Comparison of effects of six main gastrectomy procedures on patients’ quality of life assessed by Postgastrectomy Syndrome Assessment Scale-45
2021-05-29KojiNakadaYoshiyukiKawashimaShinichiKinamiRyojiFukushimaHiroshiYabusakiAkiyoshiSeshimoNaokiHikiKeisukeKoedaMikihiroKanoYoshikazuUenosonoAtsushiOshioYasuhiroKodera
Koji Nakada,Yoshiyuki Kawashima,Shinichi Kinami,Ryoji Fukushima,Hiroshi Yabusaki,Akiyoshi Seshimo,Naoki Hiki,Keisuke Koeda,Mikihiro Kano,Yoshikazu Uenosono,Atsushi Oshio,Yasuhiro Kodera
Koji Nakada,Department of Laboratory Medicine,The Jikei University School of Medicine,Tokyo 105-8461,Japan
Yoshiyuki Kawashima,Department of Gastroenterological Surgery,Saitama Cancer Center,Saitama 362-0806,Japan
Shinichi Kinami,Department of Surgical Oncology,Kanazawa Medical University,Kahoku-gun 920-0293,Ishikawa,Japan
Ryoji Fukushima,Department of Surgery,Teikyo University School of Medicine,Tokyo 173-8605,Japan
Hiroshi Yabusaki,Department of Surgery,Niigata Cancer Center Hospital,Niigata 951-8566,Japan
Akiyoshi Seshimo,Department of Gastrointestinal and Pediatric Surgery,Tokyo Medical University,Tokyo 160-0023,Japan
Naoki Hiki,Department of Upper Gastrointestinal Surgery,Kitasato University School of Medicine,Kanagawa 252-0374,Japan
Keisuke Koeda,Department of Medical Safety Science,Iwate Medical University,Iwate 028-3695,Japan
Mikihiro Kano, Department of Surgery,Hiroshima City Asa Citizens Hospital,Hiroshima 731-0293,Japan
Yoshikazu Uenosono,Department of Digestive Surgery,Imamura General Hospital,Kagoshima 890-0064,Japan
Atsushi Oshio,Faculty of Letters,Arts and Sciences,Waseda University,Tokyo 162-8644,Japan
Yasuhiro Kodera,Department of Gastroenterological Surgery,Nagoya University Graduate School of Medicine,Nagoya 466-8550,Japan
Abstract BACKGROUND The effects of various gastrectomy procedures on the patient’s quality of life(QOL)are not well understood.Thus,this nationwide multi-institutional crosssectional study using the Postgastrectomy Syndrome Assessment Scale-45(PGSAS-45),a well-established questionnaire designed to clarify the severity and characteristics of the postgastrectomy syndrome,was conducted.AIM To compare the effects of six main gastrectomy procedures on the postoperative QOL.METHODS Eligible questionnaires retrieved from 2368 patients who underwent either of six gastrectomy procedures [total gastrectomy with Roux-en-Y reconstruction(TGRY;n = 393),proximal gastrectomy(PG;n = 193),distal gastrectomy with Roux-en-Y reconstruction(DGRY;n = 475),distal gastrectomy with Billroth-I reconstruction(DGBI;n = 909),pylorus-preserving gastrectomy(PPG;n = 313),and local resection of the stomach(LR;n = 85)] were analyzed.Among the 19 main outcome measures of PGSAS-45,the severity and characteristics of postgastrectomy syndrome were compared for the aforementioned six gastrectomy procedures using analysis of means.RESULTS TGRY and PG significantly impaired the QOL of postoperative patients.Postoperative QOL was excellent in LR(cardia and pylorus were preserved with minimal resection).In procedures removing the distal stomach,diarrhea subscale(SS)and dumping SS were less frequent in PPG than in DGBI and DGRY.However,there was no difference in the postoperative QOL between DGBI and DGRY.The most noticeable adverse effects caused by gastrectomy were mealrelated distress SS,dissatisfaction at the meal,and weight loss,with significant differences among the surgical procedures.CONCLUSION Postoperative QOL greatly differed among six gastrectomy procedures.The severity and characteristics of postgastrectomy syndrome should be considered to select gastrectomy procedures,overcome surgical shortcomings,and enhance postoperative care.
Key Words:Gastrectomy;Quality of life;Postgastrectomy syndromes;Patient reported outcome measures
INTRODUCTION
Gastrectomy is widely performed and is the most effective treatment for gastric cancer.Recent improvements in early-stage diagnosis and treatment have improved the detection,treatment,and subsequent curing of the disease[1].However,postgastrectomy syndrome occurs frequently[2-7],and the patient’s long-term impairments are a concern.In patients with gastric cancer,procedure selection depends on its location,extent,and progression.Daily life impairment caused by gastrectomy varies with the type of surgical procedure.Therefore,function-preserving gastrectomies such as proximal gastrectomies(PG)and pylorus-preserving gastrectomies(PPG)[8-10] are performed for early gastric cancer to attenuate the postgastrectomy syndrome associated with gastrectomy by reducing the extent of resection,and local resection of the stomach(LR)in rare cases[11].
