fibrosis.PAI1 is upregulated by TGF-β1,IL-1b,hypoxia and others.Ghoshet al[27]suggest that the increase of PAI1 Levels in fibroblasts from patients with scleroderma is linked to the activation of TGFβ 1/ SMAD axis.
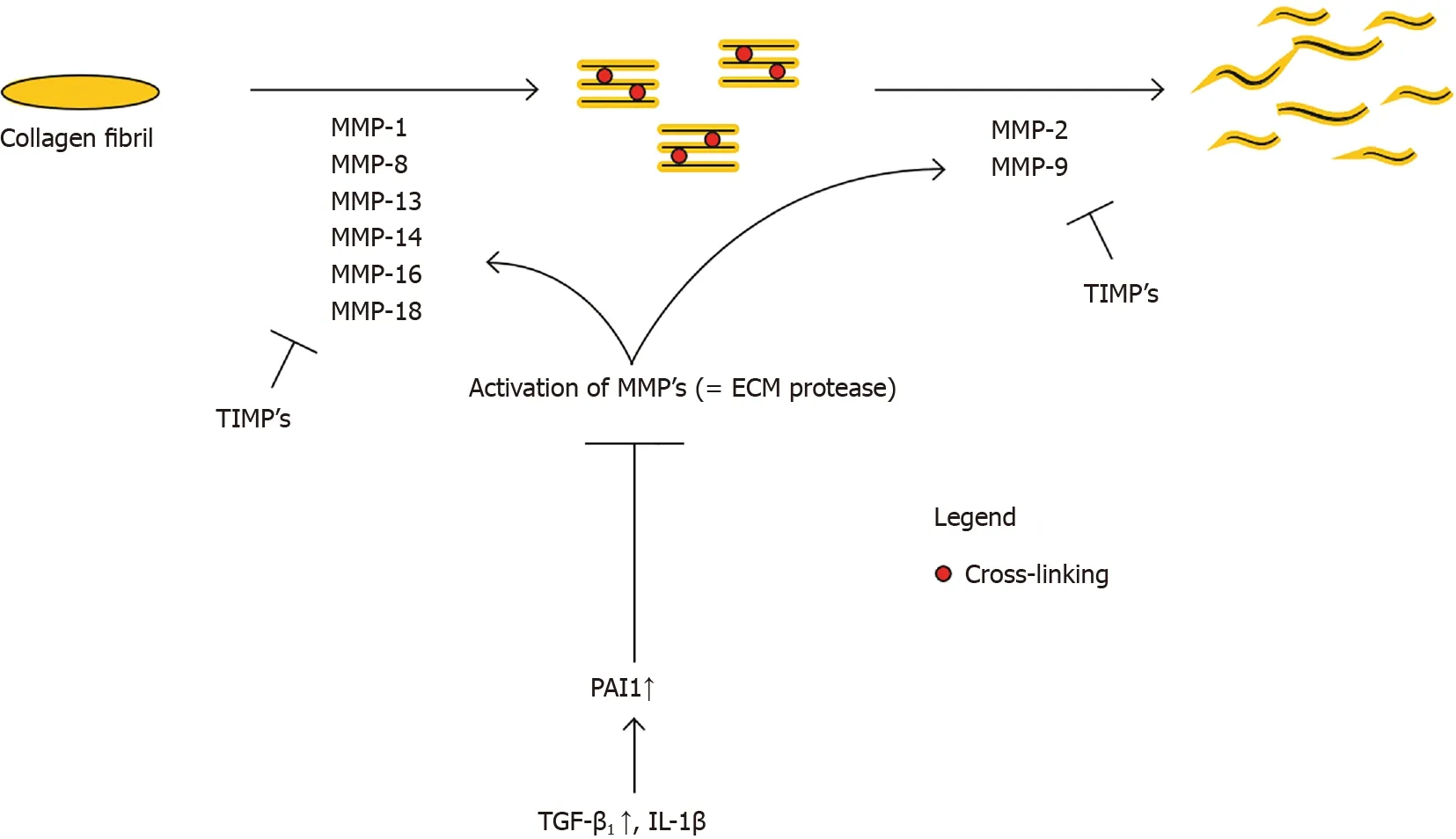
Figure 3 Collagen degradation.Collagen type 1 and type 3 are the predominant collagen types in fibrosis.ECM homeostasis requires a balance between collagen production and collagen degradation.MMPs manage the collagen degradation,while TIMPs inhibit MMPs,therefore inhibiting degradation.MMPs need activation,which is inhibited by PAI1.So,when TGF-β1 increases,PAI1 renders more inhibition of MMPs activation,therefore inhibiting ECM turnover/ remodeling and increasing fibrosis.MMP:Matrix metalloproteinase;TIMP:Tissue inhibitor of metalloproteinase;TGF-β1:Transforming growth factor beta;IL-1β:Interleukin-1β;PAI1:Plasminogen activator inhibitor 1.
