Could neoadjuvant chemotherapy increase postoperative complication risk of laparoscopic total gastrectomy?A monoinstitutional propensity score-matched study in China
2021-05-29HaoCuiJianXinCuiYuNingWangBoCaoHuanDengKeChengZhangTianYuXieWenQuanLiangYiLiuLinChenBoWei
Hao Cui,Jian-Xin Cui,Yu-Ning Wang,Bo Cao,Huan Deng,Ke-Cheng Zhang,Tian-Yu Xie,Wen-Quan Liang,Yi Liu,Lin Chen,Bo Wei
Hao Cui,Tian-Yu Xie,School of Medicine,Nankai University,Tianjin 300071,China
Jian-Xin Cui,Bo Cao,Huan Deng,Ke-Cheng Zhang,Wen-Quan Liang,Yi Liu,Lin Chen,Bo Wei,Department of General Surgery,Institute of General Surgery,Chinese PLA General Hospital,Beijing 100853,China
Yu-Ning Wang,First Medical Center,Chinese PLA General Hospital,Beijing 100853,China
Abstract BACKGROUND The potential survival benefit of neoadjuvant chemotherapy(NC)in patients with advanced gastric cancer has been widely recognized.With the development of minimally invasive surgery,which is represented by laparoscopy,the effect of NC on the safety of laparoscopic gastrectomy remains to be further explored.AIM To compare the short-term outcomes of laparoscopic total gastrectomy(LTG)after NC(NC-LTG)with LTG alone.METHODS A total of 92 patients who underwent NC-LTG and 381 patients who received LTG alone at the Chinese PLA General Hospital between September 2015 and September 2020 were retrospectively included in our study.We used propensityscore matching(PSM)to balance baseline bias.After 1:1 PSM,73 patients were included in each group with no statistically significant difference in baseline characteristics.RESULTS The NC-LTG group exhibited a longer operation time(244.10 ± 48.13 min vs 225.74 ± 45.33 min,P = 0.019)and increased intraoperative blood loss [150(100-300)mL vs 100(100-200)mL,P = 0.011] compared to the LTG group.The 30-d postoperative morbidity of the NC-LTG group was 20.5%(15/73),and that of the LTG group was 13.7%(10/73).There were no significant differences in 30-d severe complication rates or anastomotic leakage rates.Subgroup analysis showed that the patients with pTNM(pathological tumor-node-metastasis classification)T0N0-II in the NC-LTG group underwent a longer operation than the LTG group,while no significant difference was found in any perioperative index for the pTNM III patients.A multivariate analysis showed that an operation time longer than 240 min was an independent risk factor(odds ratio = 3.021,95% confidence interval:1.160-7.868,P = 0.024),while NC was not an independent risk factor for postoperative complications in LTG.CONCLUSION Despite a longer operation time and more blood loss after NC-LTG,which indicate surgical difficulty,NC-LTG exhibits acceptable short-term outcomes compared to LTG,suggesting the safety and feasibility of NC-LTG.
Key Words:Neoadjuvant chemotherapy;Gastric cancer;Laparoscope;Total gastrectomy;Morbidity
INTRODUCTION
Gastric cancer is one of the most common malignant tumors and is the fifth most frequently diagnosed tumor and third leading cause of cancer-related deaths,according to GLOBOCAN data updated in 2018[1].People in East Asia are prone to suffer from gastric cancer due to their dietary habits and genetic background.Compared to those in Japan and South Korea,patients in China have lower morbidity but higher mortality,which has become a heavy burden on public health.This outcome is primarily attributed to the decreased popularity of early gastric cancer screening,which leads to a higher proportion of patients with advanced gastric cancer upon diagnosis[2,3].
To improve long-term survival for patients with advanced gastric cancer,integrated perioperative treatment based on radical surgery has recently received gradually increasing attention.Neoadjuvant chemotherapy(NC),a crucial part of integrated perioperative treatment,has attracted attention as an area of frontier research[4,5].Since the MAGIC trial[6] first demonstrated that NC significantly improves progression-free and overall survival of gastric cancer,an increasing number of high-grade evidence-based clinical trials have shown a potential survival benefit of receiving NC due to preoperative downstaging of tumors,appropriate NC regimens,etc.However,in our experience,NC might lead to perigastric tissue effusion and fragility,and the anatomic interval is fuzzy.Therefore,whether NC affects surgical safety remains unclear[10-12].