Currently,a means of assessing the effect of gastrectomy on a patients’ daily living does not exist.Therefore,it was difficult to assess the severity and characteristics of postgastrectomy syndrome.In this context,we developed the Postgastrectomy Syndrome Assessment Scale-45(PGSAS-45)[12],which is a patient-reported outcome scale,designed to assess the effect of gastrectomy on postoperative patients’ daily living.It has been reported to be useful for assessing symptoms,living status,and quality of life(QOL)of postgastrectomy patients[13-20].Studies have investigated the postoperative QOL among procedures performed to treat gastric cancer at a specific site.However,no study has simultaneously assessed different gastrectomy procedures used to treat gastric cancer at various sites and compared the severity and characteristics of postgastrectomy syndrome for these procedures to elucidate the broader perspective of the burden of gastrectomy.Therefore,this study aimed to compare the outcomes of the six main gastrectomy procedures with respect to the patient’s QOL using PGSAS-45 in order to clarify the severity and characteristics of postgastrectomy syndrome.
MATERIALS AND METHODS
Study population
Fifty-two institutions participated in this study.The PGSAS-45 questionnaire was distributed to 2922 patients between July 2009 and December 2010.The questionnaires were given to 2922 patients,and 2520 responses were mailed to the data center.Among the 2520 respondents,152 provided answers that were deemed unsuitable for analysis.Consequently,a total of 2368 questionnaires returned by mail were analyzed(Figure 1).
Eligibility criteria
All patients enrolled in this study fulfilled the following eligibility criteria:(1)Pathologically confirmed stage IA or IB gastric cancer(for LR,other tumors,such as gastrointestinal stromal tumors(GISTs)or carcinoids,were included);(2)First-time gastrectomy;(3)Age ≥ 20 and ≤ 75 years;(4)No history of chemotherapy;(5)No recurrence or distant metastasis;(6)≥ 1 year had elapsed since gastrectomy;(7)Performance status ≤ 1 on the Eastern Cooperative Group Scale;(8)Fully capable of understanding and responding to the questionnaire;(9)Absence of other diseases or previous surgeries that may have a greater influence on the results of the questionnaire than gastrectomy;(10)No organ failure or mental disease;and(11)Provision of written informed consent by the patient.The patients with dual malignancy or concomitant resection of other organs(co-resection equivalent to cholecystectomy being the exception)were excluded.
Design
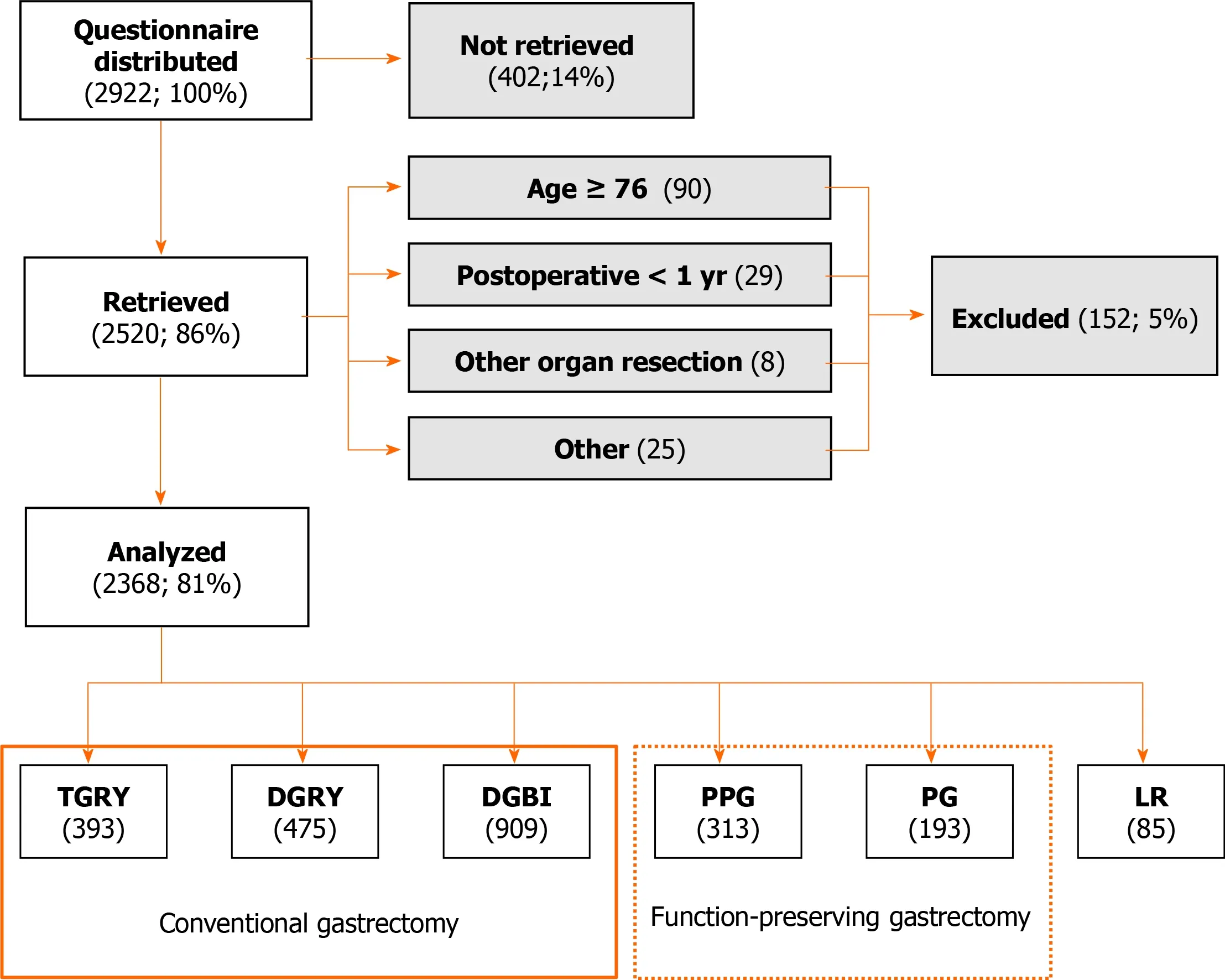
Figure 1 CONSORT flowchart of the Postgastrectomy Syndrome Assessment Study.TGRY:Total gastrectomy with Roux-en-Y reconstruction;PG:Proximal gastrectomy;DGRY:Distal gastrectomy with Roux-en-Y reconstruction;DGBI:Distal gastrectomy with Billroth I reconstruction;PPG:Pylorus preserving gastrectomy;LR:Local resection of the stomach.
We performed continuous sampling from a central registration system for participant enrollment.The questionnaire was distributed to all eligible patients on presentation to the participating clinics.The patients were requested to return the completed forms to the data center by mail.The perioperative data were reported by the attending surgeon to the data center through case report forms.All QOL data from questionnaires were matched with individual patient data collected via the case report forms.
