非对称二甲基精氨酸作为血管再狭窄生物标志物的Meta分析
2021-11-10杨春卿李佳阳李意奇李光月杨丹莉程晓明吕俊远
杨春卿,李佳阳,李意奇,李光月,杨丹莉,程晓明,吕俊远
(1.菏泽市立医院 心血管外科,山东 菏泽 274000;2.遵义医科大学附属医院 临床试验机构,贵州 遵义 563099;3.遵义医科大学 基础药理教育部重点实验室暨特色民族药教育部国际合作联合实验室,贵州 遵义 563099;4.遵义医科大学附属医院 甲乳外科,贵州 遵义 563099)
Ischemic disease continues to be the leading cause of death globally and is predicted to dominate mortality trends in the future[1].Revascularization,such as vascular bypass or angioplasty,is the typical surgical means for restoration of perfusion to a body part or organ that has suffered ischemia.Excessive wound healing reaction of target vessel of revascularization could lead to lumen narrowing again what is called “restenosis”,vascular restenosis represents the main limiting factor of long-term success of revascularization procedures[2-4].Despite the establishment of guidelines for the secondary prevention,many patients still develop vascular restenosis after revascularization.For example,vascular restenosis affects up to 20% of the 1.5 million patients undergoing coronary angioplasty annually in the United States[5].Therefore,effective biomarker that can identify restenosis-prone conditions is necessary to improve the follow-up and treatment for the patients undergoing revascularization.
Asymmetric dimethylarginine (ADMA) as an endogenous inhibitor of nitric oxide synthase was characterized in the 1992 by Vallance[6].Nitric oxide synthase dysfunction disrupts vascular homeostasis and leads to vascular restenosis by promoting changes in vascular smooth muscle cell proliferation,migration and extracellular matrix production[7-8].Higher ADMA levels were observed in patients with vascular restenosis compared with those in the controls[9-12].ADMA may be independently associated with the risk of restenosis.However,an association of ADMA levels with vascular restenosis has been reported with conflicting findings[13].Therefore,we performed a Meta-analysis of all relevant studies to define the magnitude and the robustness of the relationship between ADMA concentration and restenosis.
1 Methods
1.1 Literature search A systematical search of five databases including PubMed,Embase,Web of Science (WOS),SinoMed,China National Knowledge Infrastructure (CNKI) and Wanfang Data was performed up to the date of January 31,2021.The following keywords were applied:“asymmetric dimethylarginine” or “ADMA” or “Dimethyl-L-arginine” or “(S)-2-Amino-5-(3,3-dimethylguanidino)pentanoic acid” and “restenosis” or “recurrent stenosis” or “neointimal hyperplasia” or “vascular remodeling”.The reference lists of relevant studies were manually retrieved to identify possible additional studies.
1.2 Inclusion and exclusion criteria The following selection criteria were considered in this Meta-analysis:1) Case-control study,cohort study or randomized clinical trial study; 2) Studies on the association between ADMA levels and vascular restenosis risk; 3) Information on the measurement of ADMA was obtained.If multiple publications on the same study were available,the comprehensive or latest publication was used.Studies were excluded if relevant information were unavailable.
1.3 Data extraction and quality assessment The data were independently extracted by two investigators and validated by a third investigator.The following information was extracted from each study:first author,year of publication,country,number of patients,age,mean±SD of ADMA concentration,sample type,storage temperature and assay method.The Newcastle-Ottawa scale (NOS) was used to evaluate the quality of the included studies[14].
1.4 Statistical analysis Meta-analysis was performed in STATA 12.0 (STATA Corp,College Station,TX,USA).Differences between cases and controls were calculated using the standardized mean difference (SMD) for continuous variables.These estimates and their 95% confidence intervals (CI) were illustrated by a forest plot.The Cochrane Q statistic andI2statistics were utilized to evaluate the heterogeneity across the included studies.The Cochrane Q test withP<0.10 orI2statistic >50% were defined as indicators of significant heterogeneity using a random effect model; otherwise,a fixed-effect model was applied.If there is significant heterogeneity,we conducted the sensitivity and subgroup analysis to test the source of heterogeneity.The possibility of publication bias was explored by Egger’s linear regression test[15]and Begg’s rank correlation test[16]withP<0.10 indicating statistical significance.A two-tailedPvalue below 0.05 was considered statistically significant.