Imbalance between organized and unorganized collagen fibers:Collagen organization can also influence the ECM balance through the extent in which they are cross-linked.Multiple fibrotic organ types show that crosslinking is disproportionately present and contribute to decreased ECM degradation and increased tissue stiffness[2].Thus,fibrosis is characterized by favoring unorganized and cross-linked collagen,over normal collagen organization.
Imbalance between multiple functions of TGF-β1 in regular vs hypertrophic scarring:Continuous activation of TGF-β1/Smad axis has been reported to mediate the excessive production of ECM without appropriate remodeling.In a study by Juhlet al[19],TGF-β-treated human dermal fibroblasts showed an increase in collagen I,fibronectin gene and protein levels.They also observed a gene-upregulation of α-SMA,type III,IV and V collagen,fibronectin and TGF-β1 genes,while type VI collagen was downregulated.In experimental animal studies,constitutive activation of TGF-β1 signaling leads to organ fibrosis,while inhibition of TGF-β1 reduces fibrosis[29].
The pro-fibrotic feature of TGF-β1 is multifactorial.TGF-β1 signaling stimulates directly the ECM accumulation by increasing the synthesis of ECM components such as collagen,fibronectin,elastin,proteoglycans,fibrillin and laminin[2].TGF-β1 also enhances ECM production indirectly by inhibiting MMPs and stimulating TIMPs[26].TGF-β1 induces fibroblast-to-myofibroblast differentiation,which results in the secretion of additional ECM components and which facilitates tissue contraction[2].The entire TGF-β1 pathway promotes collagen cross-linking and leads to increased rigidity and decreased ECM degradation.The main sources of TGF-β1 production are fibroblasts and activated immune cells such as macrophages.Both of these are reciprocally upregulated by the presence of TGF-β1 creating a positive 2ndorder TGF-β1 production loop.
The TGF-β1/Smad axis is also critical in regular wound healing,exerting influence on both the inflammation and revascularization processes.TGF-β1 increases inflammation by drawing neutrophils and monocytes to the injury environment and stimulates the differentiation of monocytes into activated macrophages[30].However,TGF-β1 may also induce anti-inflammatory effects[31,32].This duality may be explained by its double origin(from macrophages or T-cells)[31]or by the distinctive temporal expression patterns during the sequential phases in wound repair[30].
Role of the innate and adaptive immune response in fibrosis
Aside from ECM accumulation,fibrosis is also driven by persistent low-grade inflammation,sustained by both the innate and adaptive immune response[31].Multiple mechanisms lead to this increased or prolonged inflammation.
The first mechanism is governed by an increase of pro-inflammatory cytokines.Adipocytes,in a stress situation(e.g.,radiotherapy),synthesize pro-inflammatory proteins such as tumor necrosis factorα(TNF-α),IL-6 and IL-8[33].IL-6 also has pro-fibrotic features by persistent stimulation of fibroblasts,which may lead to the differentiation into myofibroblasts[19].Furthermore,various innate inflammatory cells(e.g.,macrophages,neutrophils,mast cells and eosinophils)secrete a multitude of growth factors and cytokines,such as TNF-α,IL-1β.Studies by Miyazakiet al[34]and Kolbet al[35]found that mice who overexpress TNF-α or IL-1β in the lung,develop pulmonary fibrosis.In turn,TNF-α and IL-1β also increase expression of IL-6[31].