With the application of laparoscopy for gastrectomy gradually gaining favour,and because of the increasing trend of middle-upper gastric cancer in China[13],laparoscopic total gastrectomy(LTG)has become a common surgical approach,and its surgical safety and feasibility for clinical stage I gastric cancer patients have been demonstrated by the CLASS-02 and KLASS-03 trials[14,15].Many large-volume retrospective studies have demonstrated that LTG has comparable short- and longterm outcomes to open total gastrectomy in advanced gastric cancer patients[16-18].Therefore,we sought to evaluate the short-term outcomes of LTG after NC(NC-LTG)vs LTG alone for pathological stage T0N0-III patients,which can provide reasonable data support for broader application of NC-LTG.
MATERIALS AND METHODS
Patients
This was a single institution retrospective analysis using prospectively collected clinicopathological data from the Department of General Surgery,Chinese PLA General Hospital First Medical Center.The eligible criteria included:(1)Histologically proven gastric cancer by preoperative gastroscopy with a tumor location suitable for LTG;(2)No metastasis according to a preoperative positron emission tomography/computed tomography scan or enhanced abdominal computed tomography scan;(3)Pathological tumor stage ranged from T0N0-III based on the UICC/AJCC 8thguideline[19];(4)No conversion to open total gastrectomy;and(5)Integrated clinical and pathological data.Patients who had severe comorbidities [American Society of Anesthesiologists score(ASA)> III] or other organ resections were excluded from our study.According to the aforementioned criteria,we collected the data for 473 patients who underwent LTG between September 2015 and September 2020.Among these patients,92 individuals underwent NC-LTG(the NC-LTG group),while 381 were treated only by LTG.We adopted double-drug NC regimens,including SOX(TS-1 + oxaliplatin)or XELOX(Xeloda + oxaliplatin),and surgery was performed on patients in the NC-LTG group 4 to 6 wk after the completion of chemotherapy.
Surgical approach
All patients recruited into this study underwent LTG plus D2 lymphadenectomy.The surgical team had extensive experience and perform at least 50 laparoscopic gastrectomies per year;therefore,they each had already overcome the learning curve.The surgical procedure and lymph node dissection were performed in accordance with the Japanese gastric cancer treatment guideline(Ver.5)[20].D2 lymphadenectomy was performed,including Nos.1,2,3,4sa,4sb,4d,5,6,7,8a,9,11p,11d,and 12a,but not No.10.After the intracorporeal procedure,a 7-cm incision made from the middle of the epigastrium was needed to remove the specimen and finish extracorporeal Rouxen-Y anastomosis using a circular stapler for esophagojejunostomy and a linear stapler for jejunojejunostomy.
Data collection and perioperative indicators
Baseline characteristics were recorded,includin g sex,age,body mass index,ASA score,history of abdominal surgery,tumour diameters,pathological tumour stage,tumour differentiation,and the presence of nerve and vascular invasion.During surgery,we determined the estimated blood loss and analyzed the operation time data to evaluate surgical difficulty.We used a propensity-score matching(PSM)method with a 1:1 ratio to reduce baseline bias.
Postoperative indicators are crucial to reflect short-term outcomes.The first flatus day and postoperative hospitalization day were recorded to represent postoperative recovery.Surgical complications occurring within 30 d after the operation were considered in this study.We used the Clavien-Dindo(C-D)classification[21] to evaluate the severe degree of 30-d morbidity.Due to the limitations of retrospective studies,C-D grade I,which was defined as a complication without medical intervention,was not included with data on total morbidity.C-D grade ≥ IIIa was regarded as a severe complication.Anastomotic leakage was observed by the colour and quantity of drainage and was diagnosed by radiological gastroenterography or a second surgery.The R0 resection rate and number of retrieved lymph nodes were acquired from pathological results.