This study was approved by the local ethics committees of each participating institution and was in accordance with the ethical standards of the responsible committee on human experimentation and with the Helsinki Declaration of 1964 and later versions.This study was registered with the University Hospital Medical Information Network’s Clinical Trials Registry as trial number 000002116.
QOL assessment
We developed the PGSAS-45 as a new integrated QOL questionnaire,comprising an 8-item short-form generic health-related QOL questionnaire(SF-8)[21] and the Gastrointestinal Symptom Rating Scale(GSRS)[22,23].In addition to the items of the SF-8(8 items)and GSRS(15 items),22 newly selected items are included,comprising questions on common postgastrectomy symptoms(8 items),number and type of dumping symptoms(2 items),amount and quality of dietary intake(8 items),daily activity status(1 item),and dissatisfaction with daily life(3 items).Hence,each patient was asked 45 questions in total(Table 1).The details of the PGSAS-45 have been reported previously[12].
Statistical analysis
Statistical analyses were performed using JMP12.0.1 software(SAS Institute Inc.,Cary,NC,United States).The differences in patient characteristics were assessed using analysis of means(ANOM)and the chi-square test,followed by residual analysis.To compare the 19 main outcome measures(MOMs)of PGSAS-45 for the six main gastrectomy techniques,the ANOM method was used,with the alpha level was set at 0.05.Values with P < 0.05 were considered significant.The statistical methods of this study were reviewed by Atsushi Oshio from Waseda University.
RESULTS
Background
The 2368 patients who underwent the six main gastrectomy procedures weredistributed according to the surgical procedure,as follows:Total gastrectomy with Roux-en-Y reconstruction(TGRY),393 patients;Proximal gastrectomy(PG),193 patients,distal gastrectomy with Roux-en-Y reconstruction(DGRY),475 patients;distal gastrectomy with Billroth-I reconstruction(DGBI),909 patients;Pylorus preserving gastrectomy(PPG),313 patients;and Local resection of the stomach(LR),85 patients(Figure 1).The average age of the patients was 62.1 years,and for patients undergoing TGRY,the mean age was significantly higher at 63.4 years(Table 2).The overall mean postoperative period was 37.7 mo.For DGBI,the mean postoperative period was significantly longer at 40.7 mo and was significantly shorter at 31.7 mo for DGRY(Table 2).The proportion of men and women in the study population was 66% and 34%,respectively.Among the patients undergoing PPG,the proportion of women was significantly higher at 41%(Table 2).The overall mean rate for the laparoscopic approach was 38% and was significantly higher for LR(61%)and DGBI(46%),but significantly lower for PG(17%)and TGRY(25%)(Table 2).The overall mean rate of preservation of the celiac branch of the vagus nerve was 24% and was significantly higher for LR(100%),PPG(71%),and PG(44%);however,it was significantly lower for TGRY(3%),DGRY(6%),and DGBI(15%)(Table 2).