The second mechanism that leads to prolonged inflammation isviamacrophages.Macrophages are vital in the wound healing process.However,redundant infiltration,overactivation,lack of differentiation and lack of clearance result in fibrotic tissue formation[18,36].This pro-fibrotic activity manifests itself mostly in the early phases of the wound-healing process and results in the production of inflammatory mediators that can aggravate tissue injury,such as TNF-α,IL-1β,and a variety of toxic mediators,such as reactive oxygen and nitrogen species.Moreover,macrophages are known to produce the pro-fibrotic TGF-β1.Duffieldet al[37]reported that early macrophage depletion effectively reduced the development of liver fibrosis in mice.Wynnet al[31]showed that limiting the pro-inflammatory activity of innate myeloid-lineage cells(incl.macrophages)may successfully treat fibrotic diseases.In later stages of the wound-healing process,a subset of macrophages convert into a suppressive phenotype and express multiple anti-inflammatory mediators(e.g.,IL-10,Arg1,Relm-α,…)that direct the resolution of the inflammatory response[38].
Furthermore,one can distinguish anti-inflammatory/pro tissue repair macrophages(M2)from proinflammatory/pro-fibrotic(M1)macrophages[39].Thus,the balance between both types also plays a role in the pathogenesis of fibrosis.Multiple studies[40,41]observed that M2 macrophages suppress fibrosis and reduce inflammation by competing with T-helper 2(TH2)cells and fibroblasts for larginine.This competition reduces the TH2 response and suppresses collagen synthesis by myofibroblasts[31].Furthermore,literature[38]indicates that M2 cells are important inducers of regulatory Tcells,that have an anti-fibrotic effect.
It seems useful to target the inflammatory cascade and the innate immune response,to treat fibrotic disorders.However,the extent of fibrosis is not per se linked with the severity of inflammation,which suggests that other immunological mechanisms,such as the adaptive immune response,play an important role in the fibrotic process.Wynn[42]described how the TH1/TH2 paradigm seems to play a key role in sustaining the immune response.There are 3 types of T helper cells;TH1 CD4+ T cells,TH2 CD4+ T cells and regulatory T cells.This categorization is based on the cytokines each of these cells secrete.
TH1 cells are predominant in the initial response of the adaptive immune system to chronic injury.TH1 cells mainly secrete interferon-γ(IFN-γ)and IL-12,as well as associated pro-inflammatory cytokines.The TH1 responses are pro-inflammatory yet anti-fibrotic.They directly inhibit collagen production by fibroblasts,stimulate ECM degradation by favoring MMPs over TIMP and inhibit TGF-b1 production[43].Moreover,they indirectly inhibit fibrosis by reducing pro-fibrotic cytokine expression by TH2 cells(e.g.,IL-13)[44].
However,when the stimulus persists,TH2 cells and regulatory T cells collaborate to suppress the TH1 response to prevent the immune system from causing additional damage.In their response,TH2 cells mainly secrete IL-4,IL-5 and IL-13[44].These factors stimulate fibrosis by enhancing collagen deposition through various mechanisms.On top of that,IL-13 specifically strengthens the pro-fibrotic TGF-β1-SMAD mechanism,while also independently stimulating collagen production by fibroblasts[45-48].Therefore,despite TH2’s facilitating function in wound healing,their response contributes to fibrosis.Specifically applied to post-irradiation fibrosis,Buttneret al[49]showed the increased concentrations of IL-4.
At last,the regulatory T-cells mainly secrete IL-10,which is anti-fibrotic by directly suppressing collagen synthesis by fibroblasts,and cooperates with TH1 cytokines to suppress collagen deposition[50-52].
Reduced vascularization
Radiation injury on the skin is characterized by microvascular obliteration and poor revascularization.The reduced vascularization results in diminished transport of oxygen,nutrients and essential factors of the immune system to the damage tissues.In the end,this may lead to the deterioration of the hypoxia,resulting in fibrosis.
DlSCUSSlON
Anti-fibrotic effect of ADSCs on scar tissue by fat grafting
Histological changes mediated by ADSCs on scar tissue:When injecting ADSCs into a fibrotic injury environment through fat grafting,multiple histological changes occur(see Figure 2).A restoration of the normal skin ridge pattern is observed.Several animal models[23,53]andin vitromodels[12,54]show a decrease in ECM components’ deposition such as collagen I,collagen III,fibronectin and elastin.The expression of α-SMA,SMAD-3 proteins and TGF-β1 seems to be decreased while the amount of decorin and MMP-1/TIMP-1 ratio is increased[12].Furthermore,Zonariet al[55]and Zhanget al[53]show improved collagen fiber alignment,organization and less cross-linking.One can also distinguish a decrease in pro-inflammatory mediators/profibrotic factors(e.g.,IL-6,IL-8,connective tissue growth factor)[12].Finally,an increase in vascularization and a normalization of the microvascular architecture is observed[13].