Statistical analysis
SPSS 26.0(SPSS Inc.,Chicago,IL,United States)was used to conduct statistical analyses.Categorical variables were analyzed by Chi-square or Fisher’s exact test,while continuous data were analyzed by Student’s t-test or the Mann-Whitney U test.Because a significant difference in partial baseline characteristics was observed between the NC-LTG and LTG groups,we performed a PSM method with a 1:1 ratio and 0.02 matching tolerance to eliminate baseline bias.Univariate and multivariate logistic regression analyses were used to evaluate risk factors for postoperative complications.A P value < 0.05 was considered statistically significant.
RESULTS
Baseline characteristics
Table 1 shows the baseline characteristics of the NC-LTG and LTG groups.We found that the ASA score was significantly different between the two groups(P = 0.023).After 1:1 matching using a generalized estimating equation model based on the abovementioned clinicopathological indicators,73 patients in each group were ultimately screened,and no significant difference was found in any of the baseline characteristics,which are presented in Table 2.In the NC-LTG cohort,73 patients were administered the SOX(n = 57)or XELOX(n = 16)regimens before LTG,and the chemotherapy effect and potential surgical opportunity were estimated by a multidisciplinary team.In the matched LTG cohort,73 patients underwent LTG without preoperative chemotherapy or radiotherapy.
Intraoperative indicators and postoperative recovery
The NC-LTG group had a longer operation time(244.10 ± 48.13 min vs 225.74 ± 45.33 min,P = 0.019)and increased blood loss [150(100-300)mL vs 100(100-200)mL,P = 0.011],with a significant difference compared to the LTG group.No significant disparity was found in the number of retrieved lymph nodes or the R0 resection rate between the two groups(P > 0.05).When analyzed for postoperative recovery,the NC-LTG and LTG groups had comparable first flatus days and postoperative hospitalization days with no significant difference.
30-d postoperative morbidity and mortality
No patients in the LTG group died on perioperative days,while one patient in the NCLTG group died due to septic shock 4 d after surgery.Although the rate of complications [20.5%(15/73)] in the NC-LTG group was higher than that in the LTG group [13.7%(10/73)],the difference was not significant(P = 0.272).Four patients(two patients in the LTG group and two patients in the NC-LTG group)experienced anastomotic leakage from the esophagojejunostomy site.One patient underwent laparotomy to close the leakage,and the other patients were attended by expectant therapy.The degree of complication severity was evaluated according to the C-D classification,which is shown in Table 3.
We divided all enrolled patients into two subgroups according to different pathological TNM stages.After baseline characteristics showed no significant difference between the NC-LTG and LTG groups in any subgroup,we evaluated the perioperative indexes.In pTNM T0N0-II patients,NC-LTG exhibited a longer operation time compared to the LTG group,while other indicators,including estimated blood loss,number of retrieved lymph nodes,R0 resection rate,first flatus day,postoperative hospitalized day,overall morbidity,and severe morbidity showed no significant differences between the two groups,as shown in Table 4.For pTNM III patients in the two groups,no significant difference was found in any of the indicators mentioned,as presented in Table 5.
Risk factors for overall complications after LTG
Table 6 shows the univariate and multivariate logistic regression results used to explore risk factors for postoperative complications after LTG.NC was not associated with postoperative complications,as shown by univariate analysis(odds ratio = 1.629,95% confidence interval:0.678-3.913,P = 0.275).We placed indicators obtained by univariate regression with P > 0.25 into the multivariate analysis and found that an operation time ≥ 240 min was a significant independent risk factor for overall postoperative complication(odds ratio = 3.021,95% confidence interval:1.160-7.868,P = 0.024).

