How to do when PFO closure failed under routine guidance:the first clinical experience for PFO closure
2021-03-03YingZHOUJunGangNIE
Ying ZHOU, Jun-Gang NIE
1. Department of Pharmacy, the First Affiliated Hospital of Nanchang University, Nanchang, China; 2. Department of Cardiology, the First Affiliated Hospital of Nanchang University, No.17 Yongwaizhengjie, Donghu District, Nanchang, China
Patent foramen ovale (PFO) is the most common abnormality of fetal origin and is affecting approximately 25% of the worldwide adult population.[1]During the past two decades, instead of surgical closure, catheter-based procedures to close the PFO have become widely used among patients. Periprocedural guidance with fluoroscopy, transesophageal echocardiography (TEE)or intracardiac echocardiography have been the mainstream technique to ensure a safe and successful procedure. However, because of its 2-dimensional (2D) nature, these modalities may be associated with a certain incidence of failure or complication. Herein, we describe an innovative use of 3-dimensional (3D) mapping system to guide the PFO closure which can provide a percutaneous alternative in some patients with a failed PFO closure. We present the following case in accordance with the CARE reporting checklist.
We describe a 53-year-old male patient who was admitted to our department because of limb dyskinesia for half a year. He had a medical history of lacunar infarction, which was being treated with relevant medication. Transthoracic echocardiography (TTE) indicated that he had patent foramen ovale (PFO), accompanying with paroxysmal atrial tachycardia.
PFO closure had been performed for the patient.Since the PFO was a “simple” defect, which was with a short tunnel and without an aneurismal atrial septum, the closure procedure was performed under fluoroscopy guidance as this would obviate the need for general anesthesia. While, the J-tipped guide wire could not across the PFO tunnel into the left atrium because the foramen ovale was tough and the PFO tunnel was short.
Considering that under three-dimensional (3D)mapping system guidance, the foramen ovale can be accurately located, and even the atrial septum can be passed across without X-ray exposure, we decided to apply 3D mapping system (EnSite Velocity 5.0, St. Jude Medical) to guide PFO closure. The catheter was introduced and placed in target position under 3D mapping system guidance. The 3D geometry of the right atrium and proximal coronary sinus was obtained with ablation catheter and then the foramen ovale was accurately located (Figure 1A,purple arrow). Since the PFO tunnel was tough and short, a conventional 4 mm tip ablation catheter could not across the foramen ovale. Therefore, we tried to use steerable decapolar catheter (IBI-AFocusIITM& OptimaTM, St. Jude Medical), which was more supportive to guide the delivery sheath into the left atrium (Figure 1B and C). When the device was adequately placed, which was confirmed with echocardiography and fluoroscopy, the left atrial disc was deployed, followed by the right disc. The occluder had been released successfully (Figure 1D,white arrow).
The patient underwent a successful PFO closure under the 3D mapping system guidance. In the following 12 months, the patient had no further symptom of limb dyskinesia and no recurrence of lacunar infarction.
Percutaneous closure of PFO in patients with cryptogenic stroke has been undertaken for years.[2,3]For the majority of patients, periprocedural guidance with fluoroscopy, transesophageal echocardiography (TEE) or intracardiac echocardiography is required to ensure a safe and successful procedure.[4]For a “simple” defect, device closure under fluoroscopy may be better. For a “complex” defect, for example with a long apparent tunnel or an atrial septal aneurysm, then intracardiac echocardiography (ICE) or TEE would be better.[5]
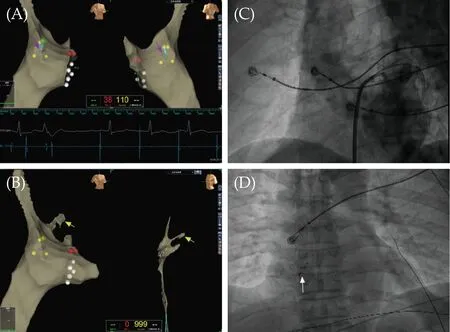
Figure 1 PFO closure guided by 3D mapping system. (A):Electrographically defined foramen ovale on the 3D electroanatomic mapping. The yellow tags encircle the electrographically defined foramen ovale; the grey tags indicate the central foramen ovale (purple arrow). (B): Catheter crossing PFO into the left atrium under 3D mapping system guidance (yellow arrow). (C):Angiographic analysis confirming that the catheter enters the left atrium. (D): The device is shown in place after release (white arrow). PFO: patent foramen ovale.
Although echocardiography (ICE or TEE) allows more precise localization of foramen ovale and provides real-time, direct visualization of the procedure for PFO closure, a few limitations prevent these modalities from routine use, including 2D visualization, patients’ intolerance, and high cost.What is more, the modality does not increase the support for the guidewire when it passes through the PFO tunnel which is tough and short.
At present, electrophysiological procedures under 3D mapping system guidance such as radiofrequency catheter ablation are often used clinically.However, the use of 3D mapping system guidance for PFO closure has not been reported. Under the 3D mapping system guidance, the foramen ovale can be accurately located, and the catheter can also be displayed in a 3D manner so as to be accurately adjusted to cross the foramen ovale. We are reporting on the first clinical experience for the application of 3D mapping system to guide PFO closure,which is a good choice for patients with difficulty in PFO closure. This strategy might provide a percutaneous alternative in some patients with a failed PFO closure. In our case, we also describe an innovative use of 3D mapping system which is more accurate and supportive to guide the PFO closure.
ACKNOWLEDGMENTS
This work was supported by the National Natural Science Foundation of China (No. 81 903 724). The authors have no conflicts of interest to declare.
杂志排行

Journal of Geriatric Cardiology的其它文章
- Journal of Geriatric Cardiology
- Potassium variability during hospitalization and outcomes after discharge in patients with acute myocardial infarction
- Beta-blocker therapy in elderly patients with renal dysfunction and heart failure
- Obstructive sleep apnea increases heart rhythm disorders and worsens subsequent outcomes in elderly patients with subacute myocardial infarction
- Sex modification of the association of the radial augmentation index and incident hypertension in a Chinese communitybased population
- Neurohumoral, cardiac and inflammatory markers in the evaluation of heart failure severity and progression