Therapeutic effects of the TST36 stapler on rectocele combined with internal rectal prolapse
2021-05-29JinMengZhiTaoYinYingYiZhangYongZhangXiuZhaoQingZhaiDeYuChenWeiGangYuLeiWangZhiGangWang
Jin Meng,Zhi-Tao Yin,Ying-Yi Zhang,Yong Zhang,Xiu Zhao,Qing Zhai,De-Yu Chen,Wei-Gang Yu,Lei Wang,Zhi-Gang Wang
Jin Meng,Yong Zhang,Xiu Zhao,Qing Zhai,De-Yu Chen,Wei-Gang Yu,Lei Wang,Zhi-Gang Wang,Department of Anorectal Disease,Shenyang Coloproctology Hospital,Shenyang 110000,Liaoning Province,China
Zhi-Tao Yin,Department of Anorectal Disease,Shenyang Hospital of Traditional Chinese Medicine,Shenyang 110000,Liaoning Province,China
Ying-Yi Zhang,First Department of General Surgery,The Third People’s Hospital of Dalian,Dalian 116000,Liaoning Province,China
Abstract BACKGROUND The most common causes of outlet obstructive constipation(OOC)are rectocele and internal rectal prolapse.The surgical methods for OOC are diverse and difficult,and the postoperative complications and recurrence rate are high,which results in both physical and mental pain in patients.With the continuous deepening of the surgeon’s concept of minimally invasive surgery and continuous in-depth research on the mechanism of OOC,the treatment concepts and surgical methods are continuously improved.AIM To determine the efficacy of the TST36 stapler in the treatment of rectocele combined with internal rectal prolapse.METHODS From January 2017 to July 2019,49 female patients with rectocele and internal rectal prolapse who met the inclusion criteria were selected for treatment using the TST36 stapler.RESULTS Forty-five patients were cured,4 patients improved,and the cure rate was 92%.The postoperative obstructed defecation syndrome score,the defecation frequency score,time/straining intensity,and sensation of incomplete evacuation were significantly decreased compared with these parameters before treatment,and the differences were statistically significant(P < 0.05).The postoperative anal canal resting pressure and maximum squeeze pressure in patients decreased compared with before treatment,and the differences were statistically significant(P < 0.05).The initial and maximum defecation thresholds after surgery were significantly lower than those before treatment,and the differences were statistically significant(P < 0.05).The postoperative ratings of rectocele,resting phase,and defecation phase in these patients were significantly decreased compared with those before treatment,and the differences were statistically significant(P < 0.05).CONCLUSION The TST36 stapler is safe and effective in treating rectocele combined with internal rectal prolapse and is worth promoting in clinical work.
Key Words:TST36 stapler;Rectocele;Internal rectal prolapse;Outlet obstructive constipation;Longo obstructed defecation syndrome score;Constipation
INTRODUCTION
Constipation is divided into three categories,outlet obstructive constipation(OOC),slow transit constipation,and mixed constipation.Of these,OOC is more common[1] and seriously affects the quality of life of patients[2-4].The most common causes of OOC are rectocele(RC)and internal rectal prolapse(IRP)[5,6].
A RC means that the anterior rectal wall protrudes forward during defecation,which is caused by weakness of the anterior rectal wall,the rectovaginal septum,and the posterior vaginal wall.The forward depression of the anterior rectal wall can be visualized by X-ray defecography and is palpable during digital rectal examination[7].Vaginal delivery is the main cause of RC[8].If the forward protruding part of the anterior rectal wall is greater than 0.5 cm,it is diagnosed as RC;0.6-1.5 cm is grade I RC,1.6-3.0 cm is grade II RC,and ≥ 3.0 cm is grade III RC[9].
IRP refers to a functional disease in which the rectal mucosa invades the rectal cavity during defecation.Sometimes it can be full-thickness intussusception,but the prolapsed part does not extend beyond the outer edge of the anus[10].IRP was first proposed in 1903[11].The main clinical manifestations of IRP include symptoms such as frequent bowel movements,anorectal swelling,incomplete defecation,and difficulty in passing stool[12].IRP ratings are grade I if the rectal mucosal prolapse is above the anorectal ring,and intussusception depth is 3-15 mm;grade II if the rectal mucosal prolapse is at the level of the dentate line,and intussusception depth is 16-30 mm;and grade III if the rectal mucosal prolapse is at the level of the anal canal,and the intussusception depth is greater than 31 mm[13,14].