This histological overview is however not exhaustive.Multiple other factors and substances are impacted by the insertion of a fat graft,which will be further described through the impact they have on the key molecular balances of fibrosis.
Anti-fibrotic effect through ADSCs
The antifibrotic potential of ADSC can be exerted in a direct or indirect fashion.
ADSCs as multipotent progenitor cells:ADSCs are multipotent progenitor cells that have the intrinsic possibility to differentiate into various sorts of cells that play a role in the wound-healing process(e.g.,fibroblasts,keratinocytes,osteocytes,neural cells,endothelial cells,etc.).These ADSC cell products can in turn cause tissue regeneration and cell restoration[7].ADSCs can also differentiate into mature adipocytes and serve as building blocks for a subcutaneous adipose layer that adds elasticity and pliability to the skin and volume required for thermoregulation.Adipogenesis is key for the effectiveness of ADSCs/fat grafts as it preserves the necessary fat tissue[33].
Paracrine:Moreover,ADSCs produce a myriad of trophic factors,which influence the formation and modulation of the ECM,and interact with the immune response and angiogenesis[7,13,30,32](see Figure 4).
Interference with excessive ECM formation
Influence on fibroblast to myofibroblast differentiation:Studies show that gene expression of the profibrotic marker α-SMA,produced specifically by myofibroblasts,is decreased upon administration of ADSCs[23,53,55,56].Borovikovaet al[30]describe multiple mechanisms:ADSCs inhibit the fibroblast-tomyofibroblast differentiation by secreting hepatocyte growth factor(HGF),IL-10 and p53.ADSCs also stimulate myofibroblast apoptosis by the secretion of basis fibroblast growth factor(bFGF)viathe Rho/Rho kinase pathway and HGFviathe FAK-extracellular signal-regulated kinase(ERK)-MMP signaling pathway.FGF is also reported to reverse the myofibroblast phenotype through its activation of ERK/MAP kinase pathway.
MMP vs TIMP balance:The administration of ADSCs by lipofilling has an antifibrotic effect by modulating MMP/TIMP ratio by various pathways(see Figure 5).
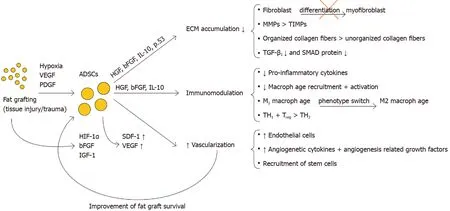
Figure 4 Main mechanisms of adipose-derived stromal cells antifibrotic action and their most important paracrine factors.VEGF:Vascular endothelial growth factor;PDGF:Platelet-derived growth factor;ADSCs:Adipose-derived stromal cells;HGF:Hepatocyte growth factor;bFGF:Basic fibroblast growth factor;IL-10:Interleukin-10;HIF-1β:Hypoxia-inducing factor-1β;IGF-1:Insulin-like growth factor-1;MMP:Matrix metalloproteinase;TIMP:Iissue inhibitor of metalloproteinase;TH1:T helper 1 cells;TH2:T helper 2 cells;Treg:Regulatory T cells.
