Population-level economic burden of lung cancer in China:Provisional prevalence-based estimations,2017-2030
2021-03-13ChengchengLiuJufangShiHongWangXinxinYanLeWangJiansongRenMarkParascandolaWanqingChenMinDai
Chengcheng Liu,Jufang Shi,Hong Wang,Xinxin Yan,Le Wang,Jiansong Ren,Mark Parascandola,Wanqing Chen,Min Dai
1Office of Cancer Screening,National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital,Chinese Academy of Medical Sciences and Peking Union Medical College,Beijing 100021,China;2 Tobacco Control Research Branch,Division of Cancer Control and Population Sciences/National Cancer Institute,Bethesda,MD 20852,USA
Abstract Objective:Population-level economic burden is essential for prioritizing healthcare resources and healthcare budget making in the future.However,little is known about the economic burden of lung cancer in China.Methods:A prevalence-based approach was adopted to estimate the economic burden of lung cancer,including direct expenditure (medical and non-medical) and indirect cost (disability and premature death).Data on direct expenditure and work-loss days per patient in each year post-diagnosis were obtained from two primary surveys.Other parameters were obtained from literatures and official reports.Projections were conducted based on varying parameters.All expenditure data were reported in United States dollars (USD) using 2017 value (exchange rate:1 USD=6.760 CNY),with the discount rate of 3%.Results:The total economic burden of lung cancer was estimated to be 25,069 million USD in China in 2017(0.121% of gross domestic productivity,GDP).The estimated direct expenditure was 11,098 million USD,up to 1.43% of total healthcare expenditure for China,covering 10,303 million USD and 795 million USD for medical and non-medical expenditure,respectively.The estimated indirect cost was 13,971 million,including 1,517 million USD due to disability and 12,454 million USD due to premature death.Under current assumptions,the projected total economic burden would increase to 30.1 billion USD,40.4 billion USD,and 53.4 billion USD in 2020,2025,and 2030,accounting for 0.121%,0.131%,and 0.146% of China’s GDP,respectively.However,if China meets the United Nation sustainable development goal of reducing premature death from non-communicable diseases by one-third by 2030,the total economic burden in 2030 would be 31.9 billion USD,0.087% of China’s GDP.Conclusions:The economic burden of lung cancer in China in 2017 is substantial and more likely to increase significantly in the future.Policy makers need to take urgent actions in budget making for health systems.The economic burden could be alleviated by reducing the disease burden of lung cancer via effective control and prevention actions.
Keywords:Lung cancer;cost of illness;China;population-level;prevalence
Introduction
Lung cancer,as a major global health threat,has been the leading cause of cancer incidence and mortality throughout the world,with more than 2.1 million new cases and 1.8 million deaths in 2018 (1).In particular,more than one third of all newly diagnosed lung cancers and nearly 40% of deaths globally occurred in China,and the number is expected to increase in the future (1,2).It is inevitable for lung cancer patients to utilize costly medical services with non-medical spending and experience productivity loss for themselves and their caregivers.Thus,the economic consequences of lung cancer and its trends in the future,including the direct and indirect cost are increasingly drawing the attention from both the government and the public.
Quantifying the comprehensive economic burden of lung cancer in the population level both at the present and in the future is a critical first step to inform cancer control strategies (3).The European Union (EU),the United States (US) and Korea have established a scientificallydesigned platform and methodology for estimating and projecting the population-level cost of cancer (4-8).In the US,the direct medical expenditure associated with lung cancer was $20.10 billion in 2015 and this figure is expected to increase (6).In Korea,the total economic burden of lung cancer is $1.9 billion (7).These estimations and projections of the economic burden of lung cancer in foreign countries have provided valuable evidence for local policymaking and resource allocation.However,data on the economic burden of lung cancer in China have always been sparse,and little is known about the projections(9,10).
Therefore,to address these gaps,using a prevalencebased approach,we estimated the comprehensive economic burden of lung cancer in China from 2017 to 2030 at population level.
Materials and methods
Study design
A prevalence-based cost-of-illness approach was used to estimate the annual economic burden of lung cancer in China from 2017 to 2030,including direct (medical and non-medical) expenditure and indirect cost (Figure 1A)(3,9,11,12). Direct medical expenditure includes all payments for healthcare services to manage lung cancer,while direct non-medical expenditure refers to the other spending on patient’s diagnosis and treatment,including additional meals,nutrition,transportation,accommodation,hired informal nursing and other expenditures.Indirect cost covers the value of lost productivity due to disability and premature death from lung cancer.
Data source
Individual direct expenditure,and work-loss days associated with lung cancer
Medical expenditure data were obtained from a hospitalbased multicenter lung cancer retrospective clinical epidemiological survey in 2015-2016 in China (13).As previously described,a convenience sampling was conducted across the seven geography regions classified by the National Bureau of Statistics,including Shanxi,Liaoning,Anhui,Zhejiang,Hunan,Guangxi,Yunnan,and Gansu (13,14).Lung cancer patients who were primarily diagnosed by pathology between 2005 and 2014 were included if they underwent main treatments in surveyed hospital with complete medical record data (13).Information of socio-demographics and risk factors,clinical characteristics and medical expenditure due to lung cancer diagnosis and treatment for all clinical visits,was collected through the hospital’s electronic medical record system(13).To present annual medical expenditure data with better robustness,information from a sub-set containing 7,052 primary lung cancer patients were applied for this analysis.
Non-medical expenditures and work-loss days were acquired from a multicenter,cross-sectional survey among hospitalized lung cancer patients conducted in 13 provinces,municipalities,and autonomous regions(including Shandong,Beijing,Jiangsu,Guangdong,Zhejiang,Hebei,Liaoning,Hunan,Heilongjiang,Henan,Xinjiang,Gansu and Chongqing),using a structured questionnaire by face-to-face interview (9,15).Nonmedical expenditure covered additional meals,nutrition,transportation,accommodation,hired informal nursing and other expenditures.Work-loss days of lung cancer were acquired both from patients and their caregivers.To acquire robust non-medical expenditure and work-loss days,information from a sub-set containing 1,145 patients was applied in the current analysis.