Table 1 Structure of Postgastrectomy Syndrome Assessment Scale-45

In italicized items or subscales,higher score indicates better condition;In non-italicized items or subscales,higher score indicates worse condition.Each subscale is calculated as the mean of composed items or subscales except physical component summary and mental component summary of 8-item shortform generic health-related quality of life questionnaire.Item 29 and 32 don't have score.Then,they were analyzed separately.GSRS:Gastrointestinal Symptom Rating Scale items;PGSAS:Postgastrectomy Syndrome Assessment Scale items;QOL:Quality of life;SF-8:8-item short-form generic healthrelated QOL questionnaire.
Symptoms
When comparing postgastrectomy symptoms of each type of gastrectomy with the overall mean symptom scores,most symptoms were severe for TGRY,while for LR,the symptoms,except for abdominal pain subscale(SS),were mild(P < 0.05).In PG,meal-related distress SS and esophageal reflux SS were serious complications(P < 0.05).The meal-related distress SS was low for both DGBI and DGRY.In addition,the esophageal reflux SS was low for DGRY and the indigestion SS was low for DGBI,respectively(P < 0.05).The diarrhea SS and dumping SS were reported less severe for PPG(P < 0.05).
Among the seven symptom SS,after gastrectomy,the most prominent symptom with higher scores were meal-related distress,constipation,and diarrhea.Additionally,as the mean score of symptoms for a specific gastrectomy type significantly differs from the overall mean score of symptoms,the symptom MOMs showing a large difference depending on the procedure were meal-related distress SS(noted in 5 of the 6 gastrectomy procedures),followed by esophageal reflux SS(4 of the 6 gastrectomy procedures)(Table 3).
Living status
Compared with the overall mean living status scores,the postgastrectomy living status for TGRY was clearly worse for all MOMs,except for the quality of ingestion SS,whereas the postgastrectomy living status for the LR was significantly better for all MOMs(P < 0.05).Moreover,for PG,the ingested amount of food per meal was low,quality of ingestion SS was poor,and weight loss was massive(P < 0.05).DGBI and PPG were associated with lesser necessity for additional meals and less weight loss;moreover,DGBI was associated with better ability for working(P < 0.05).Additionally,as the mean score of living status for a specific gastrectomy type significantly differs from the overall mean score of living status,the living status MOMs showing a large difference depending on the procedure were weight loss(noted in 5 of the 6 gastrectomy procedures),followed by necessity for additional meals(4 of the 6 gastrectomy procedures)(Table 3).
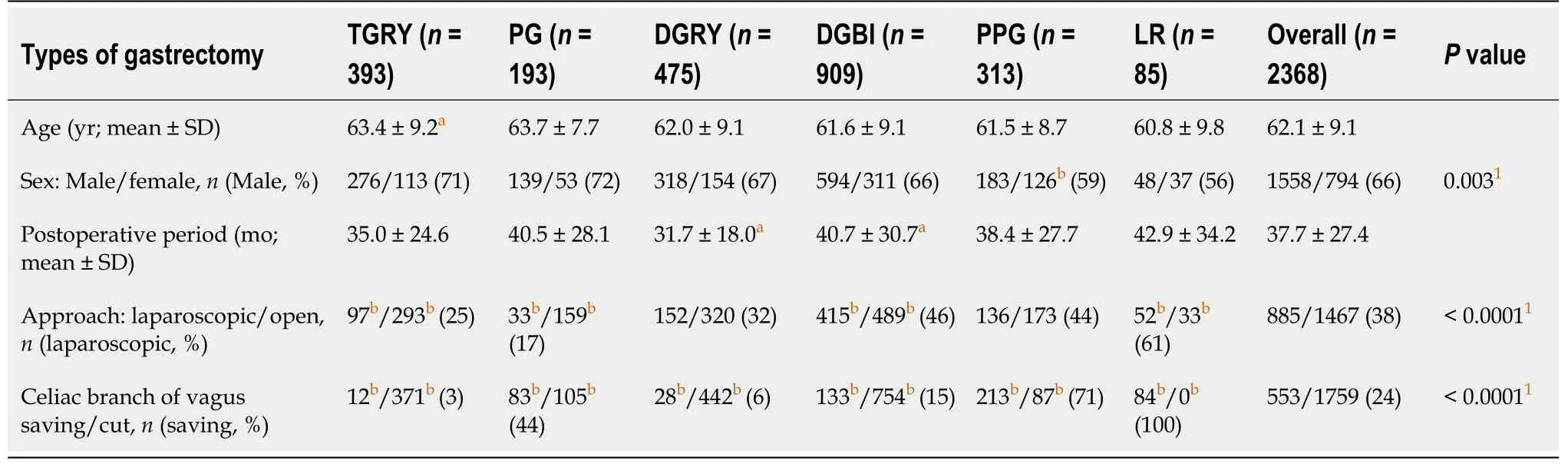
Table 2 Patients' background
QOL
Compared with the overall mean QOL scores,TGRY showed poor scores for all QOL MOMs,except for the mental component summary of SF-8,whereas LR showed excellent scores for all QOL MOMs(P < 0.05).For PG,a significantly more patients reported dissatisfaction at the meal,dissatisfaction at working,and dissatisfaction for daily life SS(P < 0.05).The prevalence of dissatisfaction at the meal was lower for DGBI and DGRY,and that of dissatisfaction at working and dissatisfaction for daily life SS