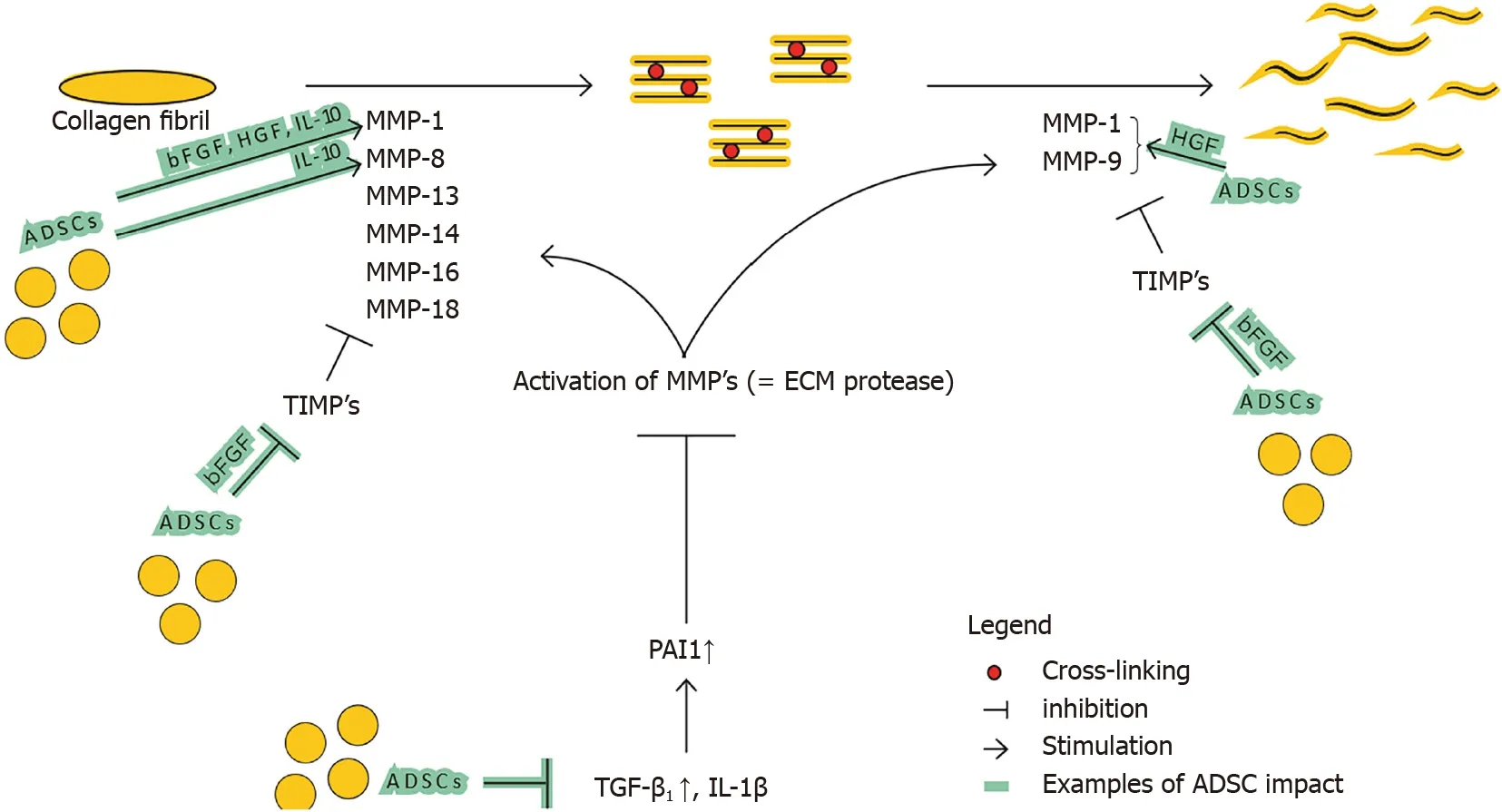
Figure 5 lmpact of adipose-derived stromal cells on matrix metalloproteinase and tissue inhibitor of metalloproteinase balance.ADSCs:Adipose-derived stromal cells;MMP:Matrix metalloproteinase;TIMP:Tissue inhibitor of metalloproteinase;TGF-β1:Transforming growth factor beta;IL-1β:Interleukin-1β;PAI1:Plasminogen activator inhibitor 1;HGF:Hepatocyte growth factor;bFGF:Basic fibroblast growth factor;IL-10:Interleukin-10.
Denget al[12]show that ADSCs enhance ECM degradation by increasing MMP-1/TIMP-1 ratio.On top of that,Spiekmanet al[54]show that ADSCs promote the expression of MMP-1,MMP-2 and MMP-14.Presumably ADSCs enhance the ratio in favor of degradation by decreasing the major regulator of MMP and TIMP expression,TGF-β1.Decreased SMAD signaling also decreases the other crucial director,PAI1 which in turn results in MMP activation.Furthermore,ADSCs secrete HGF,which activates MMP-1,MMP-2 and MMP-9[57,58].ADSCs also produce bFGF and IL-10 that influence the ratio significantly.IL-10 does this by increasing MMP-1 and MMP-8,and bFGF presumably by increasing MMP-1 and decreasing TIMP-1 expression[59-61].bFGF also stimulates HGF production,strengthening the said HGF effect.