The surgical methods used for this disorder are diverse and difficult,and postoperative complications and recurrence rates are high[15-22],which results in significant physical and mental pain in patients.With the continuous deepening of the surgeon’s concept of minimally invasive surgery and continuous in-depth research on the mechanism of OOC,the treatment concepts and surgical methods have also continuously improved.In this study,the TST36STARR+ stapler was used to treat patients with RC and IRP,and its effect was analyzed in terms of morphology and function after surgery to evaluate comprehensively the clinical efficacy of this new technology.
MATERIALS AND METHODS
General information
From January 2017 to July 2019,female OOC patients with RC combined with IRP who met the inclusion criteria in Shenyang Anorectal Hospital and Dalian Third People’s Hospital were selected for treatment using the TST36 stapler.A total of 49 patients aged 35-71 years with an average age of 53.1 years and a medical history of 2-20 years were enrolled.The patients all had symptoms such as straining defecation,elongation of defecation time,hand-assisted defecation,and a feeling of incomplete evacuation that lasted more than 1 year.
Inclusion and exclusion criteria
Patients who met the Rome III criteria[23] and who had two or more of the following symptoms were included in the study:(1)More than 1/4 of defecations were laborious;(2)More than 1/4 of defecations consisted of a dry ball-shaped stool or hard stool;(3)More than 1/4 of defecations resulted in a feeling of incompleteness;(4)More than 1/4 of defecations had an anorectal obstruction/blockage;(5)More than 1/4 of defecations required manual assistance;and(6)Defecation less than 3 times/wk.
The patients must have symptoms for at least 6 mo before enrollment,and the duration should be more than 3 mo.The results of defecography and virtual defecography under 360° ultrasound in the rectal cavity suggested RC(> 3 cm)combined with IRP(> 10 mm)[24,25];the balloon expulsion test was positive.
Patients with organic diseases such as irritable bowel syndrome,colonic slow transit constipation,and intestinal tumors were excluded.
Apparatus and methods
The TST36STARR+ stapler made by Touchstone International Medical Science Company Limited(Suzhou,China)was used during surgery.In addition,the Anorectum Manometer(Laborie Medical Technologies,Inc.,Mississauga,Canada)and the 360° intrarectal ultrasound instrument(Brüel and Kjær,Denmark)were also used.
Treatment methods
The procedure was carried out under sacral anesthesia.The lithotomy position was routinely disinfected to expand the anus,and the circular anal dilator matching the TST36STARR+ stapler was placed in the anal canal(Figure 1A).According to the degree of prolapse and the depth of the protrusion,parachute anastomosis was performed at the 1,5,9,and 11 o’clock positions using traction sutures,which reached the muscle layer(Figure 1B).The TST36 stapler was inserted,and the traction line was drawn through the visible window(Figure 1C).Before activating the stapler,the posterior vaginal wall was identified to prevent it from entering the stapler cavity.After activating the stapler,bleeding was observed,and hemostatic treatment was carried out.The excised specimen was examined to confirm whether it was fullthickness rectum(Figure 1D).After the operation,the patient fasted for 3 d to control defecation and was then given laxative treatment for 5 d to prevent constipation.
Efficacy evaluation
The efficacy was determined according to the Chinese Medical Association’s constipation diagnosis and treatment standards.Cure:Constipation was improved,defecation 1-2 times/d,and the stool was evacuated within 5 min.Improved:Constipation was relieved;however,there was still mild smooth defecation.Defecation 2-3 times/d,and the defecation time was shorter than before treatment.Invalid:Constipation was not improved[26].
Scoring
Defecation function in patients was evaluated by Longo’s obstructed defecation syndrome(ODS)score(Table 1)[27].
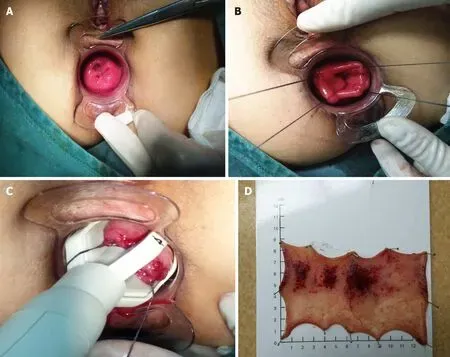
Figure 1 The TST36STARR+ surgical procedure.A:The anus was enlarged and the circular anal dilator was inserted;B:The traction sutures were performed by parachute anastomosis,and the sutures reached deep into the muscle layer;C:The traction sutures were drawn through the visible window;D:The excised specimen was full-thickness rectum.
