Operations of school health program assessment at selected secondary schools in Egor Local Government Area, Benin City, Nigeria
2021-06-29
ABSTRACT
Keywords: Assessment, children, education, health promotion, Nigeria, school health program
INTRODUCTION
Globally, different initiatives have been proposed by various international organizations with a view to achieving greater integration of youth-oriented health promotion activities,one of those programs is school health program (SHP) that was launched in 1995.[1]SHP is an integrated set of planned,sequential, school-affiliated strategies, activities, and services designed to promote the optimal physical, emotional, social,and educational development of students.[2,3]The program is family oriented and it is determined by the local community,based on community needs, resources, standards, and requirements.[4]It is coordinated by multidisciplinary team and is accountable to the community for program quality and effectiveness.
The SHP is made up of five key components, namely healthful school environment; school-feeding services; skills-based health education; school health services; and school, home,and community relationships.[5-7]Pre-entering medical screening/examination, school health records, sick bay, first aid, and referral services are some of the services that SHP renders.[8]
The operation of SHP in schools is an important issue of great concern because children who are kept in these schools if not properly care for will have health problems that can affect them in their later years.[9]SHP helps the children by responding to their first aid needs, administering care,listening to the pupils, establishing a preventive program,advising children, health education, aiding the integration of weak and chronically ill children, and caring for the cleanliness of the environment.[1,3]Qualified health-care professionals and first aid attendants are provided by the school authority as approved by the Ministry of Education.[10,11]The Universal Basic Education (UBE) Act has an expanded scope which includes program and initiatives for childhood education,development, and health.[12-14]The UBE program has made provision for every school to have school health services and health facilities to cater for children in their school.[15,16]The national policies, reforms, and the Child Rights Act[17,18]and the UBE Act[16,19]on the national policies on education,food, nutrition, and health are laws and policies which have given shape to different sectorial interventions on childhood care and development in Nigeria. Infections are common in children and can occasionally result in illness in a child or outbreaks of illness in groups of children.[20,21]When living at home, children will have contact with a limited number of people from whom they may contact an infection, but while in school, they will come in contact with far greater number of other children; interaction through play and also the manipulation and sharing of educational materials provided greater opportunity to be exposed to a range of infections.It will never be possible to prevent all infectious diseases in children, but the risk of contracting infection can be reduced by maintaining strict observance of simple health habit practice, and hygiene is essential to achieving the goal.[22]It should be noted that early years of a child’s life are the most formative, and if there is poor care at that time, it may leave lasting physical, mental, and potential handicaps to the child for the rest of their life.[23]SHP is established for health appraisal,and control of communicable diseases, record keeping and supervision of all other issues related with school children's health. SHP is part of school health services which has been described as a neglected component of primary health care.[8,24]These services are not well performed and evaluated after provision according to the UBE Act. Studies show that school health services are the basic requirements for child care and major ingredients for the child’s development, if properly performed.[8,22,24]Therefore, this study assesses the operations of school health services in schools in Egor Local Government Area (LGA), Benin City, Nigeria.
MATERIALS AND METHODS
Research design

The inclusion criteria were as follows: school health education teachers who were willing to participate in the study and who consented after carefully going through the detailed procedure of bioethical principles in conducting research studies on human participants. The exclusion criterion was any school health teachers who are on sick or maternity leave.
Data collection tools and procedure
Data collection instrument was a self-developed structured questionnaire, using items from published instruments that were modified and developed specifically for the purpose of this study. The research instrument consists of five sections as follows: Section A of the instrument contains the demographic details of the school. Section B contains responses on the level of awareness of the objectives of the SHP. Section C seeks information on structures put in place for achieving the objectives of SHP. Section D seeks information on strategies put in place for the realization of the objectives of SHP. Section E seeks information on constraints for the full realization of the objectives of SHP.
The instrument was assessed and scrutinized by an expert to verify the content validity ensuring the items measured what is ought to measure. In order to ensure the reliability of the instrument, the split-half method was used as an indicator of the instrument stability and consistency. This was done by administering the instrument to 10 schools in Ovia Local Government. A correlational score (s) of 0.87 was obtained showing a high level of reliability of the instrument.The researchers with the help of other research assistance administered the questionnaire to the school health teachers.The researchers were present during the filling of the questionnaire for correction as well as clarity and achieved 100% return of the instrument.
Ethical consideration
Ethical approval for this study was not required, but the researchers strived to do no harm to participants. Permission was seeking from head of the schools, and a consent form was given to the school health teacher to seek written and verbal consent before data collection. Participants were not being exploited financially and physically.
Statistical analysis
Data obtained were coded and analyzed using the Statistical Package for the Social Sciences (SPSS) version 21.00 statistical software (IBM corp. released 2012. IBM SPSS Statistics for Widows, version 21.0, Armonk, NY, USA: IBM Corp). Variables and research questions were analyzed using frequencies,percentage, mean, and standard deviation statistics.