Finally,not all MMPs and TIMPs will necessarily have a singular effect(e.g.,increase of MMP-9 can in certain circumstances be pro-fibroticvsthe anti-fibrotic effect of other MMPs).
Improvement of collagen linking:Zonariet al[55]and Zhanget al[53]show improved collagen fiber alignment,organization and less cross-linking when ADSCs are inserted into the fibrotic injury environment.Given that cross-linking contributes to decreased ECM degradation[2],this decreased crosslinking has an anti-fibrotic effect.
TGF-b1/Smad axis:Section‘Imbalance between multiple functions of TGF-β1 in regularvshypertrophic scarring’ described the pro-fibrotic feature of the TGF-β1/Smad axis,through its multifactorial influence on the key mentioned balances leading to ECM accumulation,and thus fibrosis.Studies by Zonariet al[55],Uysalet al[56]and Spiekmanet al[54],report that ADSCs decrease the presence of TGF-β1 as well as SMAD 2 and SMAD 3 proteins.An effect possibly contributing to this is given by Ejazet al[62],who in their study describe a downregulation of TGF-β1 as a result of increased concentrations of HGF(also secreted by ADSCs).In turn,decreased TGF-β1 reduces ECM accumulation both through its direct as well as indirect effects(by reducing myofibroblast activation,favoring MMPs over TIMPs and decreasing collagen cross-linking),all mitigating fibrosis.
For completeness on ADSC impact,one can mention the impact of another member of the TGF-β cell group,i.e.,TGF-β3.Impacting the TGF-β1/TGF-β3 balance towards increasing TGF-β3,is linked to reduced scar formation in adult wound healing[30].Multiple studies[23,55,63]have shown such an increase of TGF-β3 in fibrotic tissue after injection of ADSCs,resulting in decreased tissue stiffness.
Immunomodulation:The anti-fibrotic effect of ADSCs through their impact on elements of both the innate and adaptive immune response,has multiple facets.
ADSCs downregulate key pro-inflammatory cytokines.Carcelleret al[64]indicates that,in anin vivomouse model,ADSCs effectively suppress the inflammatory response through the downregulation of selected inflammatory mediators(e.g.,IL-1b,TNF-α,IL-6,leukotriene B4).A similar effect of ADSCs could be seen through their secretion of HGF,which is documented to lead to a decrease of pro-inflammatory cytokines(TNF-α,IL-12,monocyte chemoattractant protein 1,IFN-g)in a fibrosis model[30].Also,ADSCs have the potency to modulate macrophage recruitment and activation,mostly by secreting bFGF,HGF and IL-10[30].Kotaniet al[32]show that ADSCs induce apoptosis of activated macrophages,and reduce infiltrations of macrophages,neutrophils and T lymphocytes.Therefore,through their immunomodulatory ability,ADSCs have an inhibitory effect on active macrophages.Moreover,Xieet al[65]showed that ADSCs promote a macrophage phenotype switch,favoring the anti-inflammatory M2 phenotype over the pro-inflammatory M1 in a mouse model.
Finally,ADSCs exhibit a suppressive effect on lymphocyte responses and induce a phenotypic conversion of T-cells.Kotaniet al[32]describes,in the context of pulmonary fibrosis,that ADSCs inhibit the differentiation and proliferation of Th2-type mCD4+ T cells while promoting this for regulatory T cells.Given the pro-fibrotic effect of TH2-cells(see section ‘Role of the innate and adaptive immune response in fibrosis’),this could suggest the phenotypic conversion of T cells as an important mechanism underlying the anti-inflammatory effect of ADSCs.Choet al[66]in turn suggest that ADSCs have an inhibitory effect on inflammatory diseases either directly or by inducing T-Regulatory cells(through PGE2 and TGF-β1)and inhibiting TH2 cytokines.
Pro-angiogenic effect of fat grafting and ADSCs
Stimulating angiogenesis and revascularization has a positive effect on fibrosis.Rebuilding natural blood flow improves the delivery of supplemental oxygen and other key substances to the injury site.On top of that,angiogenesis allows for better survival of administered ADSC/fat grafts in general,enhancing beforementioned treatment effects.Evanset al[67]describe how ADSCs,like bone marrowderived mesenchymal stem cells,have the capacity to differentiate into endothelial cells(ECs),that provide the required cellular building blocks for angiogenesis.
