Effect of structured education program on physiological and psychosocial outcomes in type 2 diabetes patients:A randomized controlled trial
2021-06-29
ABSTRACT
Keywords: Diabetes, injection techniques, insulin, structured education
INTRODUCTION
China has the world’s largest number of adults with diabetes;a situation sometimes referred to as diabetes epidemic.According to statistics, 11.2% of adults aged 18 and older living in mainland China in 2017 had diabetes.[1]Because diabetes is a heavy economic burden on society, family, and individuals in China, extensive efforts by health-care providers must be put forth to control diabetes and reduce its complications. Poor blood glucose control remains a major problem. China had particularly poor record of well-controlled blood glucose in patients with Type 2 diabetes (among which 21.8% of patients on insulin only and 27.0% of patients on insulin in combination with oral antidiabetic drugs).[2]One reason of this situation caused was mainly poor insulin injection technique, and it is also a global problem. Lipohypertrophy, bleeding, even infection at the injection site resulting from incorrect insulin injection techniques (such as needle reuse and incorrect rotation of injection sites) can reduce insulin absorption,cause an asynchronous effect of blood glucose peak and insulin peak, leading to increased risk of hyperglycemia and nocturnal hypoglycemia.[3-6]In addition, diabetes is a lifelong disease and living with diabetes can be challenging and stressful, which may cause psychological comorbid conditions such as anxiety and depression disorders. One approach by nursing staff to control blood glucose and reduce diabetes complications is enhancing self-management by implementing and evaluating an evidence-based structured diabetes education program and using physiological as well as psychosocial interventions.[7]
The purpose of this study was to examine the effect of structured education program versus usual (traditional)care on insulin injection technique as well as physiologically and psychosocially related outcomes in adults with Type 2 diabetes. Although diabetes education in mainland China began in 1990, today this education still takes the form of a traditional short-term “teach to (knowledge infusion)”approach while neglecting patient’s behavior change,individual assessment, or long-term follow-up.[8]Using structured education would be a step forward to test evidence-based interventions in China. Therefore, the need for research on structured education in China is great as well as the need to see how advanced education programs could be used clinically in future.
MATERIALS AND METHODS
Ethical approval for this study was provided by Affiliated Hospital of Integrated Traditional Chinese and Western Medicine, Nanjing University of Chinese Medicine, and all patients gave their written informed consent before enrolling in the study.
Patients
This randomized controlled trial enrolled inpatients with Type 2 diabetes from August 2014 to November 2014.In this study, the sample size calculation formula of the intervention study was adopted. Based on the result of the previous study,[9]the required sample size for each group was calculated as twenty cases. Considering the 20% loss of follow-up rate, the sample size was calculated as 24 cases in each group. Totally, 71 patients were enrolled in this study, and they were randomly divided into intervention group (n = 36) and control group (n = 35) according to random number table method [Figure 1]. The inclusion criteria were (1) a confirmed diagnosis of Type 2 diabetes mellitus (T2DM),[10](2) men or women ≥18 years of age, (3) insulin or an insulin pen use, and (4) an ability and willingness to accept structured education. Exclusion criteria were (1) pregnancy or breastfeeding, (2) serious neurological or mental disorders, (3) coagulopathy, serious complications (cardiovascular disease or end stage renal disease), or (4) acute illness.
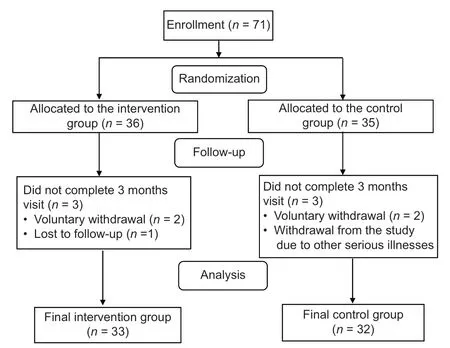
Figure 1: Trial flow diagram of this study
Intervention
Patients in the intervention group received structured education program, while patients in the control group received traditional diabetes education. The structured education program was in the form of inpatient education and consultations, and outpatient consultations and follow-up. The program began with an inpatient interactive group teaching approach, 1 h a session, 3 sessions a week, for a total of 6 sessions in 2 weeks. Each group had 10–15 patients. Diabetes educator called the participants 1 day in advance to participate in the 2ndday of the class.Diabetes courses are taught using slide shows, and the following topics were covered: diabetes basic knowledge,diet management, exercise management, blood glucose monitoring, prevention of diabetes complications, and insulin therapy. In addition to the slide show approach,food models, skill demonstrations, and an insulin injection technique video were used. Participants received education on insulin injection techniques individually.One week after the inpatient sessions were completed,patients set self-management goals and decided on an implementation program with the diabetes educator. Next,the diabetes educator scheduled the 3 monthly follow-up clinic visits. During each clinic visit, the diabetes educator inquired about the completion of goals. If the goals were achieved, new goals were set by the participants after a discussion with the educator. If not, the educator and the participants would work together to revise the goals to be more achievable. If their blood glucose was too high or too low, the educator strongly urged participants to see the doctor.