Statistical analysis
Statistic Package for Social Science 22.0 software(Armonk,NY,United States)was used for data analysis and processing,and the paired-samples t-test was used.When P < 0.05,the difference was considered statistically significant.
RESULTS
Efficacy
Of the 49 patients included in the study,45 were cured,4 improved,and no invalid patients were observed.The cure rate was 92%.Short-term postoperative complications included anastomotic bleeding at 3-9 d after the operation in 2 patients,who were discharged after hemostasis treatment.Five patients had urine retention after the operation.Long-term postoperative complications after 1 year of follow-up showed no anal stenosis,anal incontinence,or rectovaginal fistula,and no recurrences were observed.
ODS symptom score
The patients’ constipation symptoms were followed up and evaluated 1 year after treatment,and these symptoms were significantly relieved.The results showed that the postoperative ODS score,defecation frequency score,time/straining intensity,and sensation of incomplete evacuation were significantly reduced compared with these parameters before treatment,and the differences were statistically significant(P < 0.05,Table 2).
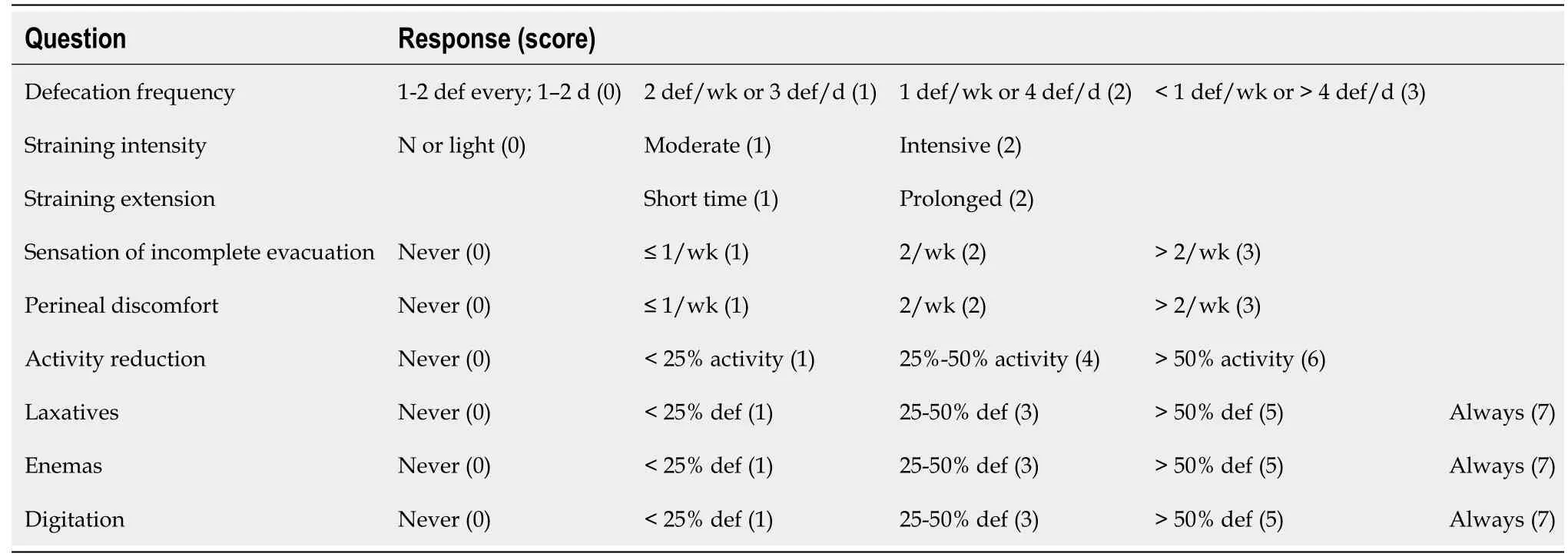
Table 1 Longo’s obstructed defecation syndrome score
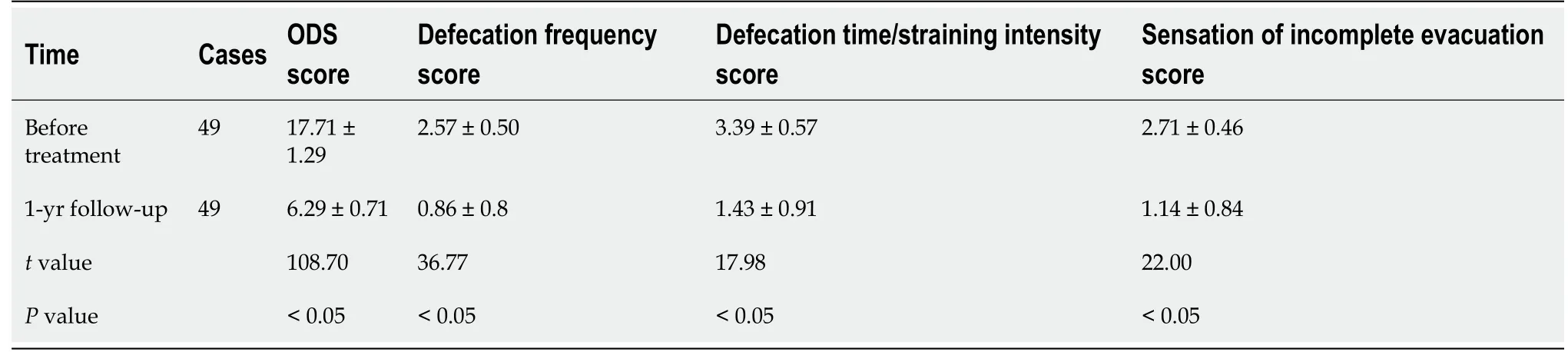
Table 2 Obstructed defecation syndrome scores and main symptom scores in patients before and after treatment
Measurement of anorectal pressure
The anal canal resting pressure and maximum squeeze pressure after the operation were lower than those before treatment,and the differences were statistically significant(P< 0.05).The initial and maximum defecation thresholds of patients after the operation were significantly lower than those before treatment,and the differences were statistically significant(P< 0.05,Table 3).
360° ultrasound measurement in the rectal cavity