Table 1 Baseline characteristics of laparoscopic total gastrectomy after neoadjuvant chemotherapy group and laparoscopic total gastrectomy group before propensity-score matching
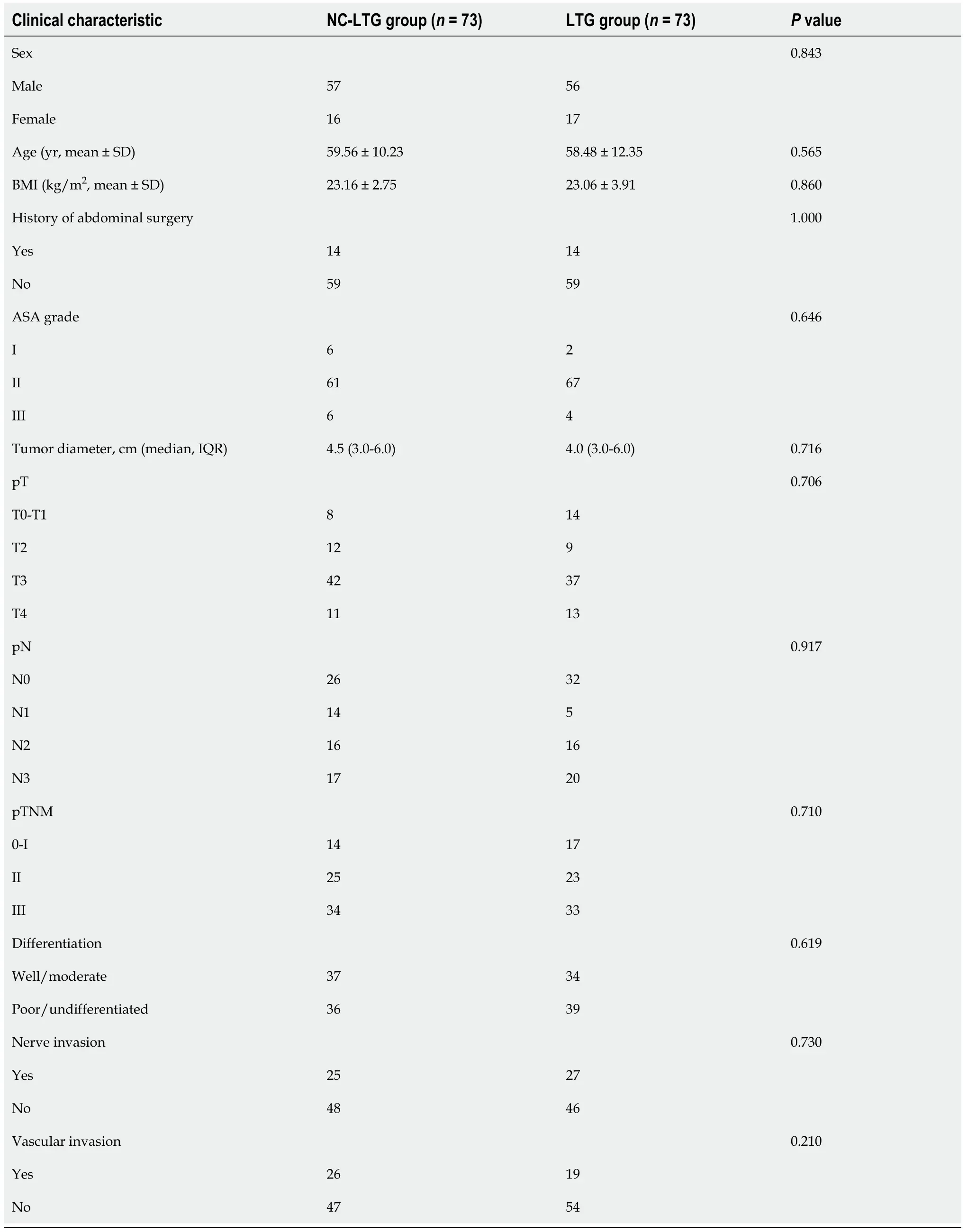
Table 2 Baseline characteristics of laparoscopic total gastrectomy after neoadjuvant chemotherapy group and laparoscopic total gastrectomy group after propensity-score matching
DISCUSSION
NC is currently a hotspot of integrated therapy for advanced gastric cancer.Many studies have demonstrated that preoperative chemotherapy previously applied in European countries can reduce the tumour clinical stage and even lead to pathological complete response,showing oncological benefit because of the elevated R0 resection rate[6,22].People in East Asia have a high risk of gastric cancer,and radical gastrectomy followed by postoperative chemotherapy is still regarded as the standard treatment for advanced gastric cancer patients[20,23].However,a lower incidence of tolerance and compliance in patients who receive chemotherapy after gastrectomy represents an obstacle to prolonged survival.NC may change this situation;therefore,continuous high-quality randomized controlled trial studies,such as JCOG-0405[24],JCOG-1002[25],and JCOG-0501[26] studies conducted by the Japan Clinical Oncology Group,the RESOLVE[7] and the RESONANCE[9] trials conducted in China,and the PRODIGY trial[8] conducted in South Korea,have been recently performed,providing theoretical support for the optimal selection of NC regimen and exploring appropriate indications,especially for patients in East Asia.