Other data sources
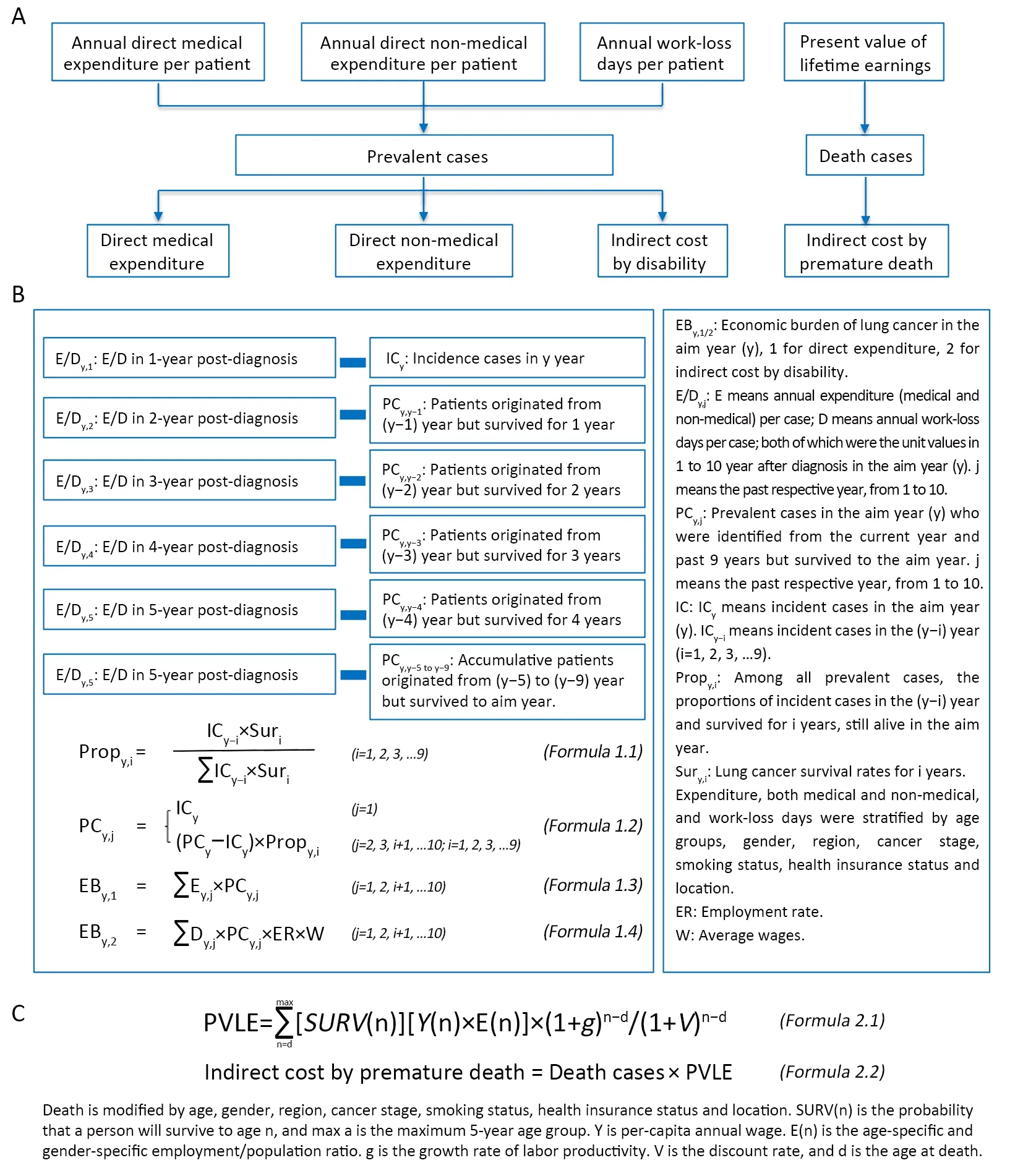
Figure 1 Methodology estimating overall population-level economic burden of lung cancer in China.(A) Overall framework for economic burden of lung cancer;(B) Methods to estimate direct expenditure and indirect cost by disability of lung cancer;(C) Methods to estimate indirect cost by premature death of lung cancer.
The disease burden of lung cancer was obtained from the GBD 2017 (16) (Supplementary Table S1). Detailed distributions of prevalent cases among various subgroups were estimated by use of proportions in the multicenter hospital-based survey of lung cancer (13).Survival rates of lung cancer,serving as parameters to calculate proportions of prevalent cases in each year,were extracted from reports based on national cancer registries (17) and other population-based studies (18).Additionally,age-specific survival rates for general population were from the 2015 China Life Tables from World Health Organization(WHO) (19).The employment rates for populations in China in 2010 were applied (20).The estimated future population size was obtained from the United Nations(UN) World Population Prospects (21) (Supplementary Table S2).
Estimation for economic burden
Direct expenditure and indirect cost by disability
The annual medical expenditure per prevalent lung cancer patient was calculated for each 12-month period after the first diagnosis (9,11).To ensure the robustness of annual expenditures (medical and non-medical) and work-loss days,the analyzed sample for each year post-diagnosis should be greater than 50. Thus,annual medical expenditure for the 1st to the 5th year post-diagnosis was presented.Expenditure in the 6th to the 10th year postdiagnosis was considered the same as those in the 5th year post-diagnosis.Among the included 7,052 cases for medical expenditure,5,156 (73%) were male patients,and most cases (90%) were diagnosed with age above 45 years old.In terms of region area,cases from the east,central,and west area were relatively balanced,with cases of 1,980 (28%),2,360 (33%),and 2,712 (38%).Additionally,most cases were diagnosed with late stages,with cases of 2,398 (34%)and 2,078 (29%) at stage III and stage IV,respectively(Supplementary Table S3).The overall medical expenditures from Year 1 to Year 5 were 9,635 USD,5,643 USD,5,581 USD,4,975 USD and 5,414 USD,respectively (Supplementary Table S3).
As for the 1,145 cases for non-medical expenditure and work-loss days with 788 (69%) male cases of total surveyed participants,nearly 91% of cases were diagnosed with age over 45 years old.Cases from the east ranked the first (630,55%),followed by cases from the west (321,28%),with the lowest cases from the central (194,17%).Cases in late stage could account for majority of all,with cases of 318(28%) and 529 (46%) in stage III and stage IV(Supplementary Table S4).Given the data availability,annual non-medical expenditure and work-loss days for the Year 1 to Year 3 were presented,while data for the Year 4 to Year 10 post-diagnosis were considered the same as those in the 3rd year post-diagnosis.The prevalent cases were also divided into 10 groups,including newlydiagnosed cases in the aim year and surviving cases originating from each previous year,as in Yearym-9,based on Formula 1.1 and Formula 1.2 inFigure 1B.The overall non-medical expenditure from Year 1 to Year 3 were 748 USD,459 USD,and 394 USD,respectively.The overall work-loss days from Year 1 to Year 3 were 66 d,54 d,and 39 d,respectively (Supplementary Table S4).
Estimations for direct expenditure and indirect cost were based on the assumption that the direct expenditure and indirect cost associated with disability in the aim year resulted from prevalent cases of patients who were diagnosed within the last 10 years,including newly diagnosed patients in the aim year and surviving patients diagnosed in previous years (11).Under this assumption,the direct (medical and non-medical) expenditure was estimated by summarizing the products of annual direct expenditure and matched prevalent cases in corresponding years after diagnosis (Formula 1.3 inFigure 1B).Indirect cost by disability (IDIS) was estimated by summarizing the products of annual work-loss days,matched prevalent cases in each year post-diagnosis,employment ratios,and daily wages (Formula 1.4 inFigure 1B).
All expenditure data were discounted to 2017 at a rate of 3% and presented in USD,together with an annual growth rate of 2.2% (22).
Indirect cost by premature death (IPD)
IPD was estimated for lung cancer patients aged from 15 years old (working age) to the life expectancy (male:74.5 years old and female:80.0 years old) (16).First,the present value of lifetime earnings (PVLE) was estimated via 5-year age groups by the human capital approach (23).A discount rate of 3% was used to convert future earnings into current worth.Taking the potential growth of future earnings into account,an annual productivity growth rate of 9.8% was assumed by referring to the annual change of gross domestic productivity (GDP) in the last 3 years (9).Second,IPD was estimated from the products of cancer death cases and PVLE (Formula 2.1-2.2 inFigure 1C)
Prediction of future economic burden
The disease burden of lung cancer in China was projected based on population numbers and rates of incidence,prevalence,and mortality.To account for changes in the disease burden of lung cancer with aging and urbanization,population numbers based on the medium fertility variant from the UN World Prospects were applied (21).Three scenarios were adopted to project the disease burden of lung cancer in China in the future (12):1) In the base case scenario,we assumed that changes in aging and urbanization are the only drivers of disease burden;2) In the main body scenario,the disease burden of lung cancer was further projected based on the current status in 2017 and rates of changes in the past trend.Mean annual change rates in the age-and sex-specific incidence,prevalence and mortality in China were estimated using data from the Global Burden of Disease (GBD) 2017 for the years 2000,2005,2010,2015 and 2017;3) Target scenario was only set for 2030.In the target scenario,we explored the predicted economic burden in 2030 under the realization of goals in disease prevention and control for lung cancer.Target 1 was assumed under Sustainable Development Goals (SDG)3.4 proposed by the UN Agenda,in which the premature mortality from non-communicable diseases in 2030 would decrease by one-third from their 2015 levels (24).Here,the non-communicable diseases were limited to lung cancer and the baseline year was 2017.Given the interactions among mortality,incidence,and prevalence,reductions were predicted to occur simultaneously for these three indicators.Moreover,under the SDG assumption,target 2 was estimated with a reduction only in lung cancer mortality.Target 3 was assumed to have a 15% increase in the survival rate for lung cancer patients,the goal set by Healthy China 2030 (25).