2 Results
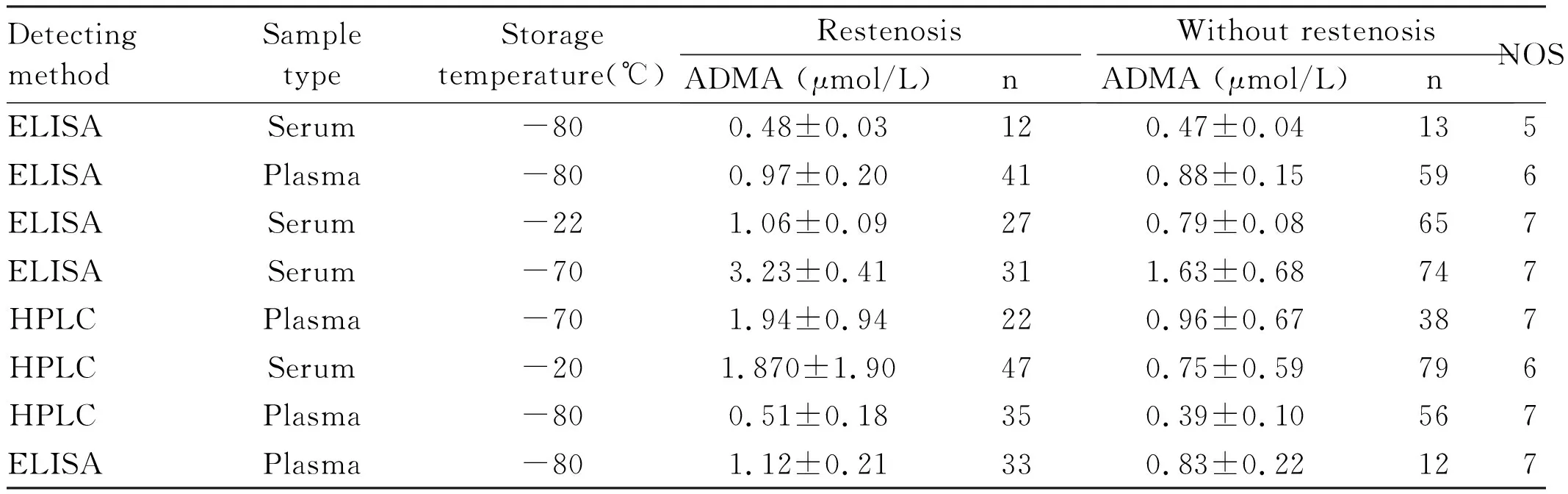
2.1 Searching results As the flow chart shown in Figure 1,a total of 382 articles were initially identified,130 articles were excluded for duplicative information and 225 articles were excluded by scanning the title and abstract.For the 27 potentially relevant studies,the full-text manuscripts were read.A total of 17 studies were excluded because not focusing on the interest and 2 studies were further excluded for not providing raw data of ADMA.Therefore,8 studies were finally eligible for this Meta-analysis,and all of them were case-control studies[9-13,17-19].The main characteristics of the included studies were summarized in Table 1.Among these 8 studies,the measurements of ADMA in 5 studies[11-13,17,18]were used enzyme-linked immunosorbent assay (ELISA),the others[9-10,19]were done by high performance liquid chromatography (HPLC).NOS scores for methodological quality of studies ranged from 5 to 7 stars,indicating moderate to good quality.

Figure 1 Flow chart showing the selection and exclusion of studies in the Meta-analysis

Table 1 Characteristics of included studies
Continued Table
2.2 ADMA andprognosis of restenosis All the included studies provided the ADMA levels in vascular restenosis patients and controls.There was significant heterogeneity among the included studies (I2=91.8%;P<0.01); thus,a random-effects model was used to combine effect size.A pooled summary shown in Figure 2,which indicated that ADMA levels in vascular restenosis patients were significantly higher compared with those in controls (SMD 1.21; 95%CI1.03-1.39;P=0.00).However,in view of the obvious heterogeneity among the included studies,subgroup analysis and sensitivity analysis were performed to dissect the heterogeneity.