Participants in the control group were given the same inpatient group education during their hospital stay as the intervention group received--six 1-h sessions of diabetes courses. The topics of the group classes and the teacher were the same as those for the intervention group. Participants also received education on insulin injection techniques individually. They could consult a diabetes educator at any time after discharge if they have any questions about diabetes self-management.
Instruments
Diabetes Distress Scale
The Diabetes Distress Scale (DDS) is a tool to evaluate psychological distress of patients with diabetes, which was developed by Polonsky et al.[11]in 2005. Yang and Liu[12]modified the scale into Chinese version in 2010 which was more suitable for Chinese patients and reported Cronbach’s alphas of 0.84–0.95, and test–retest reliability of 0.849. The DDS has four domains and includes 17 items, emotional burden (5 items), physician-related distress (4 items),regimen-related distress (5 items), and diabetes-related interpersonal distress (3 items), a total score was the sum of the 17 items. These items use a six-point Likert scale ranging from 1 = no problem, 2 = a slight problem, 3 = a moderate problem, 4 = a somewhat serious problem, 5 = a serious problem, to 6 = a very serious problem. Higher scores indicate greater distress.
Summary of diabetes self‑care activities
The summary of diabetes self-care activities (SDSCA) is a tool to evaluate the self-management behavior of patients with diabetes. The scale contains 11 items consisted in five dimensions: Diet, exercise, blood glucose testing, medication taking, and foot care. Each item is scored ranging from 0 to 7,reflecting the number of the days the behavior performed by the patient. Higher scores indicated better self-management behavior. The Cronbach’s ɑ coefficient of the scale was 0.62,and re-test reliability was 0.83.
Evaluating indicators
The evaluation indicators included clinical and biochemical characteristics, blood glucose, blood lipid, hypoglycemia,insulin injection technique, changes in DDS scores, and SDSCA scores before and after intervention.
Statistical analysis
All statistical analyses were conducted with SPSS version 16.0 software (SPSS Inc., Chicago, IL, USA). Differences between groups at baseline were analyzed using t-test and Chi-square test. Scales that assessed patient-reported outcomes were scored according to scoring algorithms. Between-group comparisons were made using nonparametric test with Mann–Whitney U-test for continuous variables and Pearson’s Chi-square for categorical variables. A value of P < 0.05 was considered statistically significant.
RESULTS
Baseline clinical and biochemical characteristics
Of the 71 participants, 65 completed the trial. The baseline characteristics of the participants were presented by group [Table 1]. There was no statistically significant difference between groups in any of the baseline clinical and biochemical characteristics (P > 0.05).
Blood glucose
There were no statistically significant differences between groups in glycosylated hemoglobin (HbA1c), fasting blood glucose (FBG), and postprandial blood glucose (PBG)at the baseline (P > 0.05). After 3 months, HbA1c was lower (7.42 ± 0.80 vs. 8.35 ± 1.40, P = 0.002), FBG was lower (7.27 ± 1.06 vs. 9.40 ± 3.16, P < 0.001),and PBG was lower (10.33 ± 2.20 vs. 12.77 ± 4.94,P = 0.012) in the intervention group than in the control group [Table 2].
Blood lipids
No significant differences were found between groups at baseline and after 3 months regarding total cholesterol (TC),triglyceride (TG), high-density lipoprotein-cholesterol (HDL-C),and low-density lipoprotein-cholesterol (LDL-C)(P > 0.05) [Table 2].
Hypoglycemia
There was no significant difference between groups in the occurrence of hypoglycemia at the baseline (P > 0.05). After 3 months, we found that the occurrence of hypoglycemia episodes fell from 27.27% to 9.10% in the intervention group and fell from 25.00% to 12.50% in the control group, but there was still no significant difference between groups or within group (P > 0.05) [Table 3].