Annual expenditure per patient (medical and nonmedical) was projected by the annual growth rate of 2.2%,while constant work-loss days were input (22).The annual growth rate for annual earnings was assumed to be the increase of GDP based on the forecast from the Organization for Economic Co-operation and Development (OECD) (26).
Parameters for sensitivity analysis
Uncertainty in economic burden from 2017 to 2030 was explored by one-way sensitivity analyses.The impact of these variations was quantified by the relative change in the percent of the total economic burden attributed to a given parameter.An annual growth rate of 5.6% for direct expenditure per capita,observed from a multicenter hospital-based retrospective clinical epidemiological survey of lung cancer,was input to test the impact (13).Expenditure patterns of lung cancer are scarcely reported in China.In the US,lung cancer expenditure could be classified based on the initial,continuing,and end of life periods,and a“J”shape could be found across three periods (6).In Australia,the“J”shape among expenditure across three periods is also observed,although the annual expenditure since the 4th diagnosis decreases substantially(11).To test the impact by expenditure pattern,data from the US and Australia were applied.Annual productivity growth rate could be easily influenced by the economic environment.Based on the OECD estimates of GDP from 2015 to 2017,an annual growth rate of 6.8% was applied as a conservative estimation (26).Furthermore,given the special circumstances,such as the economic situation under the coronavirus disease 2019 (COVID-19) pandemic,we assumed the worst productivity/earnings growth rate of the-6.8%,based on GDP in the first quarter in China (27).Distinct ranges of working age,including 16-60 years old for males and 16-55 years old for females required by China (28),15-64 years old defined by OECD (20) and 30-69 years old recommended by a global estimation (29),were tested for their impact on the estimation of indirect cost.Data from Cancer Tomorrow in GLOBOCAN 2018 were used to evaluate the potential influence of the data source (30).
Results
Economic burden in 2017
The total estimated economic burden of lung cancer in 2017,including direct expenditure and indirect cost,was 25,069 million USD,equivalent to 0.121% of the local GDP of China in 2017 (Table 1) (26).If we adopted the GDP from the China Statistical Yearbook,the share of GDP would be 0.205% (14).The total estimated direct expenditure,including direct medical expenditure and direct non-medical expenditure,was 11,098 million USD,which is approximately 1.43% of total healthcare expenditure (31) in China for 2017 (Table 1).The total direct medical expenditure and direct non-medical expenditure were 10,303 million USD and 795 million USD,respectively.The total estimated indirect cost,covering the IDIS and IPD,was 13,971 million USD,accounting for 55.7% of the total economic burden,of which 89.1% resulted from IPD (Figure 2).Younger patients bore more of the burden caused by IPD,with the proportions of 85.5% and 68.7% in the age groups <45 years and 45-59 years,respectively (Figure 2).
The total economic burden increased with age,with patients over 60 years old accounting for 51.3% of the burden.Male patients constituted 71.9% of the economic burden.Compared with the burden in central and western regions,the economic burden was the highest in east regions (16,259 million USD),accounting for 64.9% of the total.Patients diagnosed in later stages (stage III and IV)(16,282 million USD) bore a greater burden than those diagnosed in early stages (stage I and II) (8,787 million USD).Moreover,the economic burden attributed to lung cancer patients with a smoking history was 14,361 million USD,representing 57.3% of the total economic burden.In terms of health insurance,compared with patients withurban employee basic medical insurance (UEBMI) (4,744 million USD) and urban resident basic medical insurance(URBMI) (1,013 million USD),patients with insurance from the new rural cooperative medical system (NRCMS)(6,346 million USD) and self-pay (5,522 million USD)represented a larger economic burden.The patterns in the subgroups for direct medical expenditure,direct nonmedical expenditure,IDIS and IPD followed a distribution similar to the total burden (Table 1,Figure 2).
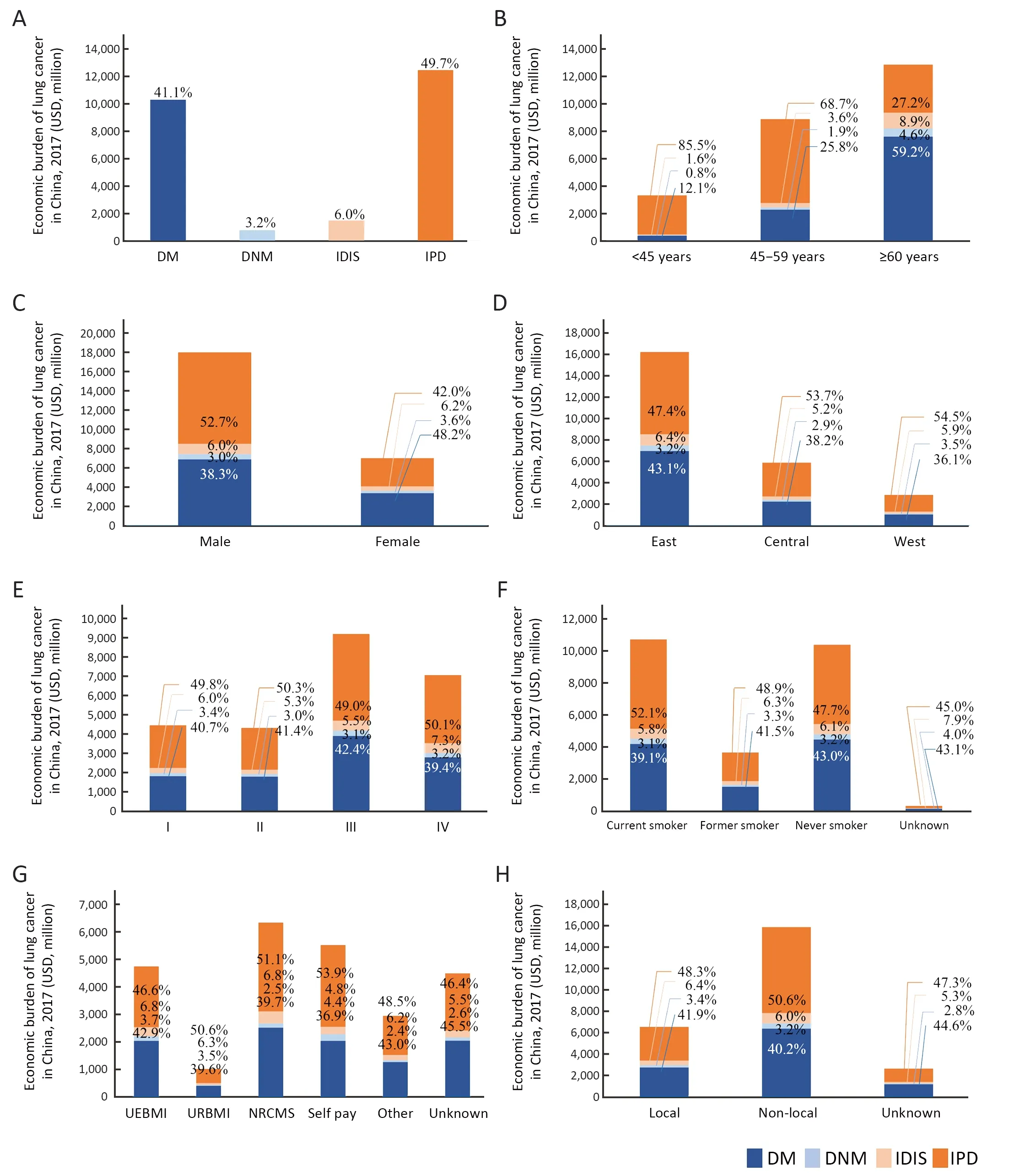
Figure 2 Break-downs of population-level economic burden of lung cancer in China in 2017,by subgroup.(A) Overall;(B) by age;(C) by gender;(D) by region;(E) by cancer stage;(F) by smoking status;(G) by health insurance status;(H) by health insurance location.DM,direct medical expenditure;DNM,direct non-medical expenditure;IDIS,indirect cost by disability;IPD,indirect cost by premature death.