was lower for DGBI(P < 0.05).One of the QOL MOMs notable in gastrectomy was dissatisfaction at the meal.Additionally,as the mean score of QOL for a specific gastrectomy type significantly differs from the overall mean score of QOL,the QOL MOMs showing a large difference depending on the procedure,was dissatisfaction at the meal(noted in 5 of the 6 gastrectomy procedures),followed by dissatisfaction at working and dissatisfaction for daily life SS(4 of 6 gastrectomy procedures)(Table 3).
Overall characteristics
The percentage for the overall mean score of each surgical procedure was calculated for 19 MOMs of PGSAS-45(Table 4).For every 5% deviation in score from the overall mean score,1 point was added if the daily living condition was good and 1 point was subtracted if the daily living condition was bad.The total score of the 19 MOMs for each procedure was calculated and compared(Table 4 and Figure 2).The overall living condition of patients who underwent the aforementioned gastrectomy procedures was compared:The TGRY had a score of -47 points,which indicated a considerably worse living condition than other procedures,while LR had score of +97 points,which indicated a markedly better living condition compared to the other procedures.PG,where the proximal stomach was resected,had a score of -26 points;therefore,the QOL of patients who underwent PG was poor compared to that of patients who underwent DGRY(3 points),DGBI(5 points),and PPG(10 points),wherein the proximal stomach is presented.The QOL was better for the patients who underwent PPG where the pylorus was preserved compared to those who underwent DGBI and DGRY,and was almost similar between the patients who underwent DGBI and DGRY.

Table 3 Comparison of main outcome measures of Postgastrectomy Syndrome Assessment Scale-45 among six types of gastrectomy using ANOM
DISCUSSION
In this study,we developed the PGSAS-45 questionnaire for the assessment of postgastrectomy syndrome.Using this questionnaire,we examined the effects of the six main gastrectomy procedures on patients’ daily living.The results revealed that TGRY had the worst postoperative QOL score,whereas LR had the highest postoperative QOL score.For PG,where the proximal stomach is resected,the postoperative QOL was clearly worse than that for PPG,DGBI,and DGRY,where the proximal stomach is preserved.Post-PPG,where the pylorus was preserved,the QOL was slightly better than that of post-DGBI and -DGRY.No significant difference was found between DGBI and DGRY in terms of QOL.Among the 19 MOMs in PGSAS-45,the major differences in the surgical procedures were meal-related distress SS and esophageal reflux SS with respect to the symptoms,weight loss and necessity for additional meals with respect to the living status,and dissatisfaction at the meal,
dissatisfaction at working,and dissatisfaction for daily life SS with respect to the QOL.After gastrectomy,the most prominent burdens were meal-related distress SS,constipation SS,diarrhea SS,and dissatisfaction at the meal.To the best of our knowledge,this is the first study to simultaneously examine the effects of various gastrectomy procedures on the patients’ daily living postoperatively and to clarify the overall characteristics of postgastrectomy syndrome.