RESULTS
The demographic characteristics of the respondents are presented in Table 1: It revealed that 7 (12.5%) of the respondents were males while 49 (87.5%) of the respondents were females. Majority of the respondents were between the ages of 21 and 30 years, and only 5.36% were 51 years and above, with a total mean age of 28.50 ± 4.35.
The table also showed that 46 (82.1%) of the schools were private schools while 10 (17.9%) of the schools were public schools. This revealed that an overwhelming percentage of the schools were private schools. This table also revealed that 40 (71.4%) of the respondents had health-related qualification and 16 (28.6%) had nonhealth-relatedqualification which included National Certificate of Education, Teacher Grade 11 Certificate, Bachelor of Science in Education, and so on.

Table 1: Respondents’ demographic characteristics of the health teachers in both private and public schools in Egor Local Government Area, Benin City, Nigeria
From Table 2, 56 (100%) of the respondents were aware that the objectives of SHP were as follows: early detection and care of students with health problems, development of healthy attitude and healthy behavior by students,ensuring healthy environment for children at schools, and prevention of communicable diseases at schools. Therefore,the result revealed that an overwhelming percentage of the respondents (school health personnel) were aware of the objectives of SHP. Hence, the level of awareness was high.
The human and materials resources put in place for the smooth running of the SHP were presented in Table 3: it showed that 14(25%) of the school had sickbay while 42(75%)didn't have, 20(35.7%) of the school sick bay or health service was run by school nurse while 36(64.3%) was run by other school health teachers. Forty-nine (87.5%) of the schools had first aid box while 7 (12.5%) didn't have. Forty-three (76.8%)had safe water supply and sanitary facilities while 13 (23.2%)didn't have. Fifty-six (100%) of the schools didn't have ambulance for conveying sick children. Two (3.6%) carried out visual activity and hearing test on students while 54 (96.4%)of the schools didn't. In conclusion, the structures put in place for a smooth operation of SHP were first aid box,safe water supply, and sanitary facilities as indicated by thehigh percentage while the structures lacking were sickbay,ambulance, visual activity, and hearing test as indicated by the low percentage. In addition, the school health services were mainly run by nonhealth-related professional (teachers).

Table 2: Level of awareness of school health program and its importance among the health teachers in Egor Local Government Area,Benin City, Nigeria
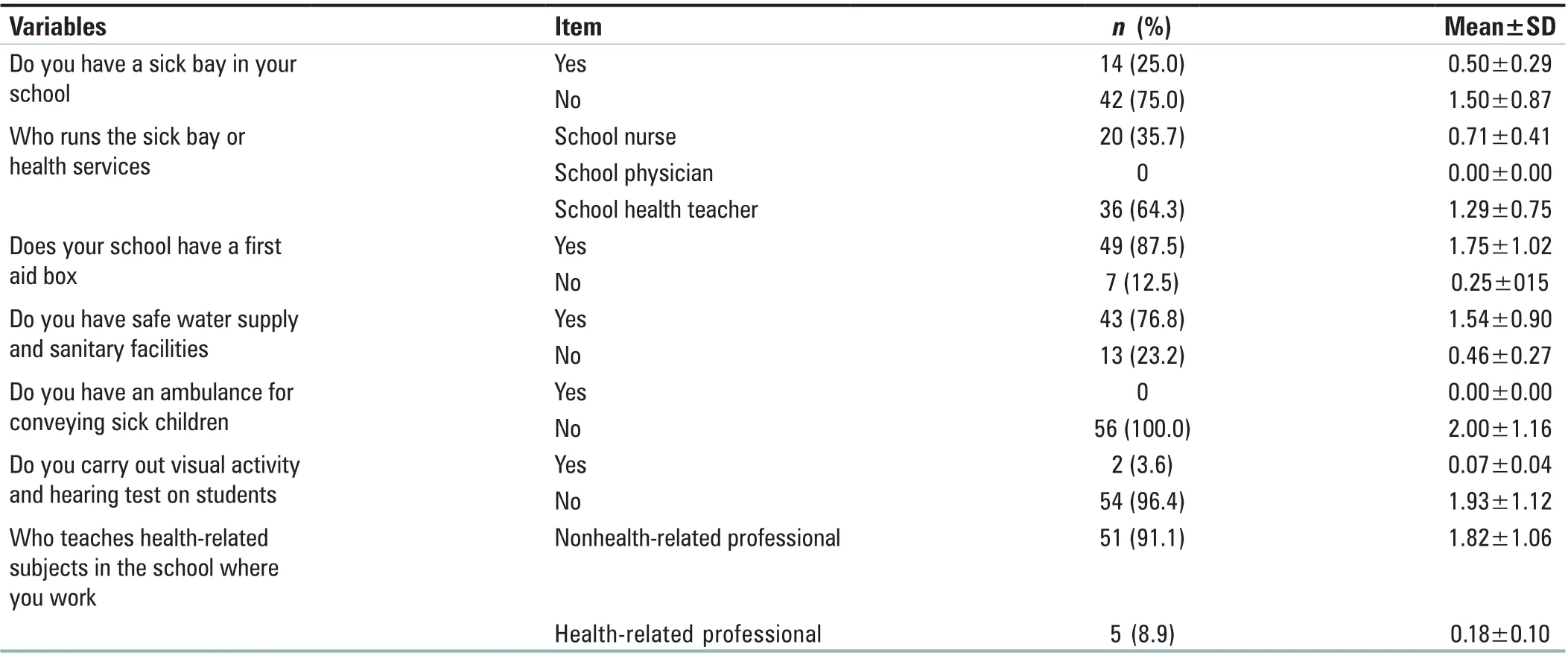
Table 3: Structures in place for a smooth operation of school health program in Egor Local Government Area, Benin City, Nigeria
Table 4 showed the strategies put in place for the realization of the objectives of SHP. 38(67.8%) of the schools studied found to keep health record while 18(32.2%) didn't, 49(87.5%)required certificate of immunization before they can be given admission into their school while 7(12.5%) didn't require that.Sixteen (28.6%) of the schools gave regular health education while 40 (71.4%) didn't. Eighteen (32.2%) of the schools were visited by health visitors while 38 (67.8%) were not.