The reasonable application of laparoscopy as a representative minimally invasive surgery was initially proven safe and feasible.With respect to LTG,CLASS-02 and KLASS-03 studies[14,15] simultaneously demonstrated that LTG and open total gastrectomy(OTG)exhibited comparable short-term outcomes in clinical stage I patients.Large-scale retrospective studies also showed that LTG was comparable to OTG in terms of short- and long-term outcomes in both early and advanced gastric cancer patients[18].Recently,surgeons have started to focus on the effects of NC associated with laparoscopic gastrectomy.Li et al[27] found that laparoscopic distal gastrectomy after NC significantly reduced postoperative complication rates and led to better chemotherapy tolerance than open distal gastrectomy.The STOMACH trial[28] conducted by European multi-institutional medical centres showed that open surgery or LTG after NC led to comparable short-term outcomes and non-inferiority in terms of 1-year overall survival.Shuai et al[29] demonstrated that NC was safe and feasible after laparoscopic gastrectomy for advanced gastric cancer,while it increased the R0 resection rate and reduced tumour stage.An international cohort study also presented similar results[30].However,few studies have reported the effect of NC on the short-term efficacy of LTG,and this issue requires further evaluation.In our study,we present our single institution data aimed at determining the perioperative safety of NC-LTG compared to LTG alone in gastric cancer patients.
There is consistent controversy regarding whether NC increases surgical difficulty.Some perspectives consider that NC may cause perigastric tissue oedema and fibrillation,lead to fragility of normal tissue,a fuzzy anatomic interval,etc.,resulting in surgical complications[31].An initial study conducted by our medical centre demonstrated that gastrectomy after NC exhibited a longer operation time and a higher proportion of patients with estimated blood loss greater than 200 mL compared to those undergoing surgery without chemotherapy[32].However,Shuai et al[29] indicated that NC did not significantly increase the surgical time or quantity of blood lost during laparoscopic gastrectomy.In the present study,the NC-LTG group had a significantly prolonged surgical time and more blood loss than the LTG group.Results of the subgroup analysis showed that patients in pathological stage T0N0-II in the NCLTG group had a longer operation time,while no significant difference was found in patients at pathological stage III in the LTG and NC-LTG groups.In terms of estimated blood loss,there was no significant difference between the two groups,regardless of the pathological stage of the patients.The potential reason for this outcome might be that patients with early pathological stages and receiving NC were sensitive to the chemotherapy or endured a longer cycle of preoperative treatment,causing tissue exudation and oedema,which increased the difficulty of the surgery.In contrast,early-stage patients in the LTG group had relatively easy surgeries.
Radical surgical resection and a sufficient number of retrieved lymph nodes can remarkably promote long-term prognosis in gastric cancer.Our research found that the R0 resection rate was 90.4%(66/73)in the NC-LTG group and 94.5%(69/73)in the LTG group with no obvious imparity,indicating that NC-LTG has an effect on radical resection equal to the effect of LTG alone.Lymph nodes can better reflect the oncological quality of resection.In our study,no significant difference was found in the number of lymph nodes retrieved between the NC-LTG and LTG groups,which demonstrates that NC-LTG and LTG have comparable capacities for lymph node resection.