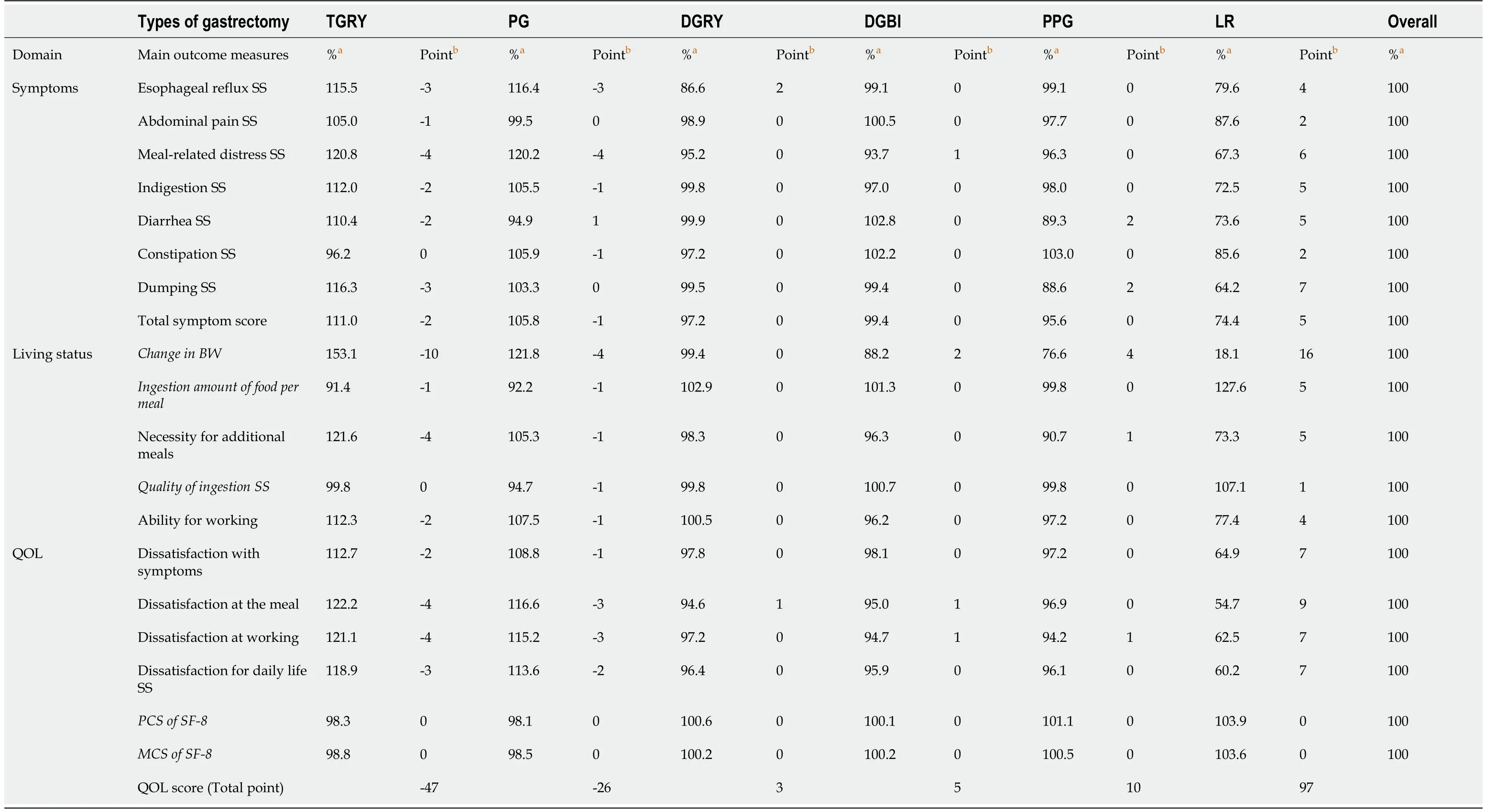
Table 4 The percentage and point against overall mean of the main outcome measures of Postgastrectomy Syndrome Assessment Scale-45 among six types of gastrectomy
In recent years,the rate of detection of early-stage gastric cancer has increased due to widespread medical screening and improvement of diagnostic techniques[1].Advances in treatment also increase the number of patients who can attain long-term postgastrectomy survival[1].On the contrary,various complications,called postgastrectomy syndrome,occur after gastrectomy[2-7],which become clinical problems that interfere with daily living.Within this context,there has been increasing interest in reducing the incidence of postgastrectomy syndrome and improving postoperative patients’ QOL,and the introduction of function-preserving surgery,such as PG and PPG[8-10],and minimally invasive surgery,such as laparoscopic surgery[24],has increased.These function-preserving surgical procedures are also accepted by the fourth edition of the gastric cancer treatment guidelines(2017)as an alternative treatment of early-stage gastric cancer(cT1N0M0)[25].