The postoperative RC scale,resting phase,and defecati on phase in patients were significantly decreased compared with those before treatment,and the differences were statistically significant(P< 0.05,Table 4).
DISCUSSION
OOC is abnormal defecation caused by abnormal function and morphology of the rectum and anal canal.The main clinical symptoms are difficulty in defecation,incomplete defecation,prolonged defecation time,and the need for manual assistance to defecate.It is commonly found in RC and IRP[11,28].OOC seriously affects people’s normal work,study,and life,in particular female patients with constipation[29].A variety of methods have been used to treat the disease,but due to a series of problems such as postoperative complications and high recurrence rates,satisfactory results have not been achieved.
The TST36 is a new type of large-capacity stapler with an average resected rectal tissue volume of 13.3 cm3(range 8-19 cm3)and an average resected height of 5.18 cm(range 2.5-8 cm).The use of this stapler results in the removal of more tissue[30].The TST36 stapler has an open large window,which provides the surgeon with a good view of the rectal tissue.The surgeon can control the volume of the prolapsed tissue tobe removed through the traction line,to treat better RC and IRP at the same time.It avoids the shortcomings of blind cutting with traditional staplers and improves the safety and effectiveness of the operation[31].
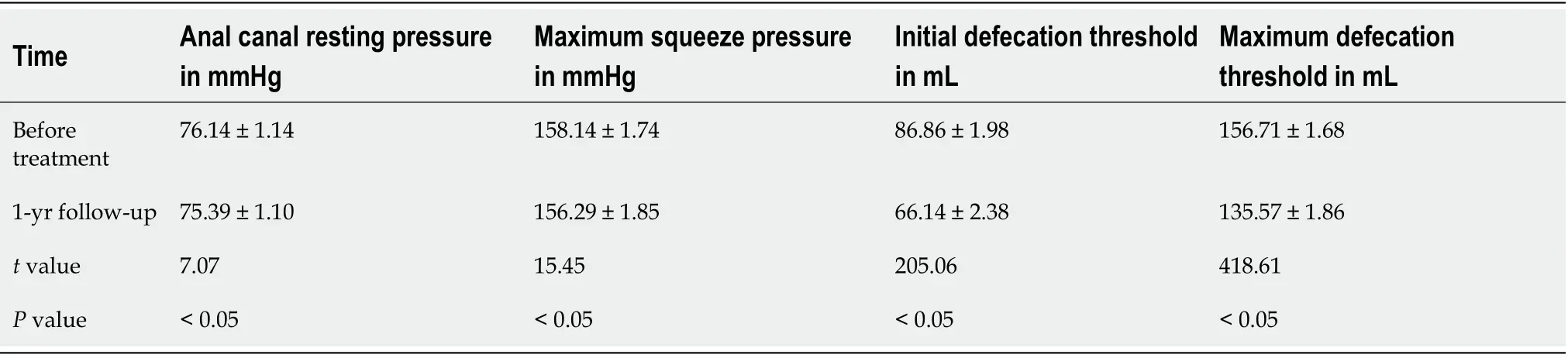
Table 3 Measurement of anorectal pressure before and after treatment

Table 4 360° ultrasound measurement of the degree and depth of rectocele in the rectal cavity
Anal stenosis is the most troublesome postoperative complication,which can result in considerable pain in patients.Our research showed that surgery using the TST36 can avoid anal stenosis.This may be due to the selective removal of prolapsed and protruding rectal tissue under the direct field of view,which can maximize the preservation of normal mucosal bridges,thereby effectively preventing postoperative anal stenosis[32].