Table 5 revealed constraints for the full realization of the objectives of SHP. Fifty-six (100%) of the schools agreed that lack of knowledge was a constraint, 56 (100%) of the schools agreed that lack of support was a factor, and 56 (100%) of the schools revealed that lack of materials was a constraint. Fifty-two (92.8%) of the schools agreed that lack of supervision was a constraint while 4 (7.2%) didn't,50 (89.3%) of the schools agreed that insufficient personnel was a constraint while 6 (10.7%) didn't, and 56 (100%) of the schools agreed that inappropriate funding was a constraint.In conclusion, lack of knowledge, lack of support, lack of material, lack of supervision, insufficient personnel, and inappropriate funding were constraints against full realization of SHP.
DISCUSSION
Awareness of the objectives of school health program
All the participants are aware of the objectives of SHP in schools in Egor LGA of Edo State; this shows that the level of awareness is high. This is in agreement with the work done by Odeyemi et al.,[25]whose findings showed that majority of the schools were aware of the SHP and its objectives, but contrary to the work done by Ademokun et al.,[26]whose findings showed that there was a low level of awareness of SHP and its objectives among schools.
Operation of school health program
This present study also shows that structures put in place for the smooth operation of SHP among schools in Egor LGA of Edo State include first aid box, safe water supply,and sanitary facilities, while the structures lack sick bay,ambulance for conveying sick students, health personnel,and medical examination (visual acuity and hearing test). Thisresult is consistent with the study carried out by Kuponiyi et al.[8]in 2016 who found that strategies put in place for the actualization of the set SHP objectives to the proper documentation of health record, utilization of immunization certificates for school admission, regular health visitation and health education. This is in line with the research carried out by Dania and Adebayo,[27]who synthesized available information on implementation of the program across Nigeria for the purpose of policy review and program improvement,and found that the implementation of SHP across the country was suboptimal because of poor coordination of the program and opined that there is a need to re-establish or strengthen the program in the country. Another study further explained this position by identifying lack of knowledge, lack of support,lack of materials, lack of supervision, insufficient personnel,and inappropriate funding as constraints for full realization of the objectives of SHP.[28]Nigeria as a country is facing shortages of health workers, and there is a need to identify the underlying reasons for the shortages, determine what motivates health workers to remain in the health sector, and evaluate the incentives required for maintaining a competent and motivated health workforce.[29]Decision-making factors and responses to financial and nonfinancial incentives have not been adequately monitored and evaluated in SHP.Therefore, efforts must be made to build the evidence base so that countries like Nigeria can develop appropriate workforce strategies and incentive packages to deliver effective SHP.