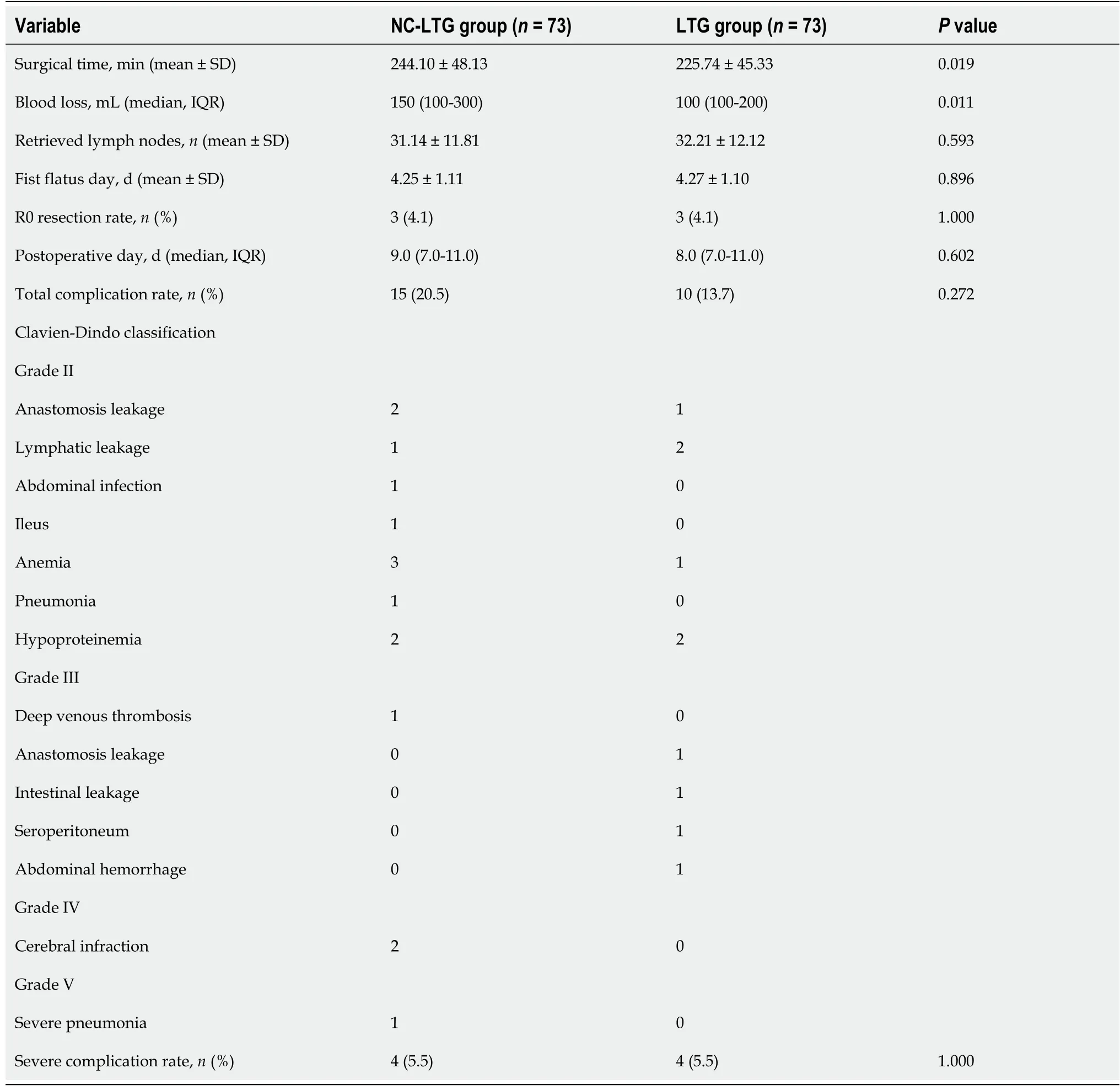
Table 3 Surgical indicators in perioperative days between laparoscopic total gastrectomy after neoadjuvant chemotherapy and laparoscopic total gastrectomy group
Postoperative complications are crucial indicators for evaluating short-term outcomes.Previous studies have shown that there was no significant difference in postoperative morbidity caused by NC after gastrectomy[11,33-35];however,few studies have focused on short-term outcomes after LTG with NC.In this study,we found that the overall postoperative morbidity in the NC-LTG group was 20.5%(15/73),while it was 13.7%(10/73)in the LTG group.The subgroup analysis illustrated that for patients in pathological stage T0N0-II or III,no significant correlation was observed between overall or severe morbidity and NC.Moreover,anastomosis leakage is a common complication after total gastrectomy that is correlated with perioperative mortality and further recurrence[36,37].A single-arm study from Japan showed that the anastomosis leakage rate after laparoscopic total or proximal gastrectomy for early-stage patients was 2.5%[38].Another large-scale retrospective study demonstrated that the anastomosis leakage rate in stage I patients was 5.4%,while that in stages II-IV patients was 5.7% after LTG[39].In the present study,the anastomosis leakage rate in both the NC-LTG and LTG groups was not significantly different at 2.7%.Based on the above research,the occurrence of anastomosis leakage did not seem to be associated with NC in LTG,indicating thatapplication of LTG is safe and feasible after NC.