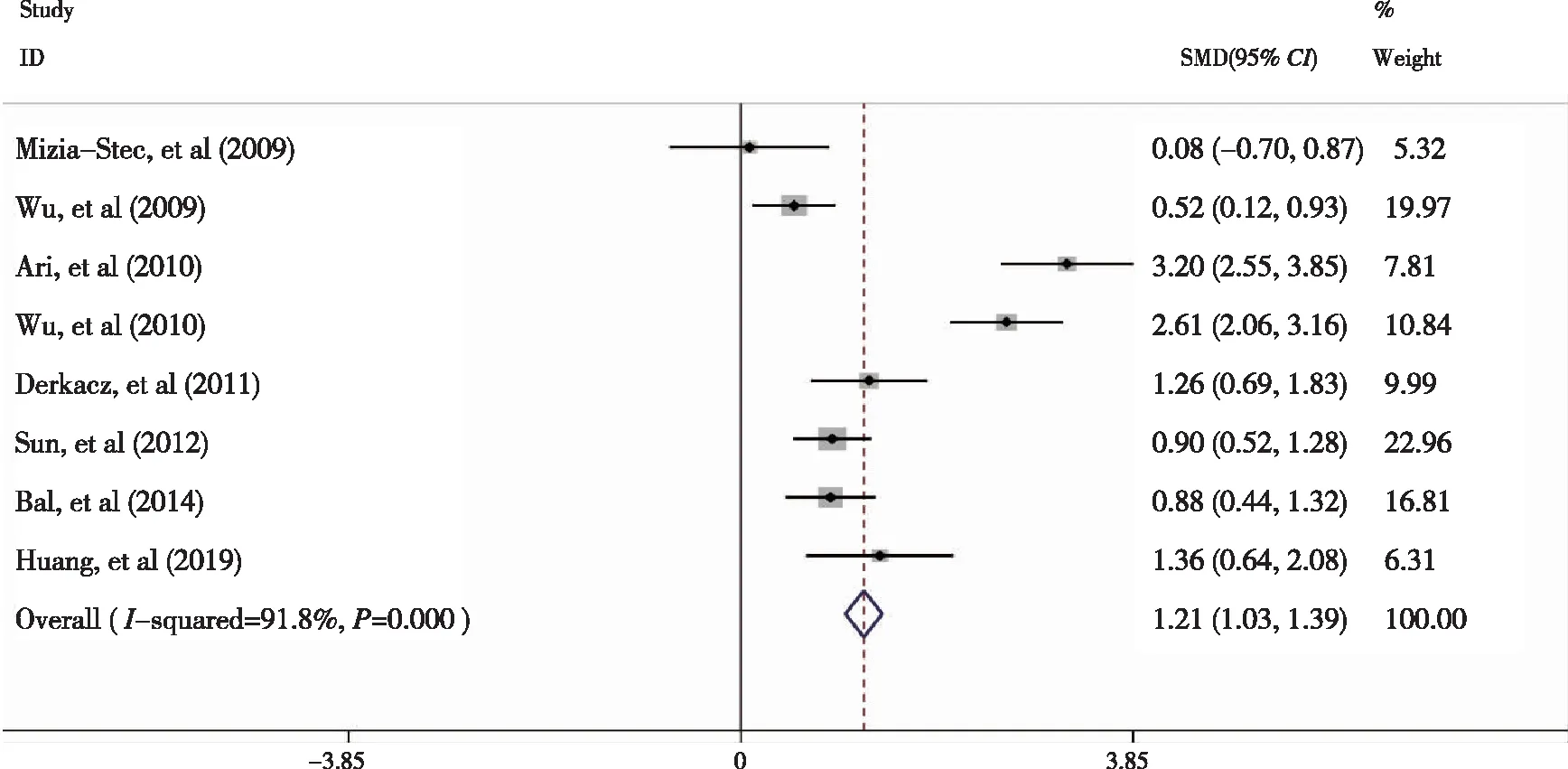
Figure 2 Forest plots of standard mean diference (SMD) with 95% confidence intervals of ADMA levels in patients with restenosis and those in controls
2.3 Sensitivity analysis and subgroup analysis Sensitivity analysis showed that the effect size was not modified when any single study was in turn removed (Figure 3).Sensitivity analysis failed to find the source of heterogeneity; the subgroup analyses were further performed according to measurement methods.ADMA levels and vascular restenosis risk based on measurement methods ADMA levels in the five eighths of studies[11-13,17-18]were detected by ELISA,while the others[9-10,19]were measured by HPLC.As shown in Figure 4,there was significant heterogeneity in the studies which used ELISA (I2=94.80%;P<0.01).Interestingly,no heterogeneity was observed in the studies measured by HPLC (I2=0.00%;P=0.53).Even though heterogeneity was always higher for ELISA in comparison to HPLC tests,the results from both approaches were consistent (Figure 4).