Insulin injection technique
No significant difference was found in needle reuse,lipohypertrophy, or injection site rotation between groups at the baseline and after 3 months (P > 0.05). The frequency of patient needle reuse decreased from 5.38 ± 6.52 to5.23 ± 5.09 in the intervention group, and increased from 5.38 ± 4.72 to 6.05 ± 5.00 in the control group after 3 months, but there was still no significant difference within group (P > 0.05) [Table 3]. Lipohypertrophy was reduced from 0.15 ± 0.50 to 0.03 ± 0.17 in the intervention group and from 0.25 ± 0.80 to 0.22 ± 0.71 in the control group after 3 months, but there was no significant difference within group (P > 0.05). The number of participants in the intervention group who rotated correctly increased from 60.61% to 78.79%, whereas in the control group, it was decreased from 68.75% to 65.63%, but there was no significant difference within group (P > 0.05) [Table 3].

Table 1: Baseline clinical and biochemical characteristics between groups
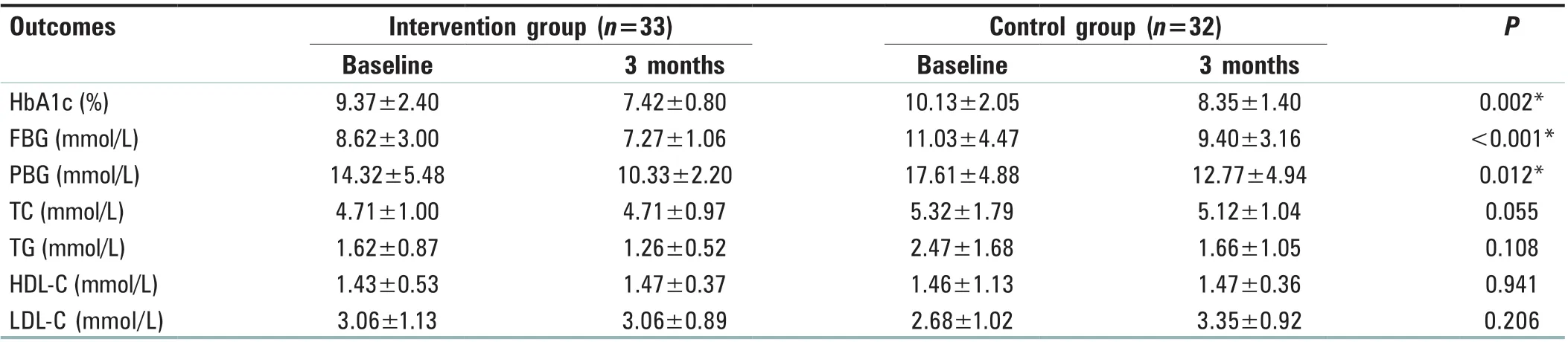
Table 2: Blood glucose and blood lipids between groups over 3 months
Changes in Diabetes Distress Scale scores and summary of diabetes self‑care activities scores
There was no statistically significant difference in total DDS scores or subscale scores between groups at baseline and after 3 months [Table 4].

Table 3: Insulin injection techniques between groups over 3 months

Table 4: Diabetes distress between groups over 3 months

Table 5: Summary of diabetes self‑care activities scores between groups over 3 months
Change in summary of diabetes self‑care activities scores
There was no statistically significant difference in total SDSCA scores and all items at baseline between the groups.After 3 months, there is no statistically significant difference between groups or within group regarding the above variables (P > 0.05) [Table 5].
DISCUSSION
The American Diabetes Association (ADA) recommends that all those with diabetes should receive structured diabetes education with all these important components in accordance with national standards.[13]A structured education program is one that is planned and that covers a set of recommended standard topics and skills and can be adapted according to each patient’s needs, education status, and culture difference.[14]ADA, together with the American Association of Diabetes Educators, has developed implementation standards of structured diabetes self-management education.[15]Similarly, the British National Institute of Clinical Technology (NICE) has also proposed best clinical practice principles, which clearly point out that all those with diabetes should be provided with structured diabetes education.[16]Structured education programs for adults with diabetes in American and United Kingdom have achieved successful outcomes.[17-19]Interventions by nursing diabetes educators in China to enhance self-management of diabetes have been proved successful to certain degree.[7]
The present randomized controlled study of exploring the efficacy of structured education in the management of T2DM patients receiving insulin injection had demonstrated a significant improvement in glycemic control compared with usual care. It was found that HbA1c in the intervention group was significantly lower than that in the control group after the program was completed, which is consistent with the results of Scain et al.’s study.[20]In 2005, the Cochrane review published by Deakin et al.[10]reviewed the effect of self-management education on diabetes in structured groups.The study showed that HbA1c decreased by 1.4% in the structured education group after 6 months. In a meta-analysis of self-administered education on structured diabetes conducted by Steinsbekk et al.,[21]a total of 21 randomized controlled trials involving 2833 participants were enrolled, of which 1454 were in the intervention group and 1379 in the control group. Nearly 81.9% of the participants used insulin or other oral hypoglycemic agents, with the education time of 6–52 h, the follow-up time of 6 months to 5 years. The results showed that HbA1c decreased significantly by 0.44%in the intervention group after 6 months. However, the reduction of HbA1c in our study was much significant (2.02%in the structured education group and 1.18% in the control group) than that of the above studies. The possible reason was that our subjects were inpatients whose HbA1c at baseline was as high as 9.37% and 10.13% in the intervention and control group, respectively, and during the hospital stay,the medication for patients was reasonably adjusted. We also focused on behavior change intervention. In the process of follow-up, participants in the structured education group and educator were more concerned the achievement of the goal of changing behavior. If the goal is achieved, the educator helped the patients develop a new goal according to their actual situation to encourage them to complete behavior changes. Once the patient reported recent hypoglycemia,or FBG >8 mmol/L or PBG >13.89 mmol/L, the educator would help patients to analyze the possible reasons, and would make referrals to their endocrinologists for medication adjustment.