Table 4: Strategies put in place for realization of the objectives of school health program in Egor Local Government Area, Benin City, Nigeria
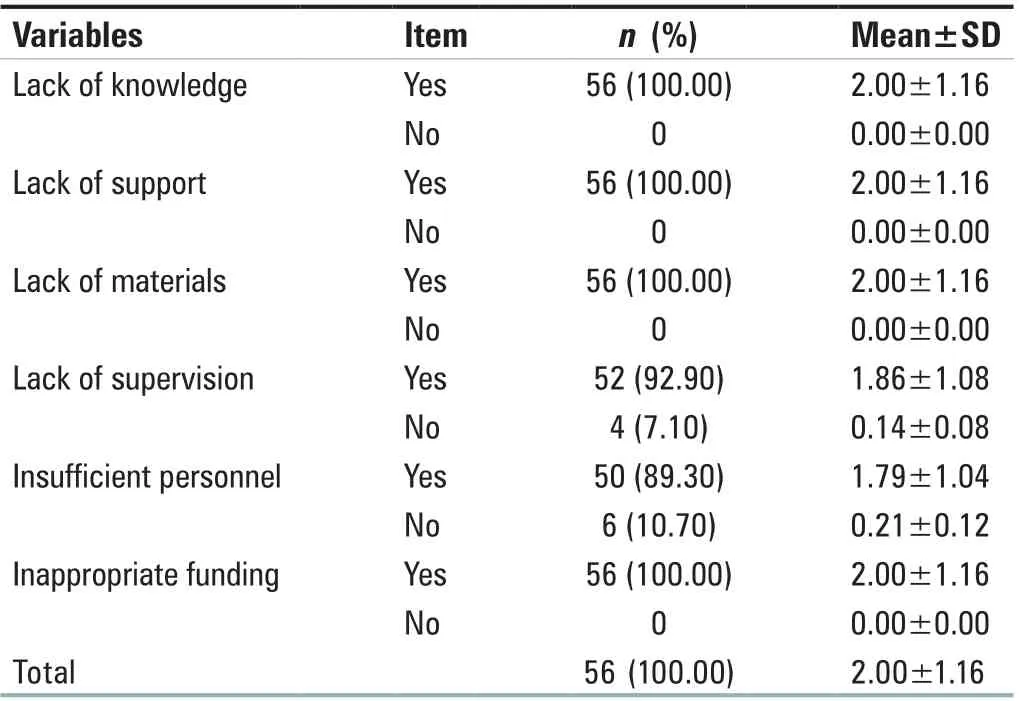
Table 5: Constraints for full realization of school health program in Egor Local Government Area, Benin City, Nigeria
Limitations
Nevertheless, this study was faced with some challenges like the limited number of the participants, this will be better if more schools can be included in the study, and comparative analysis can be conducted to identify why there is variation in result from one school to the others.
CONCLUSION
This study found that the participants are aware that the objectives of SHP and the structures needed to put in place for a smooth operation of SHP are first aid box, safe water supply,and sanitary facilities as indicated by the high percentage while the structures lacking were sickbay, ambulance, visual activity, and hearing test as indicated by the low percentage.In addition, this study found that the school health services were mainly run by nonhealth-related professional (teachers),which constitutes a major drawback in SHP. Furthermore, the strategies put in place for the realization of the objectives of SHP are keeping records and requesting for immunization records before giving admission as indicated by majority of the schools, while strategies lacking are health visitation.The constraints for full realization of the objectives of SHP were lack of knowledge, lack of support, lack of materials, lack of supervision, insufficient personnel, and inappropriate funding. Therefore, the authors made the following conclusion: there is a high level of awareness of SHP among all schools. The SHP is being run in most schools,however, not equiped with professional health teachers, and its components are not fully implemented due to numerous constraints such as lack of knowledge, lack of support, lack of materials, lack of supervision, insufficient personnel, and inappropriate funding.
Recommendations
First, in-service training on SHP should be provided to better equip the personnel to play their role in full implementation of SHP. Second, the various school authorities should ensure that regular supply of the needed medical equipment is made available to their schools. The government should employ competent health personnel to take charge of the school health services, as the research study revealed that provision of school health service personnel in secondary schools is grossly inadequate.
What this topic adds to the body of knowledge
It enlightens the school administrators on how to monitor the health status of the students, and educates them on the materials and appropriate personnel required for the smooth running of the school health program.
It also enables the health-care professional to educate the staff, students, parents, and the community on healthful living and the importance of school health services. It also affords the Ministry of Health in policymaking regarding regular inspection of schools and administration and supervision of schools.
Acknowledgments
The authors wish to sincerely thank all the principal and science teachers who participated in the study despite their tight academic schedule.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
杂志排行

Journal of Integrative Nursing的其它文章
- Control effect of structured skin care plan of integrated Chinese and Western medicine in elderly patients with incontinence‑associated dermatitis
- Analysis of risk factors for lymphedema of the lower limbs after endometrial cancer surgery and suggestions for prevention and treatment
- Effect of structured education program on physiological and psychosocial outcomes in type 2 diabetes patients:A randomized controlled trial
- The effect of baduanjin exercise in rehabilitation for functional ankle instability: A study protocol for a ra ndomized controlled pilot trial