Economic burden in 2020-2030
In the main body scenario,the estimated economic burden of lung cancer in China for 2020,2025,and 2030 was 30.1 billion USD,40.4 billion USD,and 53.4 billion USD,representing up to 0.121%,0.131%,and 0.146% of China’s GDP,respectively.Based on GDP long-term forecast from OECD,the GDP for China in 2020,2025,and 2030 were 168,218.9 billion USD,208,948.6 billion USD,and 247,928.3 billion USD,respectively (26).Compared with the burden in 2017,it would increase by 20.1%,61.2%,and 113.1%,respectively.In contrast,if the only drivers were population aging and urbanization,the economic burden of lung cancer in China for 2020,2025 and 2030 would be 29.6 billion USD,38.2 billion USD,and 47.8 billion USD,respectively (Figure 3,4).
However,if China meets the UN goal of a one-third reduction in premature death from non-communicable diseases (focusing on lung cancer here),together with a similar reduction in the prevalence and incidence rates,the economic burden of lung cancer in 2030 would decrease to 31.9 billion USD (approximately 0.087% of China’s GDP),with a reduction of 40.3% relative to the main body scenario in 2030.Even if the reduction were confined to reducing mortality by one-third,the economic burden would decrease by 14.4% (45.7 billion USD).In addition,if the goal set by Healthy China 2030 was achieved,with a 15% increase in the cancer survival rate,the economic burden would be 46.7 billion USD,which is 12.6% lower than that in the main body scenario for 2030 (Figure 3).
Sensitivity analysis
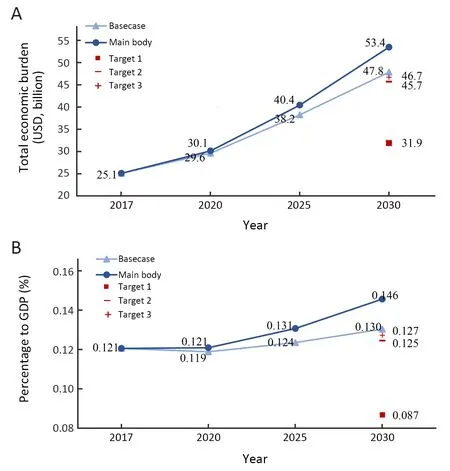
Figure 3 Projections for population-level economic burden of lung cancer in China.(A) total economic burden;(B) percentage to GDP of China.GDP,gross domestic productivity.GDP was from Organization for Economic Co-operation and Development.
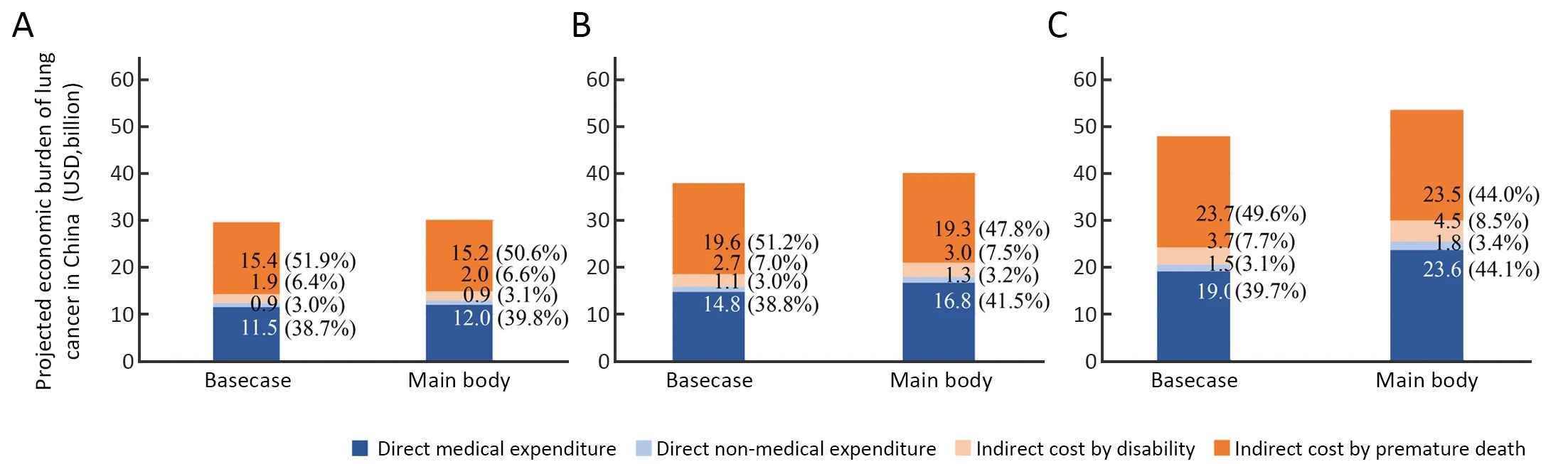
Figure 4 Break-downs of projected economic burden of lung cancer in China,in 2020 (A),2025 (B) and 2030 (C).
The range of working age plays an important role both in the estimation of economic burden in 2017 and in projections.If we adopted the range of working age from China’s official recommendation 16-60 years for males and 16-55 years for females,the economic burden would be reduced by more than 40%.Moreover,economic burden could be easily influenced by the annual productivity growth rate due to the economic environment.In the conservative estimation with annual productivity growth rate of 6.8%,10.0%-15.0% declines for economic burden were observed.However,in the worst scenario,such as the current situation under COVID-19 with annual productivity growth rate of -6.8%,the economic burden could be reduced by over 30.0%.When we applied expenditure patterns by period in US,the economic burden would be 28.6 billion USD,which is higher than our estimation of 14.2% in decline. Regarding medical expenditure pattern by years’ post-diagnosis in Australia,the burden would be 23.7 billion USD,which is reduced by 5.6% (Data was not shown in theTable 2).In addition,if medical expenditure rises at a faster annual rate (5.6%),the economic burden would have been expected to grow by 10.3% in 2017.Moreover,the economic burden would be projected to rise by at least 33.6% when we use the disease burden of lung cancer from Cancer Tomorrow in GLOBOCAN 2018 (30) (Table 2).