The primary purpose of gastrectomy is to cure cancer,and then,to allow the patient to live comfortably at the same level as their preoperative condition.To improve the QOL of postgastrectomy patients,it is important to select a gastrectomy procedure considering the patient’s postoperative QOL.However,to achieve this,a questionnaire,which accurately measures the postgastrectomy patients’ burden in their daily living,is essential.Many studies have compared different gastrectomy procedures[26-28],but in the absence of a suitable questionnaire to assess the effects of gastrectomy,satisfactory assessment could not be attained.In this light,PGSAS-45[12],a new questionnaire developed by the Japan Postgastrectomy Syndrome Working Party,was used to assess the gastrectomy procedures,and a nationwide multi-institutional collaborative study called Postgastrectomy Syndrome Assessment Study was conducted to elucidate the effects of the six main gastrectomy procedures on the daily living of postoperative patients.
To date,several studies have compared various gastrectomy procedures as treatment of gastric cancer on a specific site.Total gastrectomy was often performed for upper gastric cancer,but in recent years,PG,which is a function-preserving surgery,has often been performed to treat early-stage gastric cancer for expecting better QOL[8-10].A study comparing postoperative QOL between total gastrectomy and PG shows that the latter results in better QOL[29] with less diarrhea and dumping symptoms,less weight loss,and less necessity for additional meals[19].On the contrary,reflux esophagitis and anastomotic stricture have been reported in PG[17,30] and remains a problem.In this study,PG had a total QOL score of -26 points compared with TGRY having -47 points.This shows that PG has lesser worse effects on QOL than TGRY,resulting in less impairment in daily living.

Figure 2 General quality of life scores after the six main gastrectomy procedures.TGRY:Total gastrectomy with Roux-en-Y reconstruction;PG:Proximal gastrectomy;DGRY:Distal gastrectomy with Roux-en-Y reconstruction;DGBI:Distal gastrectomy with Billroth I reconstruction;PPG:Pylorus preserving gastrectomy;LR:Local resection of the stomach.
Distal gastrectomy is often performed for middle-third gastric cancer;however,PPG has also been selected as a function-preserving surgery for early-stage gastric cancer[8-10].In studies comparing the postoperative QOL of distal gastrectomy and PPG,PPG was reported to have better QOL[13,14,31-33] with fewer occurrences of diarrhea and dumping,less weight loss,and less necessity for additional meals[13].In this study,DGBI had QOL score of 5 points,and DGRY had 3 points vs PPG’s score of 10 points,indicating that PPG provides better QOL than distal gastrectomy.
Distal gastrectomy is performed as a standard surgical procedure for lower gastric cancer.DGBI and DGRY are mainly performed as reconstructive methods.Many studies have compared DGBI with DGRY[20,34-41],each of which has reported benefits,such as lesser weight loss in DGBI[20] and lower occurrence of residual gastritis and esophageal reflux symptoms in DGRY[20,38,41].However,there is no definitive view on which of the two reconstructive surgeries is effective.In this study,DGRY(3 points)and DGBI(5 points)had virtually identical scores.
The results of this study were consistent with previous studies comparing various contrasting rival gastrectomy procedures.As mentioned above,various gastrectomy procedures were compared,which revealed an increase of evidence,showing the usefulness of function-preserving surgery.In the future,we anticipate that functionpreserving gastrectomy will be applied to a wider extent to address early-stage gastric cancer.
In the overall characteristics,the worse effects of total gastrectomy on daily life were greater than those in the other five procedures(Table 4 and Figure 2)and fatal.In recent years,PG has been frequently performed for early-stage upper gastric cancer,which reduces the incidence of postgastrectomy syndrome,and the postoperative QOL is better than that in total gastrectomy.Alternatively,subtotal gastrectomy is performed,which leaves a portion of the proximal stomach even if the size of the remaining stomach becomes considerably small[42,43],and its QOL is reported better than that of TG[43].If oncological safety is maintained,avoiding total gastrectomy as much as possible,and actively adopting a procedure that leaves either the distal stomach or a portion of the proximal stomach may help improve postoperative QOL.
In contrast,the QOL after LR was by far better than that after other gastrectomy procedures.Many reports have indicated that QOL after LR was favorable[15,44,45] and that residual stomach functions were retained[44].Local gastric resection is often performed for GISTs;however,it has been performed as a surgical treatment for earlystage gastric cancers based on the sentinel lymph node concept[45,46].Endoscopic submucosal dissection(ESD)has been increasingly performed for early-stage gastric cancers,and its applicability continues to increase[47].The QOL after ESD is especially favorable[48],and it would be an ideal treatment method if gastric cancer could be completely cured.Meanwhile,gastrectomy procedures,such as PG,PPG,and DG have been performed in conjunction with the preservation of the celiac branch of the vagus nerve as function-preserving gastrectomy for lesions in early-stage non-ESD applicable gastric cancers.However,there is still a major gap between functional preservation after gastrectomy and ESD with regards to the patients' QOL.In recent years,sentinel node navigation surgery has been incorporated against early-stage non-ESD applicable gastric cancers by safely employing LR while maintaining oncological safety.As the present results show,the QOL after LR is exceedingly favorable compared to that after PPG and PG;therefore,LR may be an effective treatment option for some early-stage non-ESD applicable gastric cancers.We anticipate the safe introduction of LR against early-stage non-ESD applicable gastric cancers with the accumulation of evidence in the future.