In this study, it was showed that there was no significant difference in TG, TC, HDL, and LDL between the structured education group and the control group after the end of the structured education program. In a study of structured education project from NICE based on theories of empowerment and discovery learning, 157 patients in the control group received conventional treatment in combination with 55-min consultation with nutritionists, nurses, and general practitioners alone; 157 patients in intervention group participated in six 2-h sessions of structured education course. After 14 months, no significant difference was found in HDL, LDL, and TG between the two groups.[16]In addition,the Cochrane review also noted that there was no statistically significant difference in TC level between the structured education group and the conventional group after 6 months.[21]The present study also showed there was no significant difference in needle reuse, injection site rotation, insulin dose,and lipohypertrophy between two groups, but the frequency of needle reuse decreased in the intervention group whereas increased in the control group. When participants were asked why they reused needles, most commonly for reasons of convenience (for example, reduction in the need to carry spare needles and avoidance of disposal issues) but also as means of saving money. In addition, the number of participants who took the correct rotation method in this study increased in the intervention group but decreased in the control group. Together,we can see the improving trend in insulin injection technique in the intervention group, but no significant difference due to the small sample size and short time intervention; most importantly,the blood glucose of participants is better controlled, which do have clinical meaning.
However, compared to blood glucose control, psychosocial metrics, such as diabetes distress and self-management behavior, which also play important roles in diabetes self-management, are less emphasized. The results in this study showed that there was no significant difference in DDS and SDSCA scores between the two groups at baseline or after 3-month intervention. This may be due to the short follow-up time in this study. In addition, it is worrisome that, in our study population, patients’ DDS and SDSCA scores are not ideal. At present, studies have confirmed that psychological distress and poor self-management behavior of patients with diabetes are important obstacles to achieve good blood glucose. The results of the study by Sumana et al.[22]showed that the higher the HbA1c of diabetic patients, the higher the corresponding DDS score. A study conducted by Alqahtani et al.[23]found that the SDSCA score showed a negative correlation with the level of HbA1c. Therefore, we suggest that health-care professionals should take effective measures to improve the psychological distress and self-management behavior of people with diabetes.
CONCLUSION
The structured education program focused on insulin injection techniques is conducive to enhancing blood glucose control and contributes to the improvement of the specification of insulin injection techniques. However, there are still some limitations in the study. First, the number of participant in this study is small, and in future research, the comparison of the effects of structured education program versus traditional diabetes education on reducing insulin injection dose, improving insulin injection technology, and reducing the incidence of hypoglycemia based on large sample size will be considered. Second, the intervention time of this study is short, and it can be extended to 1 year or more in future to compare the effect of two kinds of education program in reducing diabetes-related pain and improving self-management ability. Third, among the diabetes patients who participate in the structured education program,there are both newly diagnosed patients and those with a long course of disease. The two have different needs, and the structured education curriculum is not well targeted.In future, structured education programs can be designed specifically for newly diagnosed patients.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
杂志排行
Journal of Integrative Nursing的其它文章
- Nursing care of a patient with programmed cell death protein‑1 immunotherapy‑related myocarditis combined with coronary heart disease
- Application of rehabilitation nursing technology in the pulmonary rehabilitation of the patients after lung cancer operation
- Discussion on optimizing nursing rounds model based on the inheritance of traditional Chinese medicine nursing
- The effect of baduanjin exercise in rehabilitation for functional ankle instability: A study protocol for a ra ndomized controlled pilot trial
- Analysis of risk factors for lymphedema of the lower limbs after endometrial cancer surgery and suggestions for prevention and treatment
- Control effect of structured skin care plan of integrated Chinese and Western medicine in elderly patients with incontinence‑associated dermatitis