Additionally ADSCs secrete an array of pro-angiogenetic cytokines and growth factors such as HGF,vascular endothelial growth factor(VEGF),bFGF,G-CSF,GM-CSF,IL-7,M-CSF,stromal cell-derived factor-1(SDF-1),etc.[33,68].These factors may promote the angiogenic sprouting process based on endothelial cell migration,proliferation and tube formation[69].
In response to entering a hypoxic environment,ADSCs activate hypoxia-inducing factor-1α(HIF-1α),and release bFGF and insulin-like growth factor-1(IGF-1),that in turn promote neovascularization by establishing high levels of VEGF at the graft site.This VEGF promotes EC proliferation and migration to the graft,as well as inhibits EC apoptosis[70].Studies also show[71-73]that high quantities of VEGF found at the grafting site,promote monocyte differentiation into M2 type macrophages,reducing fibrosis.On the paracrine side,increasingly more literature details the importance of SDF-1 in angiogenesis.Muroharaet al[68]states that SDF-1 Likely plays a key role in the ADSC-mediated angiogenesis.Other studies mention that SDF-1,like VEGF,improves revascularization and angiogenesis by recruiting stem cells such as endothelial progenitor cells and hematopoietic stem cells to the engrafted/ischemic site.It is reported that SDF-1/CXCR4 axis exerts one of the strongest chemotactic effects on BMSCs[74,75].
Macrophages play an important role in angiogenesis.Caiet al[76]reported that early macrophage infiltration in the graft environment appears to be key for angiogenesis and revascularization.However,when present for an extended period of time they can stimulate fibrosis.By initially releasing angiogenetic cytokines(e.g.,VEGF,bFGF),macrophages stimulate vessel growth in a VEGF-dependent manner,while also generating recruitment signals for stem cells such as ECs.On top of that,M2 macrophages are a major source of SDF-1.Through all this,the macrophages role in angiogenesis is regulated in an important,though delicate and time-sensitive balance.ADSCs influences this balance,by stimulating a phenotype switch to M2 macrophages and by inhibiting a prolonged infiltration.Further research needs to clarify the impact of ADSCs on early macrophage infiltration,possibly through M-CSF.
Finally,it must be stated that in select cases of fibrosis(e.g.,liver fibrosis),angiogenesis can have a fibrosis stimulating effect[77].This paradox indicates that the anti-fibrotic effect of ADSCs through angiogenetic stimulation,is case-dependent and remains particularly complex.
CONCLUSlON
When injected into fibrotic tissue by using fat grafts,ADSCs exert anti-fibrotic and pro-angiogenic effects by impacting multiple distinctive mechanisms.Through their capacity to directly differentiate into key cell types that influence the wound healing process,as well as secrete multiple paracrine factors(e.g.,HGF,bFGF,IL-10),they carefully alter different mechanisms underlying fibrosis.ADSCs favor ECM degradation by modifying the fibroblast-to-myofibroblast differentiation,by favoring MMPs over TIMPs,by positively influencing collagen organization,and by inhibiting the pro-fibrotic effects of TGFβ1.In addition ADSCs influence both the innate and adaptive immune response system.The proangiogenic effect of ADSCs can be categorized into direct(direct differentiation into ECs)as well as indirect effects(secreting pro-angiogenic cytokines such as stromal cell-derived factor-1 and VEGF).
Increasingly morein vitroandin vivostudies tend to focus on the development of anti-fibrotic drugs on a single aspect of fibrosis,not considering the complex interactions nor the time dependency of these mechanisms.This review has shown that the understanding of the complex interaction between ECM accumulation,immune response and vascularization,is vital for the effectiveness of treatments against fibrosis,like fat grafting.
ADSCs have the ability to interact intensivelyviamultiple mechanisms-of action.They intelligently steer multiple molecular balances in an anti-fibrotic or pro-angiogenic direction in a delicate manner.It is by these synergistic actions that ADSCs injected through fat grafts successfully soften fibrotic scars.
ARTlCLE HlGHLlGHTS
Research background
The successful anti-fibrotic effect of clinical fat grafting has been described extensively in literature.However,the mechanisms leading to fibrosis and how adipose-derived stomal cells(ADSCs)can interact with these mechanisms to reduce fibrosis,are far from clarified today.