Table 4 Clinical characteristics and surgical indicators in pTNM 0-II patients between laparoscopic total gastrectomy after neoadjuvant chemotherapy and laparoscopic total gastrectomy group
Some inherent limitations exist in this research.First,this was a single institution retrospective study with potential selection bias.Prospective studies can be conducted based on our previous results to provide more reliable evidence.Second,even though we utilized the PSM method to reduce baseline characteristic bias between the NCLTG and LTG groups,there were still some potential factors that may have influenced the short-term outcomes.Third,due to uncertainty of the preoperative clinical stage[40],we recorded only postoperative pathological stage to ensure that we could evaluate perioperative outcomes after LTG with NC or not at the current pathological stage.The final limitation is that we unified pTNM T0N0-II stage patient data into one group due to the small sample size in the subgroup analysis.Further studies need to expand the sample size to analyze significant differences in perioperative indicators based on explicit pathological stage.
Despite these limitations,to our knowledge,few preliminary studies in addition to that presented herein,have reported short-term effects of NC-LTG in China.After PSM,we found that although NC-LTG was found to be associated with prolonged operation time and increased intraoperative blood loss,which increased surgical difficulty to a certain extent,no significant difference was observed between NC-LTG and LTG with respect to the number of retrieved lymph nodes or 30-d postoperative morbidity,indicating that the NC does not increase the risk of LTG and is a safe and feasible operation.However,the long-term oncology efficacy needs to be further evaluated.
CONCLUSION
Despite a longer operation time and more blood loss after NC-LTG,which indicate surgical difficulty,NC-LTG exhibits acceptable short-term outcomes compared to LTG,illustrating the safety and feasibility of NC-LTG.
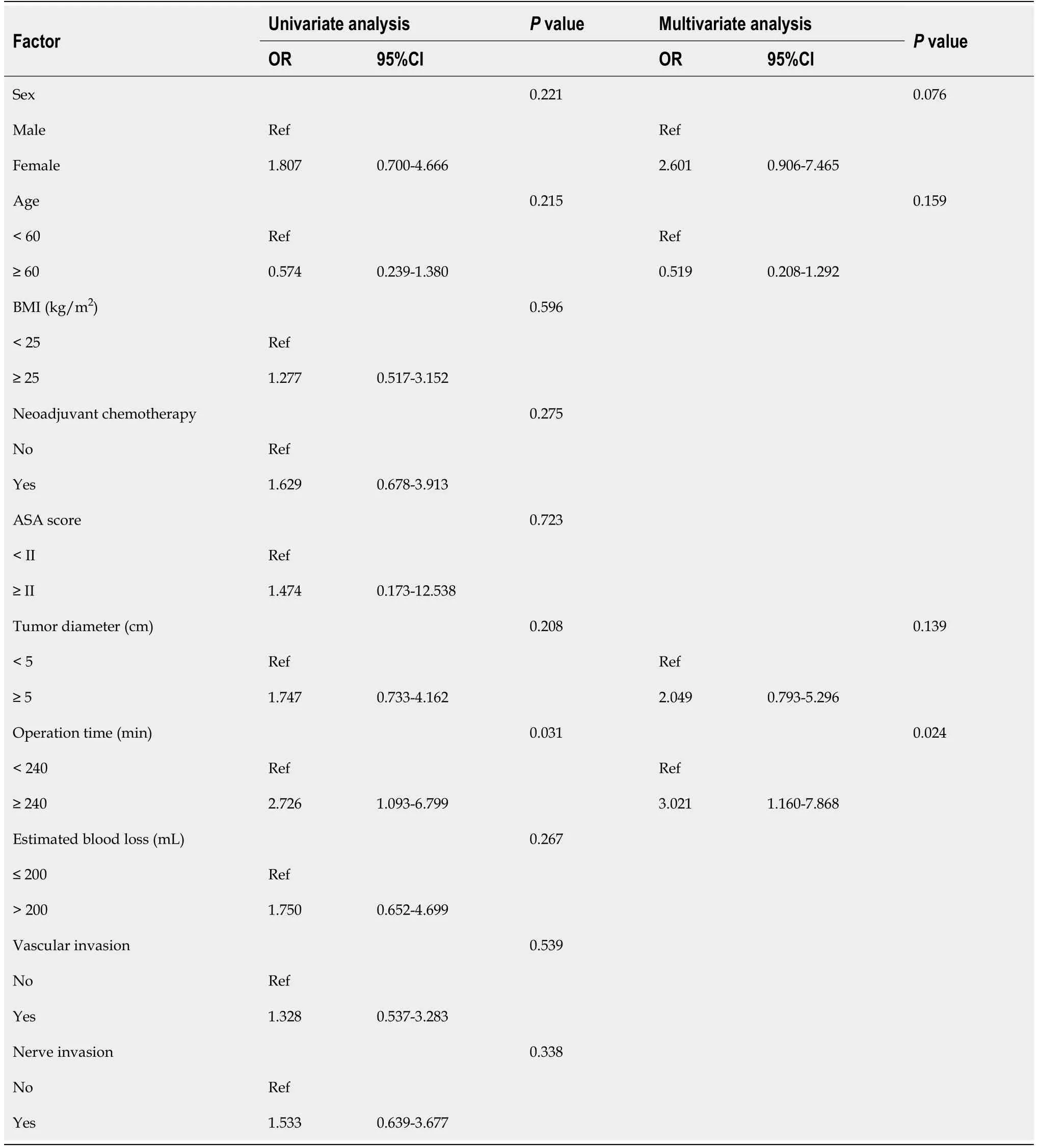
Table 6 Univariate and multivariate logistic regression analyses for postoperative complications in laparoscopic total gastrectomy patients
ARTICLE HIGHLIGHTS
Research background
The potential survival benefit of neoadjuvant chemotherapy(NC)in patients with advanced gastric cancer has been widely recognized.