Figure 3 Sensitivity analysis of studies examining ADMA concentrations after revascularization
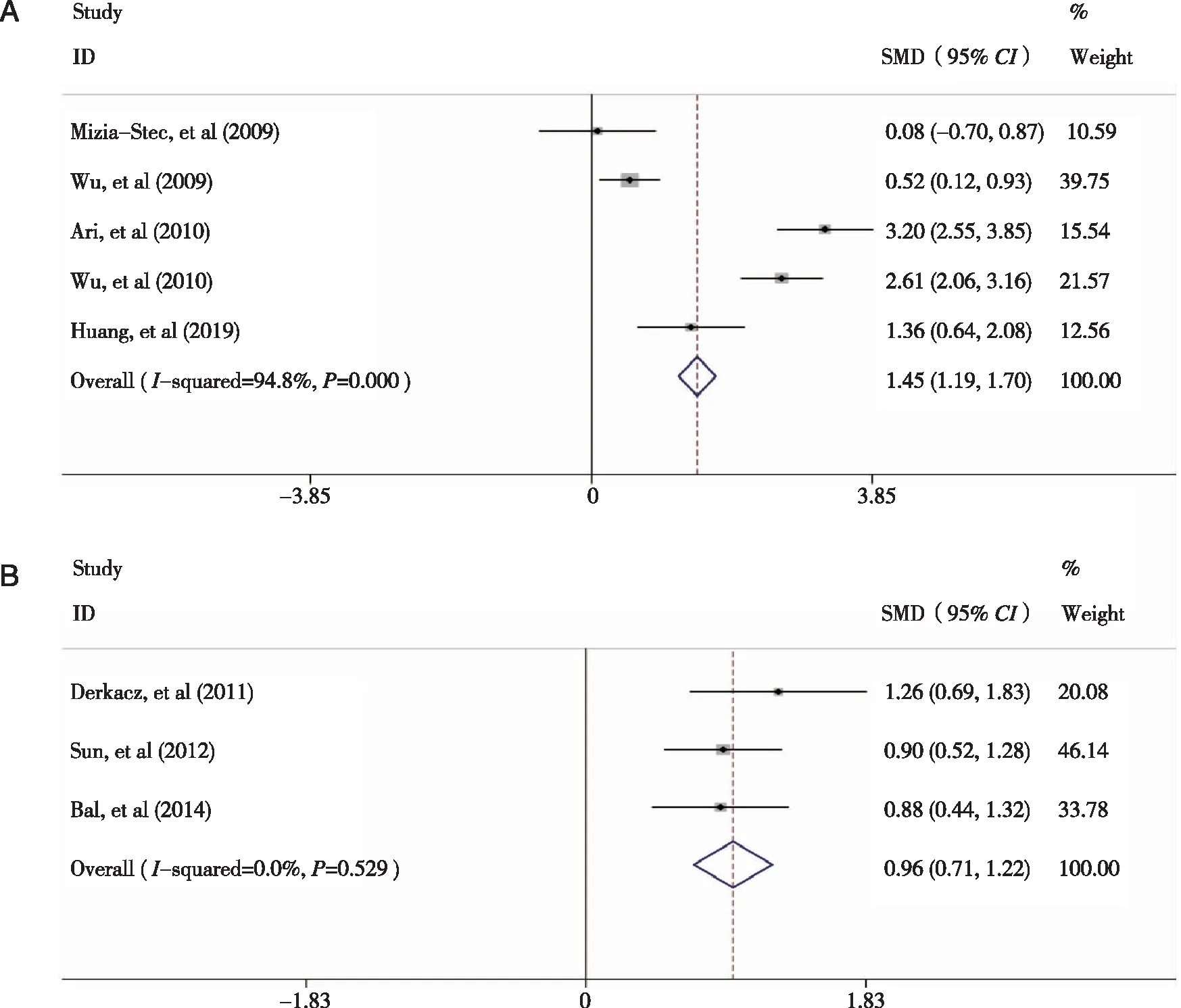
Forest plots for SMDs of ADMA levels with restenosis acquired from the involved studies using( A:ELISA ; B :HPLC).Figure 4 The subgroup analyses based on measurement methods
2.4 Publication bias Evidence of publication bias was not observed in theBegg's rank correlation test (P= 0.38; Figure 5A) and Egger's linear regression test (P=0.34; Figure 5B).