Among the MOMs of PGSAS-45,the major differences according to the type of procedure were meal-related distress SS,change in body weight,and dissatisfaction at the meal.Therefore,the effect of gastrectomy on meal-related MOMs was extremely large,and this was considered the most important factor contributing to the reduction of QOL of postoperative patients.Of the seven symptoms SS of PGSAS-45,mealrelated distress SS and dumping SS were reported to have the largest influence on QOL,reducing postgastrectomy QOL[16].Therefore,the procedure should be improved to reduce meal-related distress SS and dumping SS.
This study has limitations.First,since the choice of gastrectomy is mainly based on the site and spread of gastric cancer,simultaneously comparing various procedures performed on gastric cancer of different sites has only a little significance on the selection of the type of gastrectomy.However,it is important for surgeons to understand the general aspects of how the site and extent of gastrectomy affect patient’s postoperative QOL.Second,this is a retrospective study,and there is a bias in the number of cases between each surgery.However,the overall analysis was based on a large number of cases(n = 2368),and the progression was relatively early as stage IA/IB.Thus,we believe that the difference in the progression of cancer has little influence on the differences between each procedure and mainly reflects the effect of the procedures.
CONCLUSION
This study provided an overview of the severity and characteristics of postgastrectomy syndrome in patients who underwent the six main gastrectomy procedures.It also clarified that the postoperative QOL differed greatly depending on the site and extent of gastrectomy.To improve postgastrectomy QOL,it is important for surgeons to understand these matters to select the appropriate procedure,to improve the surgical technique to compensate for the shortcomings of each procedure,and to enhance postoperative care by providing appropriate dietary guidance and detecting and addressing postgastrectomy syndromes at an early stage.
ARTICLE HIGHLIGHTS
Research background
No study has simultaneously assessed the effects of the different gastrectomy procedures used to treat gastric cancer at various sites on the postgastrectomy quality of life(QOL).
Research motivation
It is important for surgeons to understand the general aspects of how the site and extent of gastrectomy affect patient’s postoperative QOL.
Research objectives
The aim of this study was to compare the effects of six main gastrectomy procedures on the postoperative QOL using the Postgastrectomy Syndrome Assessment Scale-45(PGSAS-45).
Research methods
The 2368 patients who underwent either of the six main gastrectomy procedures [total gastrectomy with Roux-en-Y reconstruction(TGRY;n = 393),proximal gastrectomy(PG;n = 193),distal gastrectomy with Roux-en-Y reconstruction(DGRY;n = 475),distal gastrectomy with Billroth-I reconstruction(DGBI;n = 909),pylorus-preserving gastrectomy(PPG;n = 313),and local resection of the stomach(LR;n = 85)] were enrolled in this study.The severity and characteristics of postgastrectomy syndrome were compared among the six gastrectomy procedures by the main outcome measures of PGSAS-45.
Research results
Postoperative QOL was greatly impaired in TGRY and PG,and was excellent in LR.After distal gastrectomy,diarrhea and dumping were less frequent in PPG,and there was no difference between DGBI and DGRY.The most noticeable adverse effects with significant differences among the gastrectomy procedures were meal-related distress SS,dissatisfaction at the meal,and weight loss.
Research conclusions
Postoperative QOL greatly differed depending on the site and extent of gastrectomy.
Research perspectives
To improve postgastrectomy QOL,it is important for surgeons to understand these matters to select the appropriate procedure,to improve the surgical technique to compensate for the shortcomings of each procedure,and to enhance postoperative care by providing appropriate dietary guidance and detecting and addressing postgastrectomy syndromes at an early stage.
ACKNOWLEDGEMENTS
This study was completed by 52 institutions in Japan.The authors thank all physicians who participated in this study and the patients whose cooperation made this study possible.
杂志排行
World Journal of Gastrointestinal Surgery的其它文章
- Ewing sarcoma of the jejunum:A case report and literature review
- Biliary drainage in inoperable malignant biliary distal obstruction:A systematic review and meta-analysis
- Liver resection for hepatocellular carcinoma larger than 10 cm:A multi-institution long-term observational study
- Practices concerning sleeve gastrectomy in Turkey:A survey of surgeons
- Therapeutic effects of the TST36 stapler on rectocele combined with internal rectal prolapse
- Could neoadjuvant chemotherapy increase postoperative complication risk of laparoscopic total gastrectomy?A monoinstitutional propensity score-matched study in China