The TST36 stapler has an open window,which avoids the shortcomings of blind cutting when using traditional staplers.The surgeon can control the volume of the prolapsed tissue to be removed through the traction line and make corresponding adjustments,without removing or destroying the normal rectal mucosa,thereby effectively reducing the risk of rectovaginal fistula and postoperative hemorrhage caused by excessive removal of rectal mucosa.
The postoperative anal canal resting pressure and maximum squeeze pressure in patients were lower than those before treatment,but the differences were not clinically significant.This suggests that surgery using the TST36 stapler does not affect the function of the internal and external anal sphincter,and normal anal pressure can be maintained after the operation.The initial and maximum defecation thresholds in patients after the operation were significantly lower than those before treatment,and the differences were statistically significant.This suggests that the normal physiological capacity of the rectum can be restored after removal of the prolapsed tissue and the capsular bag of the anterior wall of the rectum,and the anal canal’s anatomical structure can be restored to a greater extent[33].
The etiology of OOC is complicated.However,use of the TST36 stapler to perform surgery in patients with RC combined with IRP reduces the risk of complications,such as anal stenosis and postoperative hemorrhage,and protects the patient’s normal anal function,achieving satisfactory clinical effects.This treatment is worth promoting;however,further long-term follow-up observation is needed to determine its longterm efficacy.
CONCLUSION
The TST36 stapler is safe and effective in treating RC combined with IRP,and it is worthy of promotion for use in clinical work.
ARTICLE HIGHLIGHTS
Research background
The most common causes of outlet obstructive constipation(OOC)are rectocele(RC)and internal rectal prolapse(IRP).The surgical methods for OOC are diverse and difficult,and the postoperative complications and recurrence rate are high,which results in both physical and mental pain in patients.With the continuous deepening of the surgeon’s concept of minimally invasive surgery and continuous in-depth research on the mechanism of OOC,the treatment concepts and surgical methods are continuously improved.
Research motivation
The TST36STARR+ stapler was used to treat patients with RC and IRP.The effects of this stapler in terms of morphology and function after surgery have not been well studied.
Research objectives
This study aimed to assess treatment outcome following use of the TST36 stapler in patients with RC combined with IRP.
Research methods
Forty-nine female patients with RC and IRP who met the inclusion criteria were selected for treatment with the TST36 stapler,and their outcomes were analyzed.
Research results
The cure rate was 92%.The postoperative obstructed defecation syndrome score,defecation frequency score,time/straining intensity,and sensation of incomplete evacuation were significantly decreased compared with these parameters before treatment.The initial and maximum defecation thresholds in patients after surgery were significantly lower than those before treatment.The postoperative ratings of RC,resting phase,and defecation phase were significantly decreased compared with those before treatment.
Research conclusions
The TST36 stapler is safe and effective in treating patients with RC combined with IRP,and it is worthy of promotion in clinical work.
Research perspectives
The TST36 stapler is safe and effective in treating RC combined with IRP,and it is worthy of popularization and continuous improvement in clinical work.
杂志排行
World Journal of Gastrointestinal Surgery的其它文章
- Ewing sarcoma of the jejunum:A case report and literature review
- Biliary drainage in inoperable malignant biliary distal obstruction:A systematic review and meta-analysis
- Liver resection for hepatocellular carcinoma larger than 10 cm:A multi-institution long-term observational study
- Comparison of effects of six main gastrectomy procedures on patients’ quality of life assessed by Postgastrectomy Syndrome Assessment Scale-45
- Practices concerning sleeve gastrectomy in Turkey:A survey of surgeons
- Could neoadjuvant chemotherapy increase postoperative complication risk of laparoscopic total gastrectomy?A monoinstitutional propensity score-matched study in China