Research motivation
With the development of minimally invasive surgery,which is represented by laparoscopy,the effect of NC on the safety of laparoscopic gastrectomy remains to be further explored.
Research objectives
To compare the short-term outcomes of laparoscopic total gastrectomy(LTG)after NC(NC-LTG)with LTG alone.
Research methods
A total of 92 patients who underwent NC-LTG and 381 patients who received LTG alone at the Chinese PLA General Hospital between September 2015 and September 2020 were retrospectively included in our study.We used propensity-score matching(PSM)to balance baseline bias.After 1:1 PSM,73 patients were included in each group with no statistically significant difference in baseline characteristics.
Research results
The NC-LTG group exhibited a longer operation time and increased intraoperative blood loss compared to the LTG group.There were no significant differences in 30-d postoperative morbidity,30-d severe complication rates,or anastomotic leakage rates.A multivariate analysis showed that an operation time greater than 240 min was an independent risk factor while NC was not an independent risk factor for postoperative complications in LTG.
Research conclusions
Despite a longer operation time and more blood loss after NC-LTG,which indicate surgical difficulty,NC-LTG exhibits acceptable short-term outcomes compared to LTG,illustrating the safety and feasibility of NC-LTG.
Research perspectives
Further research like multi-institutional retrospective study or randomized controlled trial study is needed to confirm our results and provide high-grade evidence for the appropriate application of NC-LTG.
杂志排行
World Journal of Gastrointestinal Surgery的其它文章
- Ewing sarcoma of the jejunum:A case report and literature review
- Biliary drainage in inoperable malignant biliary distal obstruction:A systematic review and meta-analysis
- Liver resection for hepatocellular carcinoma larger than 10 cm:A multi-institution long-term observational study
- Comparison of effects of six main gastrectomy procedures on patients’ quality of life assessed by Postgastrectomy Syndrome Assessment Scale-45
- Practices concerning sleeve gastrectomy in Turkey:A survey of surgeons
- Therapeutic effects of the TST36 stapler on rectocele combined with internal rectal prolapse