Research motivation
Fibrosis is increasingly recognized as an important cause for morbidity and mortality.Moreover,the increasing clinical use of radiotherapy results in an enhanced incidence of severe tissue damage by fibrosis.Therefore,an efficient anti-fibrotic treatment and a thorough understanding of its mechanismofaction is mandatory.
Research objectives
The objective of this systematic review was to obtain an in-depth understanding of the complex mechanisms underlying fibrosis,and more specifically,the potential mechanisms-of-action of ADSCs in realizing their anti-fibrotic effect.
Research methods
This systematic review was conducted according to the PRISMA(Preferred Reporting Items for Systematic Reviews and Meta-Analyses)methodology.We clearly defined a set of objectives with predefined eligibility criteria.We performed a thorough and disciplined literature search to obtain all relevant studies that met the eligibility criteria.Each citation is associated with a set of Mesh terms that describe the content.
Research results
Systematic assessment of available literature was performed by two reviewers and one control to avoid bias.This process resulted in 80 references cited as reported in the PRISMA flow diagram.These references served as basic scientific platform to investigate the previously mentioned research objectives.Due to some contradictory findings in the molecular balances,we performed a supple mentary literature search trying to elucidate some of the more specific mechanisms-of-action.This review has shown that the understanding of the complex interaction between extracellular matrix(ECM)accumulation,immune response and vascularization,is vital for the effectiveness of treatments against fibrosis,like fat grafting.
Research conclusions
ADSCs have the ability to interact intensively with the healing environmentviamultiple mechanisms of action.Through their capacity to directly differentiate into key cell types that influence the wound healing process,as well as secrete multiple paracrine factors,ADSCs meticulously alter distinctive mechanisms underlying fibrosis.ADSCs stimulate ECM degradation by modifying the fibroblast-tomyofibroblast differentiation,by favoring matrix metalloproteinase over tissue inhibitors of metalloproteinases,by positively influencing collagen organization,and by inhibiting the pro-fibrotic effects of transforming growth factor-beta 1.In addition,ADSCs influence both the innate and adaptive immune response system.The pro-angiogenic effect of ADSCs exerted by direct differentiation into ECs,as well as by the secretion of pro-angiogenic cytokines such as stromal cell-derived factor-1 and vascular endothelial growth factor.ADSCs intelligently steer these molecular balances in a delicate manner.It is by these synergistic actions that ADSCs injected through fat grafts successfully soften fibrotic scars.
Research perspectives
This thorough systematic review describes the intensive and cross talk of ADSCs with surrounding cells and active molecules all having a significant effect on the outcome of fibrosis.This manuscript invites to further research to unravel the complex interactions of ADSCs and the seemingly contradictory effects depending on time and place of occurrence.
ACKNOWLEDGEMENTS
We would like to thank Prof.Opdenakker G,Professor of Microbiology and Immunology,Chairman BoD,Rega Institute,KU Leuven,for his expert opinion and guidance.
FOOTNOTES
Author contributions:The selection of articles was performed independently by both authors;Vanderstichele S conducted the systematic review,with Vranckx JJ providing scientific content and supervision;all authors have read and approved the final manuscript.
Conflict-of-interest statement:This article is not subject to any conflict of interest or financial disclosure.
PRlSMA 2009 Checklist statement:The authors have read the PRISMA 2009 Checklist,and the manuscript was prepared and revised according to the PRISMA 2009 Checklist.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:http://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Belgium
ORClD number:Sophie Vanderstichele 0000-0001-7918-9376;Jan Jeroen Vranckx 0000-0002-0920-8620.
S-Editor:Wu YXJ
L-Editor:A
P-Editor:Li X
杂志排行

World Journal of Stem Cells的其它文章
- Abnormal lipid synthesis as a therapeutic target for cancer stem cells
- Transcription regulators differentiate mesenchymal stem cells into chondroprogenitors,and their in vivo implantation regenerated the intervertebral disc degeneration
- Extracellular vesicles from hypoxia-preconditioned mesenchymal stem cells alleviates myocardial injury by targeting thioredoxininteracting protein-mediated hypoxia-inducible factor-1α pathway
- Physical energy-based ultrasound shifts M1 macrophage differentiation towards M2 state