Each circle represents a separate study of the indicated association,and the size of circle is positively proportional to the sample size of each study( A:Begg’s plot ; B :Egger’s plot).Figure 5 Begg’s plot and Egger’s plot for the evaluation of publication bias
3 Discussion
From the beginning of the vascular surgery to the endovascular era,vascular restenosis represents the main clinical problem with what is named “a challenge for a vascular surgeon”[20].Therefore,it is necessary to explore pathogenesis and identify reliable prognostic biomarker of restenosis.Numerous studies have revealed that nitric oxide (NO) play an essential role in the suppression of neointimal hyperplasia and restenosis,NO mediates this effect by inhibiting the phenotypic switching of vascular smooth muscle cell,stimulating of endothelial cell growth and platelet activation[7-8].In the vasculature,NO is derived from L-arginine oxidation catalyzed by the constitutively expressed nitric oxide synthase.ADMA is formed by methylation of arginine residues in proteins and released after proteolysis and act as an endogenous nitric oxide synthase inhibitor[21-24].In previous studies,exogenous ADMA directly induces vascular smooth muscle cells phenotype change and migration[25-26].These finding indicate ADMA may serve as a potential prognostic marker for restenosis.
Therefore,we performed a systematic review and Meta-analysis to evaluate the strength of the association between circulating ADMA concentration and restenosis.The results suggest that patients with higher circulating ADMA after vascular reconstruction are associated with significantly higher risk for the incidence of restenosis.However,we found substantial heterogeneity in studies estimating ADMA (Figure 2).To explore potential sources of heterogeneity we presented data on subgroups based on methodology used to determine ADMA.
Measurement of ADMA was hampered by its low concentration in plasma[27].Current analytical methods to determine ADMA concentration include HPLC[28],mass spectrometric[29-30],capillary electrophoresis[31]and ELISA[32].Currently,HPLC and ELISA are the most frequently used methods.HPLC can determine the quantity of multiple substances at the same time (eg ADMA,L-Arg),but its time-consuming analysis can be inconvenient.ELISA is an easy-to-use method with the disadvantage of less sensitivity.Previous studies found ELISA to overestimate plasma ADMA concentration compared to HPLC[33-34].By contrast,a Meta-analysis,including data from 66 studies with a total of 5,528 subjects,suggested that ELISA provided lower ADMA concentration compared to HPLC[35].In the present study,8 studies are included in the quantitative analysis (3 using HPLC and 5 using ELISA).In the case of studies using ELISA,high heterogeneity persisted even in testing studies using ELISA kits developed by the same manufacturer.Nevertheless,no heterogeneity was detected in the studies measured by HPLC (Figure 4).These results indicate that the ELISA of ADMA sampling is a determinant of heterogeneity among the included studies,as already alluded to,the source of heterogeneity attribute to insensitivity of ELISA.
There are some limitations in this Meta-analysis should be considered.First,heterogeneity could not be fully investigated because of the small sample size.The potential source of heterogeneity may be linked to not only analytical techniques,but also different baseline characteristics of patients,sample collection and sample storage conditions.Subgroup analyses based on these characteristics are recommended in future studies.Second,the inclusion of case-control studies increased susceptibility to selection bias.Besides,included studies had a relatively small sample size,which could indicate a higher risk of type I and II errors; however,both Begg's test and Egger's test do not point towards publications bias.Last but not least,although significant relationship between high ADMA and vascular restenosis is detected in this study,it failed to provide the optimum ADMA cut-off value for clinical practice,which is an inherent shortcoming for Meta-analysis.
This systematic review and Meta-analysis show a significant positive association between elevated circulating ADMA concentration and restenosis,which indicates ADMA could serve as a potential biomarker of restenosis.We recommend the use of HPLC for detection of ADMA instead of ELISA.