Discussion
By using prevalence-based approaches,this study determined the comprehensive economic burden of lung cancer in China from 2017 to 2030 at the population level,which can provide a reference for evidence-based policymaking in cancer prevention and control.The estimated economic burden of lung cancer in China in 2017 was 25.1 billion USD,accounting for 0.121% of the local GDP,and is projected to increase significantly in the future.However,if the target for the prevention and control of lung cancer could be achieved by 2030,the economic burden would be mitigated.
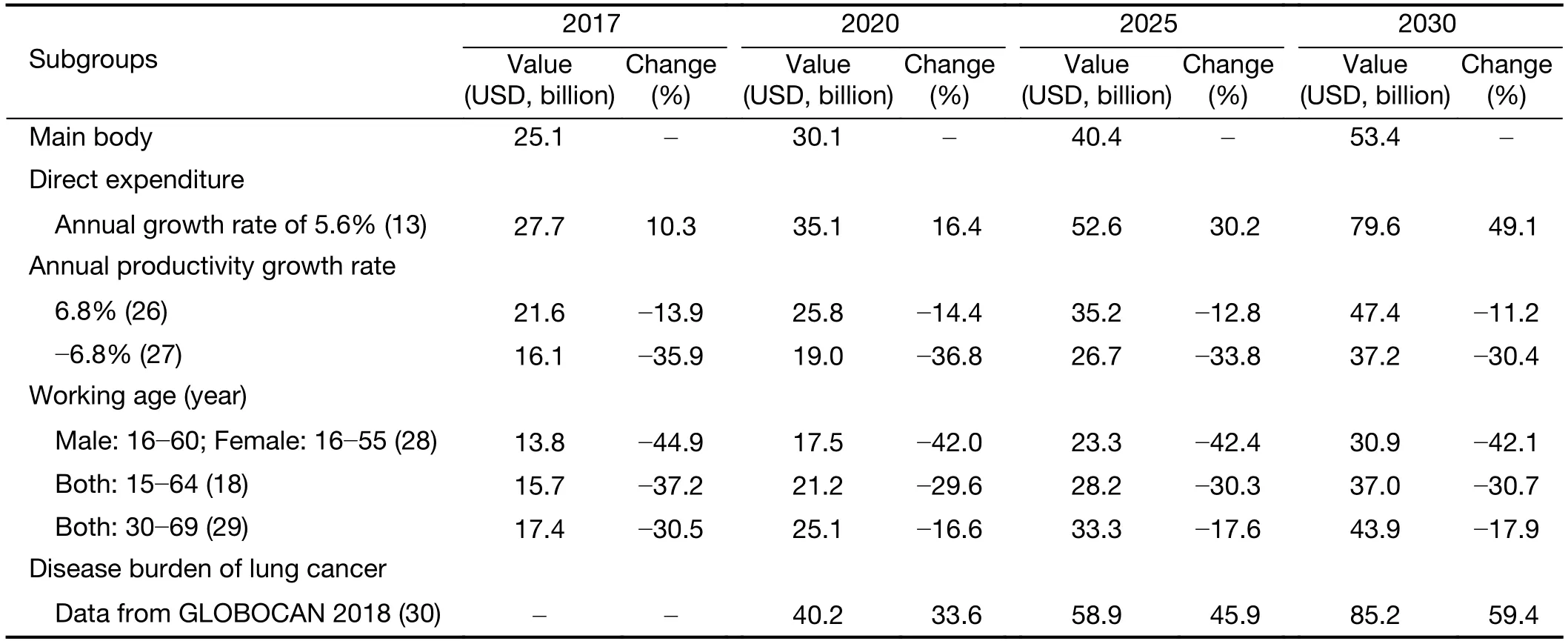
Table 2 Changes in estimated economic burden of lung cancer in China:based on variations in key parameters considered in sensitivity analyses
The contemporary economic burden of lung cancer in China is substantial,up to 0.121% of the local GDP in 2017.If we adopted the GDP from the China Statistical Yearbook (14),it would be 0.205%,equal to 4 times that previously described for the economic consequences of smoking in China (9).Very large differences could be caused by the following factors.Changes in prevalent cases and deaths from lung cancer play an important role.In GBD 2015,the prevalent cases and deaths were 918,794 and 580,020 for China in 2015,respectively (32),while they were as high as 1,271,772 and 692,389 in 2017 based on GBD 2017 due to increases in the disease burden of lung cancer (16),the aging population and comprehensive updates in the data source for GBD.Moreover,an upward trend in expenditure related to treatment could accelerate the growth in the economic burden.
The economic burden of lung cancer varies greatly across countries and regions due to the differences in the disease burden of lung cancer,treatment patterns and healthcare settings (4-8,33,34).For the US,the economic burden of lung cancer was 0.24% of the local GDP in 2018(direct cost:$14.2 billion,indirect cost:$36.1 billion) (33),which was much higher than our estimation.Higher medical cost due to differences in treatment intensity,duration,and supporting care and high labor wages is potential explanations (35).For the EU,the economic burden of lung cancer in 2009 was €18.8 billion,which was up to 0.160% of the local GDP (8).For Korea,the economic burden of lung cancer in 2015 was $19.9 billion,which accounted for 0.139% of the local GDP (7).For Iran,the total burden of lung cancer was only up to 0.03%of the local GDP in 2014 (34).Multiple factors could lead to these variations across countries.Apart from the methodology (34) and types of economic burden (7),differences in the disease burden of lung cancer contribute greatly (16).Based on results from GBD 2017,the number of prevalent cases were 483,923,50,059,7,235,and 1,271,722 for the EU in 2009,Korea in 2015,Iran in 2014,and China in 2017,respectively (16).Moreover,differences in medical and non-medical expenditure caused by treatment patterns could be another contributor.Thus,it is of great significance to estimate the comprehensive economic burden of lung cancer based on Chinese-specific parameters.
The contemporary direct expenditure is very high,amounting to 1.43% of the total healthcare expenditure of China in 2017.Direct expenditure is greatly affected by the disease burden of lung cancer,the range of target population,and the unit of expenditure related to treatment.Based on the Chinese hospital database and assumptions for outpatient payment,Caiet al.estimated the total direct expenditure in 2015,as 0.59% of the total healthcare expenditure,which was lower than our estimation (10).As noted previously,differences in the disease burden of lung cancer could account for most of the gap.Furthermore,patients who were not treated in the hospital during survey time or not seeking treatment in local clinics were not included,which could have resulted in underestimation in the study by Caiet al(10).In addition,our primary survey was conducted among highlevel hospital in each province,while all hospitals with electronic hospital databases were included in the study by Caiet al.(10).Thus,unit medical expenditure in our study might be higher than that in the prior study.
The relative proportions of the direct and indirect economic burden are closely related to prognosis.In our analysis,the indirect burden could account for 55.7% of the total burden,in which the cost of premature death accounted for the majority.The distribution is in accordance with the estimation for lung cancer from the US (36),the United Kingdom (36),and Korea (7).Most lung cancer patients undergo worse survival,with 5 relative survival rates of 19.7% in China (17).Thus,lung cancer could cause more premature death,driving the higher proportions of indirect cost.Improvements in the prognosis of lung cancer could not only prevent death but also bring substantial economic benefits nationally (37).
The economic burden of lung cancer varies across demographic and tumor characteristics,which could be helpful in identifying economically vulnerable cases and guiding policy making in controlling lung cancer.Consistent with distributions of the disease burden of lung cancer,male patients and older patients had a greater burden.Lung cancer patients diagnosed in later stages bore a heavier burden,which was caused by the higher proportions of cases in stages III and IV (63.5%) with worse survival.This issue underscores the importance and promising cost-effectiveness of early detection of lung cancer (38).Consistent with our previous estimation,patients with a smoking history (including current and former smokers) constituted 57.3% of the total economic burden in 2017.Such an enormous health and economic burden caused by smoking highlights the strong tobacco control strategies.
Projections for the future economic burden of lung cancer are essential for policy making in terms of long-term budget making and healthcare resource allocation and have never been performed in China before.Under the context of population aging,urbanization and increased disease burden from lung cancer,it is projected that the economic burden of lung cancer in 2020,2025,and 2030 will be 30.1 billion USD,40.4 billion USD,and 53.4 billion USD,accounting for 0.121%,0.131%,and 0.146% of China’s GDP,respectively.Even without changes in the disease burden of lung cancer in the current projections,population aging and urbanization could strongly drive the economic burden,which is consistent with the US projection (6).On the one hand,this dynamic increasing trend may serve as a reminder for the government that it is urgent to make healthcare budgets with a long-term view,especially in an era with inevitable population aging and rapid urbanization.On the other hand,the findings also emphasize the need to take actions to control and prevent lung cancer and the associated economic burden.
If the goals of lung cancer control and prevention can be achieved,including the SDG 3.4 and Healthy China 2030,the economic burden would decline by 12.6% and 40.3%,respectively.These reductions shed light on the directions we should take in reducing the economic burden.It is imperative that actions be taken to reduce lung cancer morbidity and mortality,including lowering modifiable risk factors,such as smoking,implementing screening programs to find more patients in early stages,and improving clinical practice to prolong patients’ lives.
Medical expenditure plays an important role in the economic burden.As we noted in method,the pattern of unit expenditure is closely related to the healthcare system.In the US,expenditure across the initial,continuing,and end of life periods were shown in“J”shape (6).In Australia,the“J”shape among expenditure across three periods is also observed,and the annual expenditure since the 4th diagnosis decreases substantially (11).In China,data for the expenditure pattern of lung cancer may be scarce.The current estimation pioneered the exploration of expenditure according to the rank of years post-diagnosis and found an“L”shaped pattern.When considering expenditure patterns by period for the US (1,0.21,1.60 for initial,continuing,and end of life periods),the economic burden in China would increase by 14.2%;when considering patterns for Australia (1,0.17 and 0.11 for 1-year,4-year and 5-year post diagnosis),the burden would be reduced by 5.6%.Given the differences in the healthcare system in the US,Australia and China,especially insurance coverage,health care access,and treatment rates,these provisional comparisons provide only preliminary results under varying patterns.More attention should be given to the expenditure pattern of lung cancer across the full disease course in China,as examining this pattern is essential for estimating the economic burden.
Identifying the appropriate age range for the working population is crucial for calculating the indirect economic burden.If we took the age range of 16-60 years for males and 16-55 years for females officially required in China(28),the age range of 15-64 years recommended by OECD(20) or the age ranges applied in a global estimation (29),the economic burden in China both in 2017 and in the future would be reduced considerably.However,according to the definition from National Bureau of Statistics in China,the labor force refers to the population aged above 16 years old with working ability,both employed and unemployed (39).Meanwhile,employment rates from OECD showed that 8.1% of the population over 75 years old were still working (20).It is reasonable to choose a working age above 16 years old and below the sex-specific life expectancy for our main comprehensive estimation.In addition,when we used data on the disease burden of lung cancer in the future from GLOBOCAN 2018,the economic burden was predicted to be higher which reflects the possible underestimation in existing predictions.
As we all know,both the surveys for medical expenditure and non-medical expenditure with work-loss days were the first ones conducted based on multi-center sites,which could provide detailed expenditure information with good representativeness.However,results should be interpreted with caution due to the potential bias caused by participants’ selection and study design.Lung cancer from hospital-based survey is easy to suffer from selection bias due to two reasons.First,patients who sought hospital care were included,neglecting the cases like those who were treated by the outpatient visit.Second,this survey was limited to high-level hospitals,lacking the hospitals at municipal or prefecture level.What is more,information bias,as the nature of retrospective study,occurred as well due to the integrity and accuracy of the medical record systems in surveyed hospitals,or the recall misleading among surveyed participants by face-to-face interview.
Furthermore,our estimates were based on various assumptions and databases that might be dissimilar due to many factors;hence,several limitations are acknowledged.The cited surveys providing original data on expenditure were conducted several years ago,and thus might not represent contemporary expenditure.To reflect the timeeffectiveness,a discount rate of 3% and an annual growth rate in the current analysis were applied in raw expenditure data.Apart from the selection bias and information bias as we stated before (13,15),the limited time period for primary surveys could be another limitation,resulting in difficulties in presenting expenditure or work-loss days across the full disease course.As we noted in the method,the unit medical expenditure in the last 5 years was assumed to be the same.However,medical expenditure among the initial,continuing,and end of life period was in an ‘J’ shape (6,11) in the US and Australia.Thus,the assumptions in our analyses lead to some uncertainties.However,the impact of expenditure patterns from the US and Australia has been quantified in sensitivity analysis.Other limitations in data sources should be acknowledged here as well.For prevalent cases,only total cases could be acquired due to data source limitations.Brief estimation was conducted by use of limited survival rates.Additionally,because of data availability limitations,average earnings were input to estimate the indirect economic burden,thus neglecting wage differences among subgroups.Despite such limitations,our estimation and prediction at the population level can provide direction for health-related policy making.
Conclusions
The economic burden of lung cancer in China in 2017 was substantial and more likely to continue increasing in the future.However,the economic burden can be alleviated via effective lung cancer control and prevention programs.Despite existing limitations,both the current status and projected trend will be essential for policy making regarding cancer prevention and control,as they can assist in shaping healthcare policies to support those who are economically vulnerable individuals and guide budget formulation in the mid-long term.
Acknowledgements
The study was supported by the National Key R&D Program of China (No. 2017YFC0907900,No.2017YFC0907901,No. 2017YFC1308700 and No.2017YFC1308705),and National Natural Science Foundation of China (No.81773521).
Footnote
Conflicts of Interest:The authors have no conflicts of interest to declare.
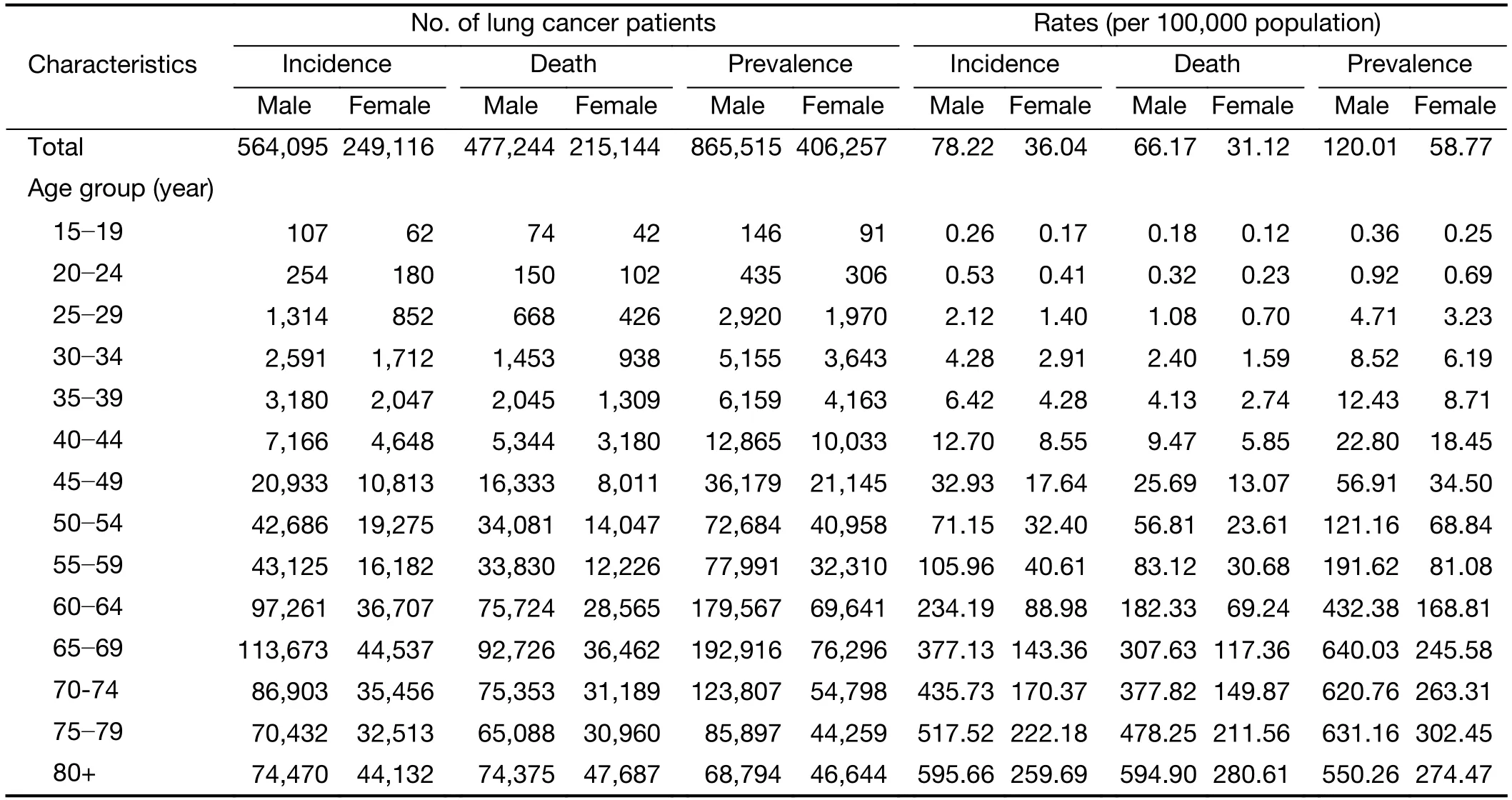
Table S1 Inputting parameters of diseases burden of lung cancer in China in 2017
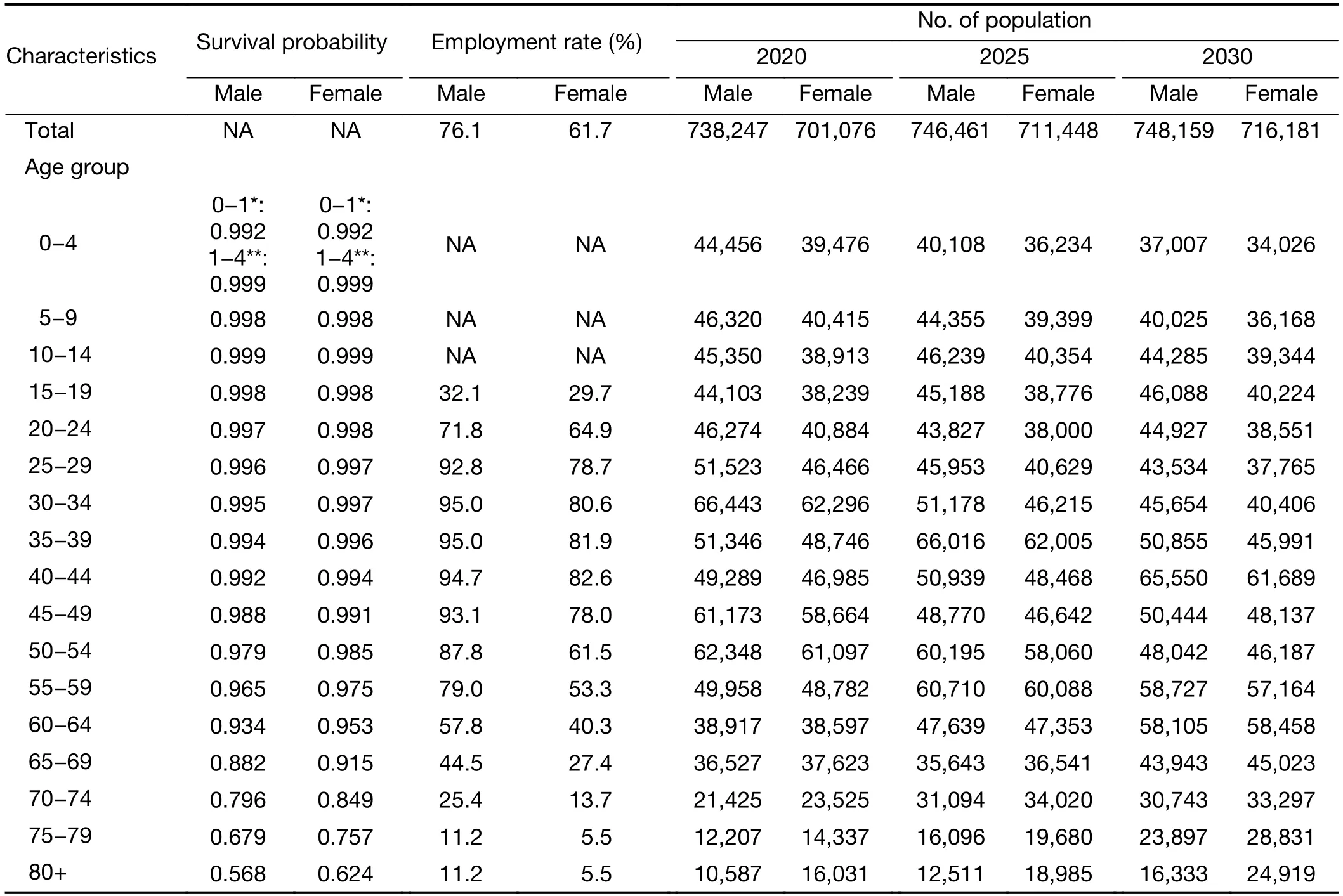
Table S2 Inputting parameters of survival probability,employment rates and number of population in China
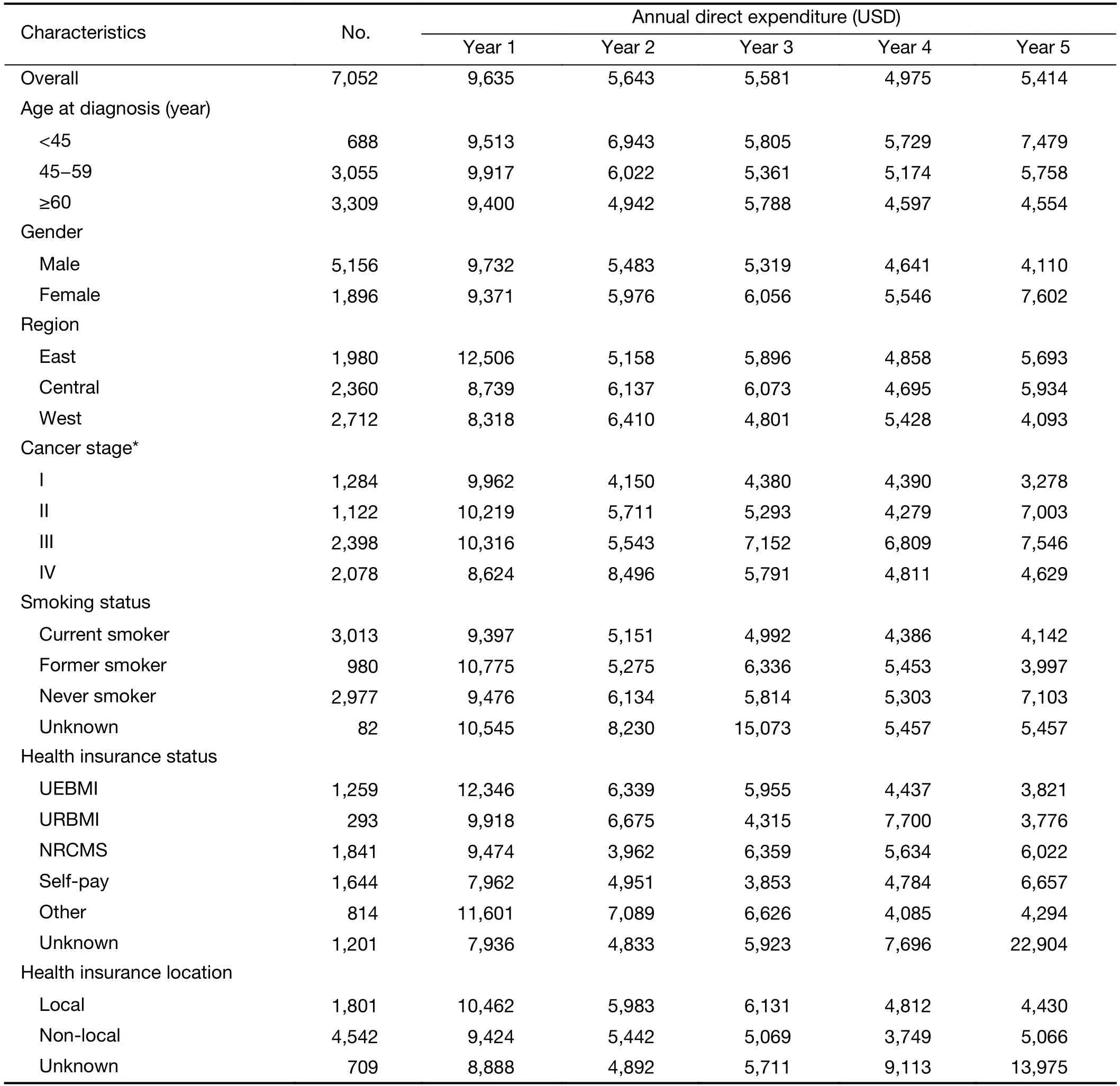
Table S3 Annual direct medical expenditure per lung cancer patient in China in 2017 by year post-diagnosis
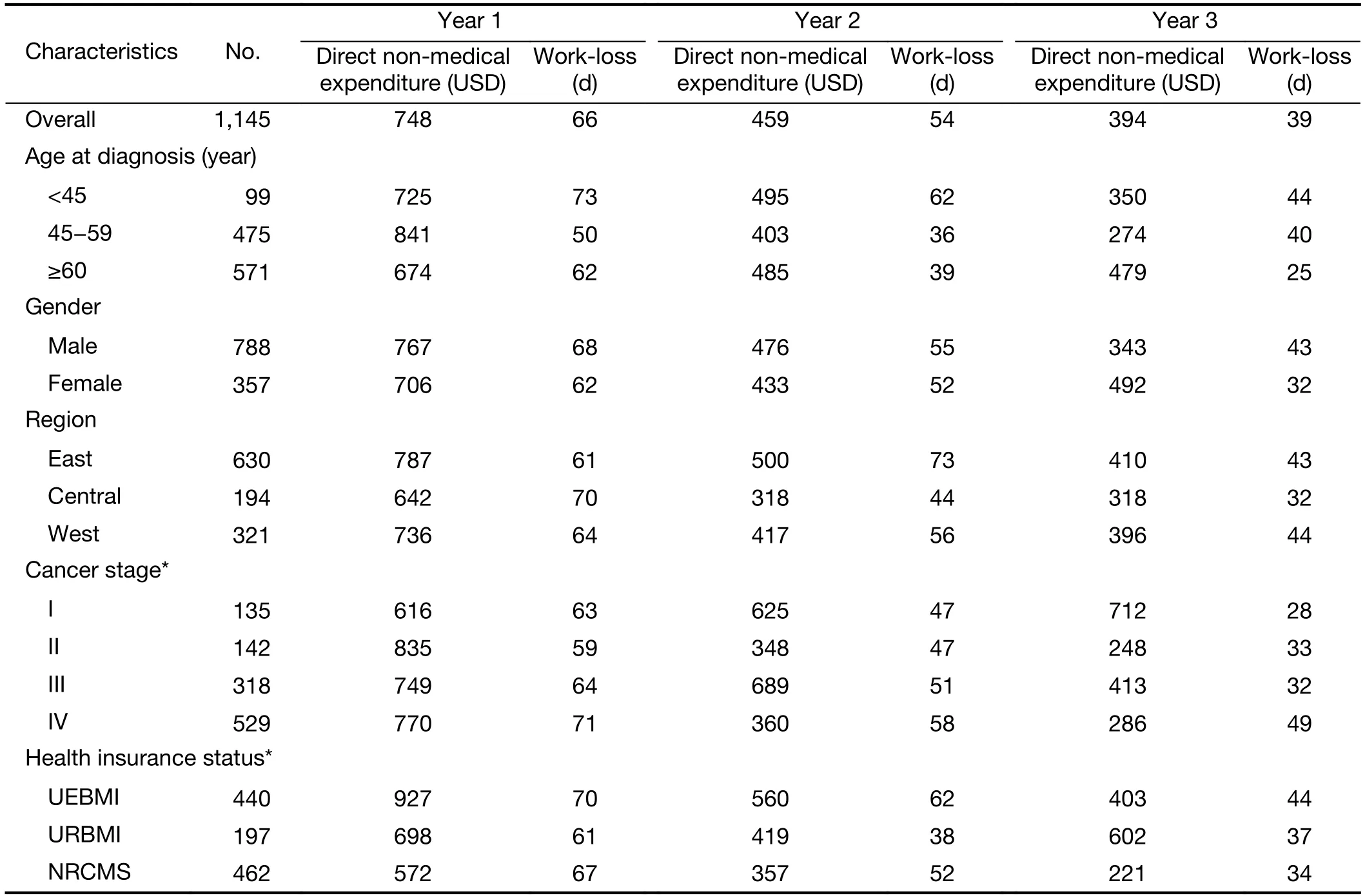
Table S4 Annual direct non-medical expenditure and days of work-loss per lung cancer patient in China in 2017 by year post-diagnosis
杂志排行

Chinese Journal of Cancer Research的其它文章
- Colorectal cancer burden and trends:Comparison between China and major burden countries in the world
- Changing trends of disease burden of gastric cancer in China from 1990 to 2019 and its predictions:Findings from Global Burden of Disease Study
- Clinical characteristics and clinicopathological correlations of bilateral breast cancer in China:A multicenter study from Chinese Society of Breast Surgery (CSBrS-006)
- Multi-center investigation of breast reconstruction after mastectomy from Chinese Society of Breast Surgery:A survey based on 31 tertiary hospitals (CSBrS-004)
- Laparoscopic vs. open surgery for gastrointestinal stromal tumors of esophagogastric junction:A multicenter,retrospective cohort analysis with propensity score weighting
- Radiotherapy combined with nimotuzumab for elderly esophageal cancer patients:A phase II clinical trial